Accessory Navicular: Comprehensive Surgical Management and the Kidner Procedure
Key Takeaway
The accessory navicular is a common congenital ossicle present in up to 14% of the population. While often asymptomatic, disruption of its synchondrosis can lead to debilitating medial foot pain and posterior tibial tendon dysfunction. Surgical management, primarily the Kidner procedure, involves excision of the ossicle and advancement of the posterior tibial tendon. This guide details the indications, biomechanics, and operative techniques for managing the symptomatic accessory navicular and associated pes planus.
Introduction to the Accessory Navicular
The inclusion of the accessory navicular (also referred to as the prehallux or os tibiale externum) in the discussion of surgical treatment for symptomatic congenital pes planus is driven more by historical convention than by modern biomechanical conviction. First described extensively in the early 20th century, the accessory navicular is a secondary center of ossification that fails to unite with the primary navicular bone during childhood development.
Epidemiological studies, notably those by Geist, demonstrate that 10% to 14% of normal feet possess an accessory navicular. Because the vast majority of these individuals maintain a normal medial longitudinal arch and remain entirely asymptomatic throughout their lives, the direct cause-and-effect relationship between the mere presence of an accessory navicular and the development of structural pes planus remains highly doubtful. However, when symptoms do arise—typically manifesting as medial midfoot pain, localized swelling, and posterior tibial tendon (PTT) dysfunction—they are directly related to the presence of this accessory ossicle and the disruption of its cartilaginous synchondrosis.
In an attempt to evaluate the inheritance pattern of the accessory navicular bone, Kiter et al. evaluated familial inheritance patterns and concluded that the presence of an accessory navicular bone is likely an autosomal dominant trait with incomplete penetrance.
Biomechanics and Pathophysiology
In 1929, Kidner postulated that the support offered to the medial longitudinal arch by the posterior tibial tendon was fundamentally compromised by its abnormal insertion into the accessory navicular. He theorized that this abnormal insertion altered the vector of pull, diminishing the tendon's suspensory function and leading to arch collapse. He subsequently devised a procedure intended to correct this loss of suspension by excising the ossicle and rerouting the tendon.
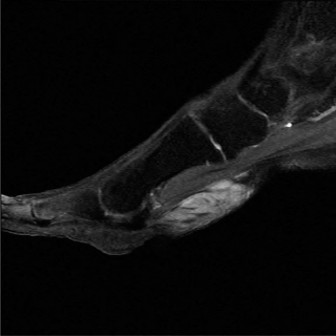
Modern advanced imaging has provided deeper insights into this anatomical variant. In 1999, Kiter et al. evaluated the insertion of the posterior tibial tendon via MRI in 27 feet with an accessory navicular bone and compared them to 22 normal feet. They noted significant abnormalities in the insertion of the posterior tibial tendon in the presence of an accessory navicular. Specifically, the tendon inserted directly into the accessory navicular bone without any continuity to the plantar aspect of the foot.
These findings were further corroborated in 2000 when Kiter et al. examined 13 additional feet, confirming that the posterior tibial tendon inserted directly into the accessory navicular without extending to the sole. Furthermore, a separate, distinct part of the posterior tibial tendon originated from the accessory navicular and extended to the normal plantar insertions, but these two parts did not connect. They concluded that this abnormal, discontinuous anatomy may play a significant role in the development of pes planus in a subset of patients.
Clinical Pearl: Any improvement in the medial longitudinal arch observed after a Kidner procedure in pediatric patients is likely attributable to continued skeletal growth and dynamic stabilization in the immature foot, rather than the mechanical rerouting of the tendon itself.
In adults, Chen et al. described the degeneration of the accessory navicular synchondrosis, noting that it is frequently confused with tendinitis or disruption of the posterior tibial tendon. A symptomatic accessory navicular bone is often seen in adults following mild trauma, which induces shear forces that disrupt the synchondrosis, leading to a painful non-union or micro-instability.
Anatomical Classification
The accessory navicular bone is broadly classified into three primary types based on its morphology and relationship to the primary navicular:
- Type I: Occurs primarily as a small, round sesamoid bone (2–3 mm) embedded within the distal substance of the posterior tibial tendon. It is completely separate from the navicular and is rarely associated with clinical symptoms.
- Type II: A larger, triangular or heart-shaped ossicle (up to 12 mm) connected to the medial aspect of the primary navicular via a 1- to 2-mm layer of fibrocartilage or hyaline cartilage (synchondrosis). This type is highly at risk for disruption from traction injuries or shear forces, making it the most frequently symptomatic variant.
- Type III: Also known as a navicular beak or a cornuate navicular. This occurs when the accessory navicular bone fuses completely to the body of the primary navicular, creating a prominent medial bony excrescence.

Fig. 79-8 Elongated cornuate navicular (Type III).
Clinical and Radiographic Evaluation
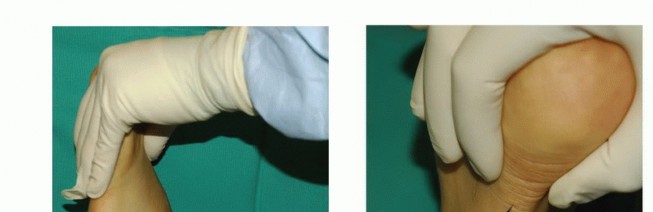
Patients typically present with a prominent bony medial eminence, localized tenderness, and pain exacerbated by weight-bearing activities, tight-fitting footwear, or sports.

Fig. 79-7 Accessory navicular. A, Teenage girl with prominent symptomatic accessory navicular. B, Large accessory navicular.
If a patient presents with a bilateral accessory navicular but only one foot becomes symptomatic following a traumatic event (often minor trauma or a twisting injury), the foot must be carefully evaluated both clinically and radiographically for asymmetrical pes planus.

Radiographic Assessment
Standard weight-bearing radiographs of the foot (anteroposterior, lateral, and oblique) are mandatory.
On the lateral weight-bearing film, the talonavicular, cuneiform–first metatarsal, and dorsal alignments must be closely examined. A "sag" at any of these joints indicates a critical loss of structural integrity in the medial column.
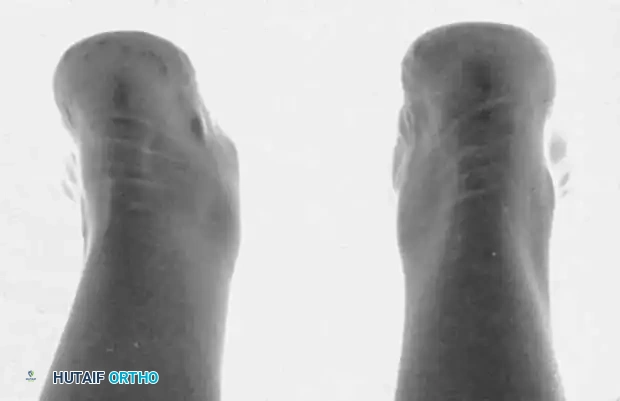
Fig. 79-9 C, Note “sag” at talonavicular joint (arrow) in the symptomatic left foot.
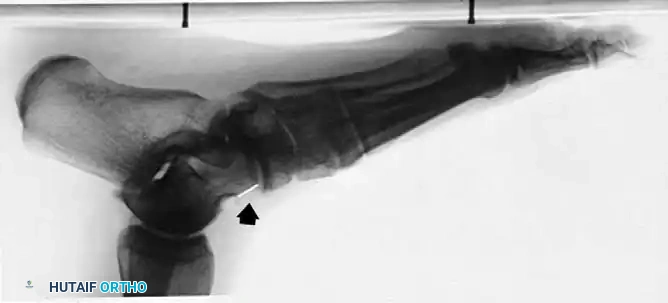
Fig. 79-9 D, There is no sag in the asymptomatic right foot.
Furthermore, the anteroposterior view may reveal an "opening up" of the metatarsal-cuboid-cuneiform articulations, suggesting a flattening of the longitudinal arch.

Fig. 79-9 B, Arrows point to “opening up” of metatarsal cuboid–cuneiform articulation, suggesting flattening of the longitudinal arch.
Also of significant clinical interest is the pronation of the entire forefoot upon weight-bearing, which is best visualized in the weight-bearing sesamoid view. Subsequent development of hallux valgus is common in these structurally compromised feet.

Fig. 79-9 E, On the symptomatic left foot, the entire forefoot is pronated in the weight-bearing sesamoid view.
Surgical Warning: Recognition of the loss of structural integrity of the longitudinal arch is paramount. This structural component of the deformity will not be corrected simply by excising the accessory navicular and reinserting or advancing the posterior tibial tendon. Severe, rigid pes planus requires concomitant structural realignment (e.g., calcaneal lengthening osteotomy).
Indications for Surgery
The primary indication for the Kidner procedure is a symptomatic accessory navicular bone with localized point tenderness over the medial eminence that has failed conservative management.
In most patients presenting with an acute injury to the synchondrosis, a strict trial of 6 to 8 weeks of cast or controlled ankle motion (CAM) boot immobilization is highly recommended before considering surgical intervention. If pain and dysfunction persist despite adequate immobilization and subsequent orthotic management, surgical excision is warranted.
Surgical Techniques
The Kidner Procedure
The classic Kidner procedure consists of excising the accessory navicular and rerouting the posterior tibial tendon into a more plantar position to theoretically restore its suspensory function.
Preoperative Counseling: Parents and patients must be explicitly informed before surgery that permanent correction of the arch sag cannot be guaranteed. However, relief of symptoms around the prominent tuberosity and the reduction or elimination of fatigue from arch strain are highly predictable.
Step-by-Step Surgical Approach:
1. Positioning and Anesthesia: The patient is placed supine on the operating table. A bump may be placed under the contralateral hip to externally rotate the operative leg, providing optimal access to the medial foot. A thigh or calf tourniquet is applied.
2. Incision: A longitudinal or slightly curved incision is made over the medial aspect of the midfoot, centered directly over the prominent accessory navicular, extending from the tip of the medial malleolus to the medial cuneiform.
3. Dissection: Subcutaneous tissues are carefully dissected. The saphenous vein and nerve branches must be identified and protected dorsally.
4. Tendon Exposure: The sheath of the posterior tibial tendon is incised longitudinally. The tendon is traced distally to its insertion on the accessory navicular.
5. Excision of the Ossicle: A longitudinal incision is made directly through the substance of the posterior tibial tendon overlying the accessory navicular. The tendon is sharply peeled back via sharp subperiosteal dissection to expose the ossicle. The accessory navicular is then shelled out and excised.
* Note on Type III (Cornuate Navicular): Excising the beak of the navicular flush with the medial border of the first cuneiform may relieve symptoms. However, in the series by Ray and Goldberg, excising the navicular beak alone was not as helpful as complete excision of the accessory navicular.
6. Tendon Advancement and Repair: The medial surface of the primary navicular is decorticated to bleeding bone to promote tendon healing. The posterior tibial tendon is then advanced plantarly and laterally. It is secured to the primary navicular using robust non-absorbable sutures or commercially available suture anchors.
7. Closure: The tendon sheath is repaired if possible, followed by standard layered closure of the subcutaneous tissue and skin.
Adjunctive Procedures for Structural Pes Planus (Lateral Column Lengthening)
As previously noted, simple excision of the accessory navicular will not correct a severe, structural pes planus. In cases where the calcaneal pitch angle is significantly lowered (as studied by Prichasuk and Sinphurmsukskul) and there is profound midfoot sag, a lateral column lengthening (Evans-type calcaneal osteotomy) may be required concomitantly.
Step-by-Step Calcaneal Osteotomy:
1. Osteotomy: A lateral approach to the calcaneus is performed. An osteotomy is created approximately 1.5 cm proximal to the calcaneocuboid joint.
2. Distraction: A lamina spreader is inserted into the osteotomy site to distract the fragments and lengthen the lateral column, thereby correcting the forefoot abduction and restoring the medial longitudinal arch.
* Pitfall: Ensure the distal calcaneal fragment does not become prominent and tent the skin; subluxation of the calcaneocuboid joint can also occur and must be monitored radiographically. If subluxation occurs, remove the lamina spreader to allow the osteotomy to close slightly.
3. Fixation Preparation: Insert a large, smooth Steinmann pin longitudinally from the dorsal-distal aspect of the cuboid, through the center of the calcaneocuboid joint, and into the center of the osteotomy surface of the distal calcaneal fragment.
4. Graft Placement: Use a trapezoid-shaped, tricortical bone graft (allogenic or autogenous from the iliac crest). In children with open apophyses, bicortical grafts are adequate. Align the cortical edges of the graft axially on the dorsal, lateral, and plantar surfaces for immediate structural stability.
5. Impaction: Impact the graft from lateral to medial in the most plantar portion of the osteotomy. The talonavicular joint should now be well aligned and stable.
6. Mosca's Modifications: Mosca recommended plantar medial plication of the talonavicular joint capsule and advancement of the posterior tibial tendon if mobility remains at the talonavicular joint. He also recommended Z-lengthening of the peroneal tendons in patients with cerebral palsy or severe rigid deformities.
7. Achilles Assessment: The Achilles tendon is lengthened (percutaneous or open Z-lengthening) if the ankle lacks at least 10 degrees of dorsiflexion with the knee extended after graft placement.
8. Final Fixation: Advance the Steinmann pin(s) through the graft and into the proximal calcaneal fragment. Bend them at the skin surface and leave them long for easy retrieval in the clinic after bony union.
9. Addressing Forefoot Supination: Adjacent deformities become more apparent after hindfoot correction. Most long-standing flatfeet have rigid supination of the forefoot. A plantar medial, closing wedge osteotomy of the medial cuneiform gives a satisfactory result in these specific cases.
Alternative Procedures (Not Recommended)
Alternative treatments to the traditional Kidner procedure exist but lack significant long-term follow-up or complementary studies to support their widespread use:
* Percutaneous Drilling: Nakayama et al. described percutaneously drilling the symptomatic accessory navicular to stimulate fusion between the primary and accessory bones, claiming efficacy in younger patients with open physes.
* Osteotomy and Screw Fixation: Malicky et al. described a modification involving an osteotomy on the medial side of the navicular body and lateral aspect of the accessory navicular, followed by lag screw fixation to achieve bony union.
* Author's Stance: We have no experience with these specific modifications and, given the high success rate of the standard Kidner procedure, cannot recommend either of these alternative procedures at this time.
Postoperative Protocol
Meticulous postoperative care is critical for ensuring tendon incorporation and preventing recurrence of symptoms.
- Immediate Post-Op: Drains (if used in older adolescents or adults for complex reconstructions) are removed the following day. A bulky soft dressing is placed around the foot and lower leg, and a sterile cast is applied in the operating suite.
- 0 to 4 Weeks: The initial cast is left in place for 4 weeks, strictly non-weight-bearing, unless neurovascular signs or evidence of infection demand early removal.
- 4 to 8 Weeks: At 4 weeks, the initial cast is removed. A short leg cast, well-molded into the arch with the foot in a plantigrade position, is applied. Partial weight-bearing is initiated.
- 8 to 10 Weeks: At 8 weeks, the cast is removed, and full weight-bearing is allowed, often transitioning into a CAM boot or supportive athletic shoe.
- 10+ Weeks: At 10 weeks, a firm, custom-molded arch support is fitted in a supportive leather oxford or athletic shoe.
Clinical Pearl: It has been our experience that many patients require a full 6 to 12 months to become completely asymptomatic at the site of the tendon repair and advancement. Patient expectations must be managed accordingly.
Clinical Outcomes and Evidence
The efficacy of simple excision of the accessory navicular in a symptomatic foot, with or without pes planus, has been affirmed by numerous independent reports, including landmark studies by MacNicol, Voutsinas, and Miller.
Prichasuk and Sinphurmsukskul reported good results in 27 of 28 patients after the Kidner procedure, noting profound improvements in pain and fatigue. However, they observed that only three patients demonstrated any clinical improvement in the medial longitudinal arch, reinforcing the concept that the Kidner procedure is a pain-relieving operation, not a structural arch-restoring one.
In 2004, Kopp and Marcus reported retrospective clinical outcomes of surgical management in 14 feet with an average follow-up of 103 months. Surgery consisted of simple excision and anatomical repair of the posterior tibial tendon. They reported excellent results: 13 of 14 feet were completely pain-free, no patients had activity limitations, and only two required shoe insert modifications. Crucially, these authors also confirmed that patients did not experience any change in their arch alignment postoperatively.
📚 Medical References
You Might Also Like