Operative Management of Quadriceps Tendon Ruptures
Key Takeaway
Quadriceps tendon rupture is a debilitating injury requiring prompt surgical intervention to restore the extensor mechanism. Operative management involves meticulous debridement, transosseous tunnel or suture anchor fixation for osteotendinous avulsions, and robust retinacular repair. Chronic ruptures with significant retraction may necessitate advanced reconstruction techniques, such as the Codivilla inverted-V lengthening. Strict adherence to biomechanical principles and phased postoperative rehabilitation is paramount for optimal functional recovery and minimizing complications like extensor lag or stiffness.
INTRODUCTION AND BIOMECHANICS
Rupture of the quadriceps femoris tendon is a profound disruption of the knee’s extensor mechanism, typically occurring in patients over the age of 40. The injury frequently manifests in the setting of eccentric loading—such as a rapid deceleration or a stumble on stairs—where the applied force exceeds the tensile strength of the degenerated tendon. Systemic risk factors, including chronic kidney disease, diabetes mellitus, hyperparathyroidism, and the use of fluoroquinolones or corticosteroids, significantly predispose the tendon to tendinosis and subsequent failure.
Anatomically, the quadriceps tendon is a trilaminar structure composed of the rectus femoris (superficial layer), the vastus medialis and lateralis (middle layer), and the vastus intermedius (deep layer). Ruptures most commonly occur 1 to 2 cm proximal to the superior pole of the patella, a region identified as a vascular watershed zone. Complete ruptures inevitably involve the medial and lateral retinacular expansions, resulting in a total loss of active knee extension.
Prompt surgical repair is the gold standard for complete ruptures. Delayed treatment (beyond 3 to 6 weeks) leads to proximal muscle retraction, severe adhesions, and intrinsic tendon shortening, transforming a straightforward primary repair into a complex reconstructive challenge requiring tissue advancement or augmentation.
💡 Clinical Pearl
Always evaluate the medial and lateral retinacular expansions during surgical exploration. The quadriceps tendon alone cannot restore full extensor power; failure to meticulously repair the retinaculum is a primary cause of postoperative extensor lag.
INDICATIONS AND PREOPERATIVE PLANNING
Indications for Surgery
- Complete Rupture: Evidenced by a palpable suprapatellar gap and an inability to perform a straight leg raise or maintain active knee extension against gravity.
- Partial Rupture with Extensor Lag: Cases where conservative management has failed or where the remaining intact fibers are insufficient to provide functional knee extension.
- Chronic Rupture: Delayed presentations requiring specialized lengthening procedures (e.g., Codivilla technique) or allograft reconstruction.
Preoperative Imaging
While the diagnosis is primarily clinical, imaging is critical for surgical planning:
* Radiographs: Lateral views may reveal patella baja (due to unopposed patellar tendon pull), soft tissue swelling, obliteration of the quadriceps fat pad, or avulsion fragments from the superior pole.
* Magnetic Resonance Imaging (MRI): The modality of choice to differentiate partial from complete tears, assess the degree of tendon retraction, and evaluate the quality of the remaining tissue.
* Ultrasound: A dynamic, cost-effective alternative to MRI for confirming the diagnosis and measuring the gap size.
PATIENT POSITIONING AND ANESTHESIA
- Anesthesia: General anesthesia or regional neuraxial anesthesia (spinal/epidural) is utilized. A femoral nerve block or adductor canal block may be administered for postoperative analgesia, though care must be taken to avoid masking postoperative neurologic assessments.
- Positioning: The patient is placed in the supine position on a standard radiolucent operating table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal thigh to ensure a bloodless surgical field.
- Preparation: The operative extremity is prepped and draped in a standard sterile fashion, allowing for full, unrestricted range of motion of the knee during the procedure.
SURGICAL TECHNIQUE: ACUTE QUADRICEPS TENDON RUPTURE
The surgical approach for an acute rupture focuses on anatomic restoration of the tendon footprint and robust mechanical fixation to withstand the immense forces of early rehabilitation.
Approach and Debridement
- Incision: Make a midline longitudinal incision measuring 15 to 20 cm, centered over the palpable defect and extending distally to the superior third of the patella.
- Dissection: Elevate full-thickness fasciocutaneous flaps medially and laterally to expose the ruptured tendon and the torn retinacular expansions. Avoid undermining the subcutaneous tissues to preserve the delicate vascular supply to the skin.
- Hematoma Evacuation: Thoroughly irrigate the fracture hematoma.
- Tissue Preparation: Freshen the frayed, degenerative tendon ends using a scalpel or rongeur until healthy, organized collagen bundles are encountered.
⚠️ Surgical Warning
Do not over-resect the tendon ends. While debridement of necrotic tissue is necessary, excessive shortening will significantly increase tension on the repair, predisposing the patient to postoperative stiffness or rerupture.
Mid-Substance Tendon Repair
If the rupture occurs entirely within the mid-substance of the tendon and sufficient tissue remains attached to the superior pole of the patella:
1. Primary Apposition: Perform a direct end-to-end repair.
2. Suturing: Utilize multiple No. 2 or No. 5 nonabsorbable mattress sutures (e.g., Ethibond or FiberWire) placed through the robust portions of the tendon.
3. Retinacular Repair: Use No. 0 absorbable sutures (e.g., Vicryl) to meticulously repair the medial and lateral retinaculum.
4. Tracking Assessment: Carefully align the tendon and move the knee through a gentle range of motion to evaluate patellar tracking and the tension of the repair.
5. Augmentation: In cases of tenuous tissue quality, a circumferential cerclage wire or heavy nonabsorbable suture may be routed around the superior pole of the patella and through the proximal tendon to protect the primary repair.
Osteotendinous Junction Avulsion (Transosseous Technique)
The most common pattern is an avulsion directly from the superior pole of the patella.
- Vastus Intermedius Stump: Frequently, an 8 to 10-mm stump of the vastus intermedius remains attached to the patella. Place No. 0 nonabsorbable sutures through this stump and lay them aside; these will be used later to reinforce the repair.
- Trough Creation: Using a rongeur or a high-speed burr, decorticate the superior pole of the patella to create a bleeding, 5 to 10-mm deep bony trough. This promotes a robust healing response at the tendon-bone interface.
- Transosseous Tunnels: Drill three parallel, longitudinal holes (typically using a 2.0 mm or 2.5 mm drill bit) approximately 1 cm apart. These tunnels should be centered over the anticipated anatomical footprint of the quadriceps tendon, starting in the trough and exiting at the anterior-inferior aspect of the patella.
- Tendon Suture Passage:
- Utilize a No. 5 nonabsorbable suture (or high-tensile strength tape).
- Begin proximally and weave the suture down the lateral third of the quadriceps tendon using a running interlocking (Krackow) technique for a distance of about 2.5 cm, ensuring purchase in normal-appearing tendon.
- Pass the suture distally in a similar manner, ending just lateral to the midline of the ruptured tendon.
- Repeat this process with a second No. 5 nonabsorbable suture along the medial side of the tendon.
- Suture Retrieval: Pass the free ends of the sutures distally through the pre-drilled transosseous tunnels using a suture retriever or a Beath pin. Place a single throw in the sutures and temporarily secure them with a hemostat.
- Biomechanical Check: Move the knee through a range of motion to verify patellar tracking, isometry, and the absence of gap formation at the repair site.
- Final Fixation:
- If placement is satisfactory, bring the previously placed sutures in the vastus intermedius stump anteriorly and secure them through the quadriceps tendon while maintaining anatomical position.
- Tie the heavy transosseous sutures distally over the bony bridge at the inferior pole of the patella, firmly drawing the proximal tendon stump into the bleeding bony trough.
- Closure: Repair the medial and lateral retinaculum with interrupted absorbable sutures. Close the subcutaneous tissue and skin in a routine, layered manner.
SURGICAL TECHNIQUE: CHRONIC QUADRICEPS TENDON RUPTURE
When a rupture of the quadriceps tendon is neglected or misdiagnosed for months or years, primary end-to-end repair becomes impossible due to severe proximal muscle retraction, fibrosis, and tendon atrophy. A defect of 2.5 to 5.0 cm or more is typically present between the tendon ends.
If the ends can be apposed with maximal distal traction, the repair is performed as described for an acute rupture. However, if shortening makes apposition impossible, advanced reconstructive techniques are required. Fascia lata autograft or allograft augmentation can be utilized, but the Codivilla Tendon Lengthening technique remains a highly effective, autologous solution.
The Codivilla Tendon Lengthening Technique
The Codivilla technique utilizes a V-Y advancement flap from the proximal quadriceps tendon to bridge the defect without sacrificing the continuity of the extensor mechanism.
- Incision and Exposure: A standard midline approach is utilized, extending further proximally to expose the healthy proximal quadriceps tendon and muscle belly.
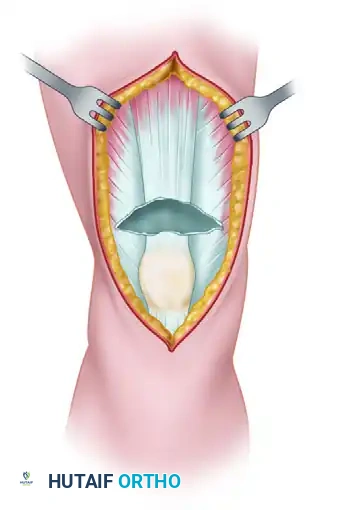
- The Inverted-V Cut: An inverted V is cut through the full thickness of the proximal segment of the quadriceps tendon. The apex of the V is directed proximally. The inferior ends (base) of the V must end 1.5 to 2.0 cm proximal to the rupture edge to maintain a bridge of intact tissue.
Figure A: Creation of the full-thickness inverted-V incision in the proximal quadriceps tendon.
- Flap Splitting: The triangular flap fashioned by the V-cut is meticulously split in the coronal plane. It is divided into an anterior part comprising one-third of its thickness, and a posterior part comprising two-thirds of its thickness.
- Tendon Apposition: The main tendon ends are drawn together as closely as possible and apposed with interrupted sutures.
- Flap Turn-Down: The anterior one-third of the split triangular flap is turned distally (flipped 180 degrees) to bridge the remaining gap and reinforce the repair site. It is sutured securely to the distal tendon stump or the patella.
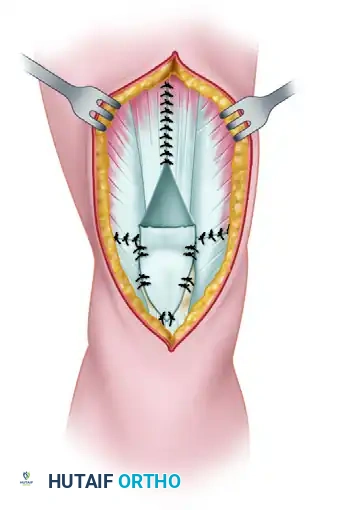
Figure B: The anterior one-third of the flap is turned distally to bridge the defect.
- Closure of the V: The open upper part of the V (the donor site) is closed side-to-side with interrupted sutures, effectively converting the V into a Y and lengthening the extensor mechanism.
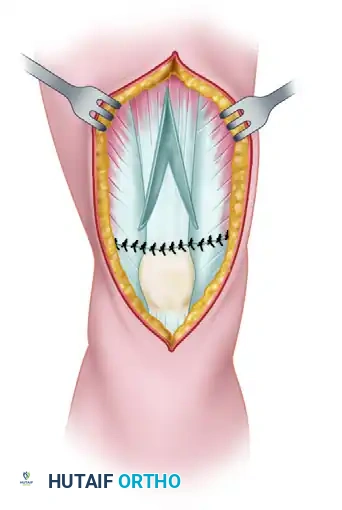
Figure C: Final repair showing the turned-down flap sutured in place and the proximal V-defect closed.
- Protection: Pull-out wire sutures or heavy cerclage cables can be used to protect the repair from early catastrophic failure, though with modern heavy suture materials and strict bracing, these are typically not necessary and avoid the complication of hardware prominence.
POSTOPERATIVE REHABILITATION PROTOCOL
Successful outcomes depend equally on meticulous surgical technique and strict adherence to a phased rehabilitation protocol. The goal is to protect the healing tendon while preventing arthrofibrosis.
- Phase I (Weeks 0 to 3):
- The knee is immobilized in a cylinder cast or a locked hinged knee brace in full extension.
- Weight-bearing is restricted. The patient is strictly non-weight-bearing or touch-down weight-bearing with crutches.
- Isometric quadriceps sets and straight leg raises (in the brace) are initiated immediately to prevent profound muscle atrophy.
- Phase II (Weeks 3 to 6):
- Weight-bearing with crutches is officially allowed and advanced as tolerated at the 3-week mark.
- The cast is removed (if used), and a dial-locked hinged knee brace is fitted.
- Range of motion (ROM) is initiated from 0 to 60 degrees of flexion.
- The allowed flexion range is increased by 10 to 15 degrees each subsequent week.
- Phase III (Weeks 6 to 12):
- The brace is unlocked for ambulation once the patient demonstrates good quadriceps control without an extensor lag.
- ROM is progressed to full flexion.
- An aggressive strengthening program is essential for good functional recovery, focusing on closed-kinetic-chain exercises (e.g., mini-squats, leg presses).
- Phase IV (Months 3 to 6+):
- Return to light jogging and sport-specific activities is permitted once quadriceps strength reaches 85-90% of the contralateral limb.
- Full recovery and maximal medical improvement may take up to 12 months.
COMPLICATIONS AND AVOIDANCE
Despite optimal surgical management, complications can arise. Anticipation and early intervention are key to mitigating long-term morbidity.
- Loss of Motion (Stiffness): Loss of terminal flexion is the most common complication following quadriceps tendon repair. It is directly correlated with prolonged immobilization. Strict adherence to the initiation of ROM at 3 weeks is critical. If severe arthrofibrosis develops, manipulation under anesthesia (MUA) or arthroscopic lysis of adhesions may be required after the tendon has fully healed (typically >12 weeks).
- Extensor Mechanism Weakness: Manifested by persistent quadriceps atrophy and an extensor lag. This is often due to inadequate repair of the retinaculum or failure to tension the tendon anatomically. While mild lags often correct with time and proper rehabilitation, severe lags may require surgical revision.
- Infection and Wound Healing: The anterior knee has a tenuous blood supply. Subcutaneous placement of bulky nonabsorbable sutures, wires, or an incision placed directly over the tibial tubercle can lead to wound breakdown and deep infection. Meticulous soft tissue handling and layered closure are mandatory.
- Hardware Complications: If circumferential wires are used for augmentation, they frequently become prominent, cause bursa formation, or undergo fatigue breakage. These sutures or wires occasionally require secondary surgical removal.
- Patella Alta or Baja: Non-anatomic tensioning of the repair alters the patellofemoral mechanics. Over-tensioning leads to patella alta, while under-tensioning or prolonged immobilization leads to patella baja. Malalignment can lead to accelerated degenerative changes at the patellofemoral joint by exponentially increasing joint reactive forces. Surgeons must pay close attention to the position of the patella within the sagittal plane during surgery, comparing it to preoperative radiographs of the contralateral knee.
- Rerupture: A devastating complication that requires repeat, often complex reconstructive repair. It is usually the result of patient non-compliance with the postoperative bracing protocol, a premature return to high-impact activities, or technical failure of the suture-tendon interface. Utilizing locked Krackow stitches and robust transosseous fixation minimizes this risk.
You Might Also Like