Terminal Syme Procedure: Surgical Technique & Outcomes
Key Takeaway
The terminal Syme procedure, or Thompson-Terwilliger amputation, involves the en bloc excision of the distal half of the distal phalanx, including the nail plate, matrix, and nail folds. It is primarily indicated for recalcitrant, recurrent infected ingrown toenails or distal phalangeal tumors. Meticulous surgical technique is required to prevent nail spicule recurrence, ensuring a highly functional and cosmetically acceptable outcome for the patient.
Introduction to the Terminal Syme Procedure
The terminal Syme procedure, historically referred to as the Thompson-Terwilliger procedure, is a highly reliable, definitive surgical intervention for recalcitrant pathology of the distal toe. The procedure involves the en bloc amputation of the distal half of the distal phalanx, which inherently includes the complete excision of the nail plate, the germinal and sterile matrices, the lateral and proximal nail folds, and the underlying osseous bed upon which these structures rest.
Named for its conceptual similarity to the classic Syme amputation of the ankle—wherein a robust plantar soft-tissue flap is advanced dorsally to provide a durable, weight-bearing stump—the terminal Syme procedure applies this exact biomechanical principle to the distal phalanx. By utilizing the thick, specialized glabrous skin of the plantar toe pad to cover the dorsal defect, the surgeon creates a resilient, pain-free terminal digit.
While often viewed as a procedure of last resort for benign nail pathology, it remains an indispensable technique in the orthopedic surgeon’s armamentarium, offering definitive resolution for patients who have exhausted less extensive conservative and surgical options.
Indications and Patient Selection
The decision to proceed with a terminal Syme amputation must be carefully weighed against the functional and cosmetic alterations it produces. Patient selection is paramount to achieving high satisfaction rates.
Primary Indications
- Recalcitrant Onychocryptosis (Ingrown Toenail): The most common indication is recurrent, severe bouts of infected ingrown toenails that have failed multiple less invasive procedures (e.g., partial nail avulsion with phenol matrixectomy, wedge resections).
- Subungual and Distal Phalangeal Neoplasms: The procedure is an excellent oncologic or excisional approach for various bone or soft tissue tumors localized to the nail unit and distal phalanx. Examples include glomus tumors, subungual exostoses, enchondromas, osteochondromas, and early-stage localized malignancies (e.g., subungual melanoma in situ or squamous cell carcinoma), provided adequate margins can be obtained.
- Chronic Osteomyelitis: Localized chronic osteomyelitis of the distal phalanx tip, often a sequela of neglected paronychia or diabetic foot ulcerations, where proximal bone stock is viable.
- Severe Macrodactyly or Congenital Deformities: Occasionally utilized to debulk and shorten a severely hypertrophic distal digit.
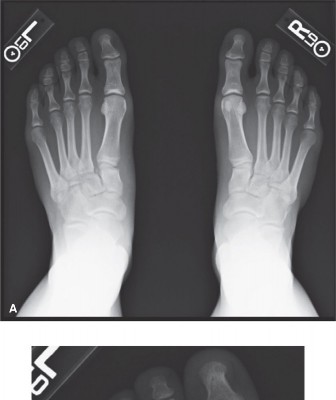
Severe Nail Incurvatum
In cases of severe nail incurvatum (pincer nail deformity), the nail plate is usually narrow and highly convex.

FIGURE 87-23 Incurvatum of nail.
While a terminal Syme procedure is definitive for incurvatum, alternative procedures such as isolated nail fold excision without concomitant nail plate or matrix removal have been described. Literature suggests that nail fold excision alone can yield zero recurrences in select cohorts. However, for severe incurvatum where the nail plate is already narrow, further reduction in size via standard nail plate procedures might yield a cosmetically displeasing result, making the terminal Syme a viable, albeit aggressive, alternative.
🛑 Surgical Warning: Active Infection
In the presence of an acute abscess or fluctuant paronychia, the terminal Syme procedure must be delayed. Immediate amputation through an actively infected field significantly increases the risk of postoperative osteomyelitis of the remaining phalangeal base and wound dehiscence.
Protocol: Institute incision and drainage first. Prescribe appropriate culture-directed oral antibiotics and implement daily warm soaks to improve the local wound condition. The definitive terminal Syme procedure should be performed once the acute cellulitis and purulence have resolved—typically a delay of less than 2 weeks.
Clinical Anatomy and Biomechanics
A profound understanding of the distal toe anatomy is required to execute this procedure without compromising the functional integrity of the digit.
- The Nail Matrix: The germinal matrix extends significantly proximal to the visible eponychium (cuticle). Failure to resect this proximal extension is the primary cause of postoperative nail spicules (horns).
- Tendon Insertions: The Extensor Hallucis Longus (EHL) inserts onto the dorsal base of the distal phalanx, while the Flexor Hallucis Longus (FHL) inserts onto the broad plantar base. The terminal Syme procedure mandates transection of the distal phalanx distal to these insertions (typically 1 to 2 mm distal to the metaphyseal flare). Preserving these insertions is critical; failure to do so results in a flail distal interphalangeal (DIP) joint, leading to instability, altered gait biomechanics, and potential hammer toe deformity.
- Neurovascular Supply: The proper plantar digital arteries and nerves arborize extensively in the plantar pad. The surgical approach must respect this plantar flap, ensuring it remains robustly vascularized to survive the dorsal transposition.
Surgical Technique (Step-by-Step)
Meticulous technique and obsessive attention to detail are mandatory. The primary goal is to remove the matrix, nail, and bone in a single, en bloc specimen to virtually eliminate the chance of troublesome nail recurrence.
1. Anesthesia and Positioning
The procedure is typically performed under a digital block using a long-acting local anesthetic (e.g., 0.5% bupivacaine without epinephrine) combined with a shorter-acting agent (e.g., 1% lidocaine). The patient is positioned supine.
💡 Clinical Pearl: Tourniquet Use
Historically, Thompson and Terwilliger did not encourage the use of a tourniquet, fearing ischemic compromise to the plantar flap. However, modern orthopedic consensus strongly recommends the use of a sterile digital tourniquet (e.g., a Penrose drain or commercial digital ring). A bloodless field allows for highly precise dissection, reduces the chance of iatrogenic injury to the proper plantar digital nerves at the proximal extent of the dissection, and aids in identifying small vessels for targeted electrocautery, thereby drastically reducing the risk of postoperative hematoma.
2. Incision Planning
The design of the elliptical incision is the most critical step in preventing recurrence and ensuring adequate soft-tissue coverage.
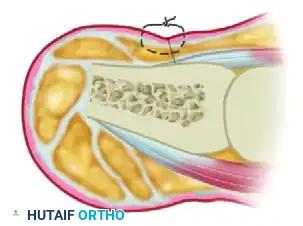
FIGURE 87-25A Skin incision (Dorsal View).

FIGURE 87-25B Skin incision (Lateral View).
- Proximal Margin: While original descriptions recommended a 4 mm proximal margin, the germinal matrix frequently extends further. It is highly recommended that the proximal skin margin measure 6 to 7 mm proximal to the cuticle. This ensures complete matrix removal. Because the extrinsic tendon insertions (EHL/FHL) lie proximal to this point, this margin is safe. Furthermore, the plantar flap is inherently long enough to reach this dorsal proximal margin without undue tension.
- Distal Margin: A skin margin of 2 to 3 mm distal to the hyponychium is sufficient to clear the distal sterile matrix.
3. Dissection and En Bloc Resection
Use sharp dissection throughout the procedure, reserving bone cutters or a microsaw strictly for the osseous transection.
- Initial Incision: Make the dorsal incision straight down to the bone proximally. On the lateral and medial aspects, do not bevel the scalpel blade toward the center of the phalanx until you have passed plantar to the lateral flares of the bone. Beveling too early risks leaving lateral matrix horns behind.
- Plantar Flap Elevation: Using a robust clamp (e.g., a Kocher or towel clip), firmly grasp the distal aspect of the phalanx (including the nail plate).
- Retrograde Dissection: With skin hooks gently retracting the plantar flap to avoid crush injury to the skin edges, continue sharp dissection along the plantar surface of the phalanx in a distal-to-proximal direction. Stay directly on the periosteum to maximize the thickness and vascularity of the plantar flap.
- Bone Transection: Identify the metaphyseal flare of the distal phalanx. Transect the distal phalanx 1 to 2 mm distal to the EHL and FHL insertions using a sharp bone cutter, oscillating microsaw, or rongeur.
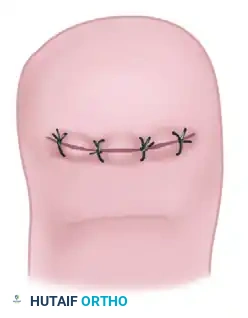
FIGURE 87-25C Removal of distal half of phalanx.
- Completion of Amputation: Release any remaining soft tissue attachments to complete the en bloc amputation of the distal phalanx, nail bed, and matrix.
- Bone Contouring: Inspect the remaining proximal stump of the distal phalanx. Use a rongeur or rasp to meticulously smooth any sharp irregularities or bony prominences that could cause pressure necrosis against the plantar flap.
4. Hemostasis and Closure
Before closure, deflate the digital tourniquet to assess perfusion and achieve strict hemostasis. Use bipolar electrocautery sparingly to address specific bleeders, avoiding widespread thermal damage to the flap.
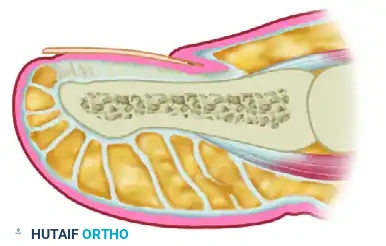
FIGURE 87-25D Closure.
- Advance the plantar flap dorsally over the contoured bone stump.
- Close the wound using interrupted, nonabsorbable sutures (e.g., 4-0 or 3-0 Nylon/Prolene).
🛑 Pitfall: Trimming the "Dog Ears"
As the broad plantar flap is sutured to the narrower dorsal skin margin, medial and lateral "dog ears" will inevitably form. Do not trim these dog ears. Excision of these tissue redundancies severely compromises the vascular supply to the distal flap, risking partial or complete flap necrosis. These dog ears will remodel and flatten out naturally over several months as the scar matures.
Postoperative Care and Rehabilitation
A strict postoperative protocol ensures flap survival and minimizes complications.
- Immediate Post-Op (0-48 Hours): The foot must be strictly elevated above the level of the heart for the first 48 hours to minimize edema, throbbing pain, and venous congestion of the flap.
- Weight-Bearing Status: The patient is allowed to ambulate for essential activities in a rigid, wooden-soled, or firm-soled postoperative shoe with an open toe box. This prevents any dorsal pressure on the healing flap.
- Wound Care: The initial bulky compressive dressing is typically changed at 3 to 5 days postoperatively.
- Suture Removal: Sutures are left in place longer than standard skin closures due to the tension and thickness of the plantar flap. Remove sutures at 14 to 16 days postoperatively.
- Return to Footwear: Once sutures are removed and the incision is stable, the patient can usually transition into a wide toe box shoe (e.g., a deep athletic shoe) within the following week.
Complications and Management
While the terminal Syme procedure is highly dependable, complications can arise, primarily stemming from technical errors during execution.
- Troublesome Nail Spicules (Horns): The most common and frustrating complication. This occurs due to incomplete excision of the extreme proximal or lateral margins of the germinal matrix. Management requires a revision surgery to excise the retained matrix tissue. Prevention via the 6-7 mm proximal margin is the best cure.
- Epidermal Inclusion Cysts: These can form along the suture line if epidermal elements are buried during closure. They present as painful, slowly enlarging nodules months after surgery and require simple surgical excision.
- Osteomyelitis of the Distal Phalanx: Usually results from operating in the presence of an active, undrained abscess, or from marginal flap necrosis leading to bone exposure. Requires aggressive debridement, potential further bone resection, and culture-directed antibiotics.
- Flap Necrosis: Caused by excessive tourniquet time, aggressive electrocautery, or trimming of the dog ears. Superficial epidermolysis can be managed with local wound care; full-thickness necrosis requires debridement and healing by secondary intention or skin grafting.
Cosmetic and Functional Outcomes
Preoperative patient counseling regarding the final cosmetic appearance is essential.

FIGURE 87-24 Result after terminal Syme procedure.
Initially, the tip of the toe will appear bulbous, shortened, and aesthetically unattractive due to postoperative edema and the presence of the lateral dog ears. However, over a period of 6 to 12 months, the soft tissues undergo significant remodeling. The dog ears flatten, and the plantar pad conforms to the underlying bone.
In vast clinical experience, the final appearance is rarely offensive to the patient. More importantly, the procedure produces an excellent functional result. By eliminating the source of chronic pain and recurrent infection, patients are able to return to normal footwear and unrestricted weight-bearing activities, making the terminal Syme procedure a highly successful and definitive orthopedic intervention.
You Might Also Like