Partial Resection of the 5th Metatarsal Head: Surgical Guide
Key Takeaway
Partial resection of the lateral condyle of the fifth metatarsal head is a highly effective procedure for symptomatic bunionette deformities. This technique relieves lateral pressure and accommodates standard footwear. Success relies on precise resection limits—typically 35% to 40% of the articular surface—and meticulous preservation of the abductor digiti minimi insertion to prevent medial toe subluxation. Proper patient selection and capsular imbrication are critical for optimal outcomes.
INTRODUCTION AND PATHOMECHANICS
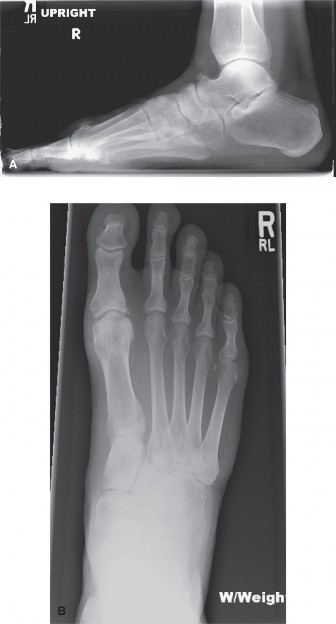
Partial resection of the lateral condyle of the fifth metatarsal head, commonly referred to as a bunionette excision or condylectomy, remains one of the most frequently utilized procedures in forefoot reconstructive surgery. The bunionette, or "Tailor’s bunion," is characterized by a painful bony prominence on the lateral aspect of the fifth metatarsophalangeal (MTP) joint. This deformity often results from a combination of lateral bowing of the fifth metatarsal shaft, an enlarged lateral condyle, or an abnormally wide fourth-to-fifth intermetatarsal angle (IMA).
The primary objective of a partial condylar resection is to relieve pressure symptoms caused by footwear impingement, thereby allowing the patient to tolerate a slightly greater variety of shoe wear. While the procedure is highly effective for pain relief, it is imperative to understand its biomechanical limitations. It does not correct the underlying angular deformity of the metatarsal shaft. Consequently, meticulous patient selection and precise surgical execution are required to prevent complications such as under-resection, joint instability, or iatrogenic deformity.
INDICATIONS AND PATIENT SELECTION
The decision to perform a partial resection of the lateral condyle rather than a corrective osteotomy hinges on the specific pathoanatomy of the patient's foot.
Primary Indications
- Symptomatic Lateral Prominence: Patients presenting with localized pain, erythema, and bursa formation directly over the lateral condyle of the fifth metatarsal head that has failed conservative management (e.g., shoe modification, padding, NSAIDs).
- Normal Intermetatarsal Angle: Patients with a normal or only mildly elevated 4-5 IMA (typically less than 8 degrees) where the primary pathology is localized hypertrophy of the lateral condyle (Type I bunionette).
Contraindications and Caveats
- Severe Forefoot Splaying: In cases of significant forefoot splaying with a severely widened 4-5 IMA, a simple exostectomy will fail to narrow the forefoot adequately, leading to recurrent symptoms.
- Intractable Plantar Keratosis (IPK): The presence of a painful plantar keratosis beneath the fifth metatarsal head suggests significant plantarflexion of the metatarsal. While a plantar condylectomy can be added to the lateral resection, a true IPK strongly suggests that a corrective elevating osteotomy of the fifth metatarsal is necessary for satisfactory and durable correction.
💡 Clinical Pearl: Preoperative Counseling
The cosmetic correction achieved by a simple condylectomy is not always pleasing to the patient. Causes of dissatisfaction often stem from a misunderstanding of the procedure's goals. The patient must be explicitly warned before surgery that only the painful bony prominence will be removed and that the overall width of the forefoot will not be altered appreciably. Managing cosmetic expectations is as critical as the surgical execution.
SURGICAL ANATOMY
A thorough understanding of the lateral forefoot anatomy is non-negotiable to avoid devastating iatrogenic complications, particularly nerve injury and joint destabilization.
- Neurological Structures: The surgical approach places two primary nerves at risk. Dorsally, the dorsolateral cutaneous branch of the sural nerve courses over the lateral aspect of the fifth metatarsal. Plantarward, the proper digital branch of the lateral plantar nerve to the fifth toe must be protected.
- Musculotendinous Structures: The tendon of insertion of the abductor digiti minimi (ADM) is the most critical dynamic stabilizer of the fifth MTP joint. It passes just plantar to the midline of the lateral aspect of the fifth metatarsal head, inserting onto the plantar-lateral base of the proximal phalanx.
- Ligamentous Structures: The lateral collateral ligament originates on the lateral condyle of the metatarsal head. Resection of the condyle inherently removes the origin of this ligament, necessitating meticulous capsular repair to restore static stability.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Positioning and Anesthesia
The patient is placed in the supine position on the operating table. A small bump may be placed under the ipsilateral hip to internally rotate the leg slightly, bringing the lateral border of the foot into a direct, accessible view. The procedure is typically performed under regional anesthesia (ankle block or popliteal block) with intravenous sedation. A calf or ankle tourniquet is applied to ensure a bloodless surgical field.
2. Incision and Exposure
The preferred approach is a straight lateral incision, though a dorsolateral incision may also be utilized depending on surgeon preference and local skin conditions.
- Make a straight lateral incision extending from the junction of the middle and distal thirds of the fifth metatarsal shaft, carrying it distally to the midshaft of the proximal phalanx.

- Incise only the skin initially. Deepening the incision too rapidly risks transecting the delicate subcutaneous nerves.

- If a dorsolateral incision is used, meticulously identify and retract the dorsolateral cutaneous branch of the sural nerve.
- When utilizing the preferred straight lateral incision, the dissection plane must pass safely between the sural nerve branch (located dorsally) and the proper digital branch of the lateral plantar nerve (located plantarward).
3. Capsulotomy and Soft Tissue Preservation
The approach to the joint capsule is the most critical step in preventing postoperative toe deformity.
⚠️ Surgical Warning: Preserving the Abductor Digiti Minimi
The tendon of insertion of the abductor digiti minimi passes just plantar to the midline of the lateral aspect of the fifth metatarsal head. If the periosteal and capsular incision is made exactly on the midline or plantar to it, this tendon will be transected. The capsular incision must be made in a straight line 2 to 3 mm dorsal to the midline. Preservation of this tendon is absolute; if lost, the fifth toe will inevitably subluxate or dislocate medially.
- Following the 2 to 3 mm dorsal offset rule, incise the capsule and periosteum longitudinally.
- By sharp dissection, elevate the capsule dorsally and plantarward.
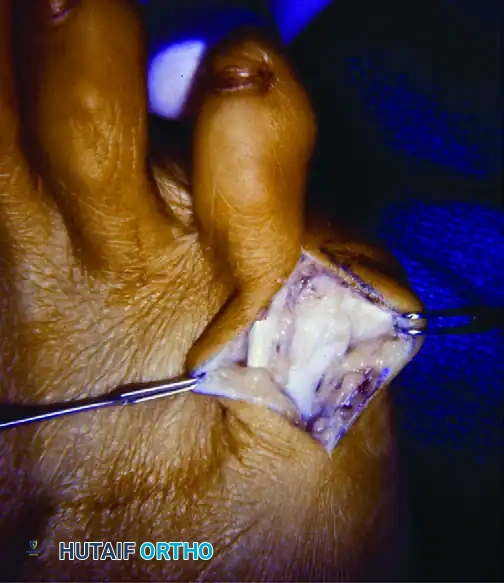
- Deliver the fifth metatarsal head laterally into the wound while simultaneously pushing the proximal phalanx medially.
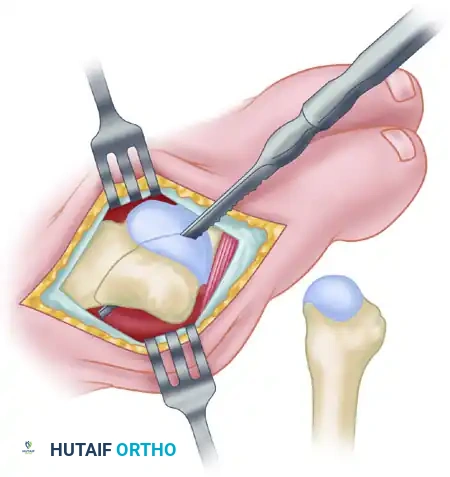
- Crucial Step: You must expose the medial edge of the articular cartilage. Failure to visualize the entire articular surface often leads to optical illusions regarding the size of the metatarsal head, resulting in over-resection.
4. Osteotomy and Condylar Resection
The goal is to remove the hypertrophic lateral eminence without compromising the weight-bearing capacity of the metatarsal head or destabilizing the joint.
- Approximately 35% to 40% of the metatarsal head is usually removed to adequately excise the bony prominence.
- Use a thin osteotome or a small sagittal blade on a power saw. A thick blade will remove too much bone stock and generate excessive thermal necrosis.
- Score the proximal margin of the proposed osteotomy at the metaphyseal flare.
- Direct the saw cut in a dorsal distal-to-plantar proximal direction. This oblique orientation ensures a smooth transition at the metaphyseal-diaphyseal junction and prevents a sharp bony step-off that could cause recurrent lateral pressure symptoms.
5. Addressing the Phalanx and Plantar Condyle
Once the metatarsal resection is complete, attention must be turned to the adjacent structures to ensure a comprehensive decompression.
- Reduce the proximal phalanx over the remaining portion of the fifth metatarsal head.
- Palpate the lateral flare of the base of the proximal phalanx. If this flare produces a projecting bony prominence that may cause persistent symptoms or rub against the fourth toe, excise the prominence with a rongeur or bone-biter. This is performed in the same manner as treating a web corn medially.
- Evaluate the plantar aspect of the metatarsal head. If a plantar callus coexists beneath the metatarsal head, use a rasp or saw to smooth the plantar projection of the condyle flush with the shaft. (Note: As mentioned, severe plantar keratosis may require an osteotomy, but mild callosities can be managed with plantar condylectomy).
- Before proceeding to closure, meticulously round off all remaining bone edges with a bone rasp to prevent soft tissue irritation.
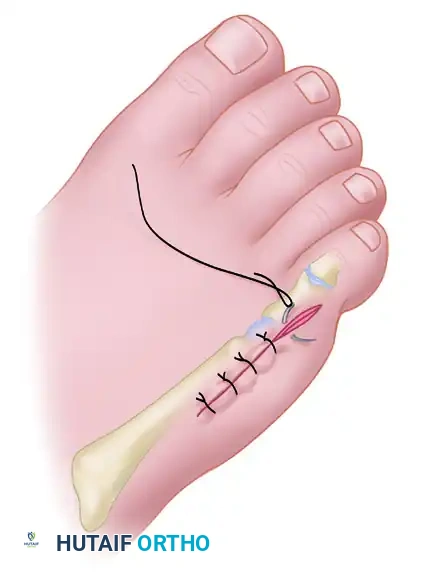
6. Capsular Imbrication and Closure
Because the partial resection inherently removes the origin of the lateral collateral ligament, the joint is rendered temporarily unstable. The closure is not merely an anatomical reapproximation; it is a reconstructive stabilization step.
- An imbricating (pants-over-vest) capsular closure is imperative to restore lateral tension and prevent medial drift of the digit.
- Ensure that the abductor digiti minimi insertion remains securely attached and is incorporated into the plantar leaf of the capsular repair.
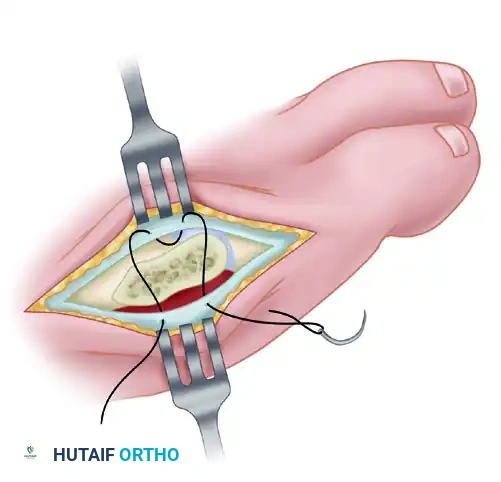
- Use strong, absorbable sutures (e.g., 2-0 or 3-0 Vicryl) for the capsular imbrication. The assistant should hold the fifth toe in slight abduction and neutral dorsiflexion/plantarflexion while the sutures are tied to set the appropriate tension.
- Close the skin with interrupted, nonabsorbable sutures (e.g., 4-0 Nylon or Prolene).

COMPLICATIONS AND PITFALLS
While technically straightforward, partial resection of the fifth metatarsal head carries specific risks that can lead to significant patient morbidity if not carefully avoided.
Medial Subluxation or Dislocation
This is the most dreaded complication of a simple bunionette excision. It occurs due to the iatrogenic transection of the abductor digiti minimi tendon or failure to perform an adequate imbricating capsular closure after removing the lateral collateral ligament origin. The unopposed pull of the medial capsule and adductor structures pulls the toe into a severe varus deformity, often overlapping the fourth toe.

Inadequate Resection
Failure to remove the recommended 35% to 40% of the metatarsal head, or failure to smooth the proximal metaphyseal flare, will result in persistent lateral pressure symptoms. The patient will continue to experience pain in closed shoes, necessitating revision surgery.
Over-Resection and Avascular Necrosis
Conversely, resecting more than 50% of the metatarsal head can compromise the articular congruity, leading to joint subluxation, stiffness, and potentially avascular necrosis of the remaining fragment. This underscores the importance of fully exposing the medial articular cartilage before making the saw cut.
Forefoot Splaying
As noted in the indications, performing this procedure on a patient with a severely widened 4-5 IMA will result in failure. The underlying structural splaying will persist, and the lateral soft tissues will continue to be subjected to high friction forces against footwear.
POSTOPERATIVE CARE PROTOCOL
A structured postoperative rehabilitation protocol is essential to protect the capsular repair while promoting early mobility.
- Immediate Postoperative Phase (Days 1-14):
- The foot is placed in a bulky, compressive dressing.
- Crucially, the dressing must be applied to hold the fifth toe in slight abduction. This releases tension on the lateral capsular repair and prevents medial drift.
- Bathroom privileges and weight-bearing to tolerance are allowed starting on the first postoperative day.
- The patient must wear a firm-soled postoperative shoe with an open toe box to accommodate the dressing and prevent forefoot compression.
- Two-Week Milestone:
- The patient returns to the clinic for wound inspection.
- Skin sutures are removed at 2 weeks.
- A soft toe spacer (silicone or foam) is placed in the fourth web space. This spacer acts as a mechanical block to prevent medial deviation of the fifth toe, thereby protecting the healing lateral capsular repair from strain.
- Weeks 2 to 6:
- The patient continues to use the fourth web space spacer for an additional 4 weeks.
- Weight-bearing continues in a wide, supportive athletic shoe or the postoperative shoe, depending on swelling.
- Six-Week Milestone and Beyond:
- At 6 weeks postoperative, the capsular repair is generally stable enough to withstand normal physiological loads.
-
The patient is allowed to transition into fashionable shoes as tolerated, though wide toe-box footwear is encouraged long-term to prevent recurrence of lateral friction syndromes. Full resolution of postoperative edema may take 3 to 6 months.
You Might Also Like