Hamstring Autograft Augmentation for Patellar Tendon Reconstruction
Key Takeaway
Hamstring autograft augmentation utilizing the semitendinosus and gracilis tendons is the gold standard for reconstructing chronic or neglected patellar tendon ruptures. This one-stage procedure provides robust biomechanical stability, minimizing gap formation under cyclic loading. By routing the autografts through osseous tunnels in the patella and tibial tubercle, surgeons can restore the extensor mechanism's integrity, correct patella alta, and permit early postoperative mobilization without the morbidity of allograft rejection.
Introduction and Historical Context
The reconstruction of neglected or chronic patellar tendon ruptures presents a formidable challenge to the orthopedic surgeon. Unlike acute ruptures, which can often be managed with primary end-to-end repair and cerclage wire augmentation, chronic ruptures are characterized by proximal patellar migration (patella alta), severe quadriceps contracture, and profound attenuation or complete absence of viable patellar tendon tissue.
Historically, authors such as Ecker, Lotke, and Glazer advocated for a two-stage procedure. The first stage involved freeing the quadriceps mechanism and applying skeletal traction through the patella via a Kirschner wire to gradually overcome the soft tissue contracture. The second stage consisted of reconstructing the patellar tendon using the semitendinosus tendon.
Modern orthopedic consensus has shifted decisively toward a one-stage procedure. Advances in soft tissue mobilization, specifically Z-lengthening of the quadriceps tendon, combined with the simultaneous harvest of both the semitendinosus and gracilis tendons, have rendered the two-stage approach largely obsolete. Utilizing both hamstring tendons is now considered necessary to provide adequate biomechanical augmentation. The hamstring autograft is highly suitable because it utilizes strong, native autogenous tissue, eliminates the risk of allograft rejection or disease transmission, avoids the need for a secondary surgery for hardware removal, and possesses sufficient tensile strength to allow for early, safe postoperative mobilization. Furthermore, extensive literature demonstrates that harvesting the ipsilateral hamstrings causes negligible long-term functional deficit to knee flexion or internal rotation strength.
Biomechanical Rationale
The primary goal of augmenting a patellar tendon repair is to protect the healing native tissue (or the primary repair site) from the immense tensile forces generated by the quadriceps mechanism.
Biomechanical studies evaluating cyclic loading of the extensor mechanism have consistently demonstrated that primary end-to-end repairs are highly susceptible to gap formation and catastrophic failure. Augmentation with the semitendinosus and gracilis tendons acts as an internal load-sharing device. By routing these robust autografts through osseous tunnels in the patella and the tibial tuberosity, the construct effectively bypasses the fragile repair site. This significantly decreases gap formation at the repair site during cyclic loading, ensuring that the restored patellar height is maintained throughout the critical early phases of biological healing.
Clinical Pearl: The ultimate tensile strength of a doubled semitendinosus and gracilis graft exceeds 4,000 Newtons, which is more than sufficient to withstand the forces of early postoperative passive range of motion and protected weight-bearing, provided the osseous fixation points are secure.
Indications and Preoperative Planning
Indications
- Neglected/Chronic Ruptures: Ruptures presenting more than 6 weeks post-injury where primary repair is impossible due to tissue retraction and degeneration.
- Failed Primary Repairs: Revision scenarios where the native tissue has stretched out or ruptured secondary to non-compliance or biological failure.
- Poor Tissue Quality: Acute ruptures in patients with systemic conditions (e.g., systemic lupus erythematosus, rheumatoid arthritis, chronic corticosteroid use) where the native tendon is highly attenuated and cannot hold suture tension.
Preoperative Evaluation
A meticulous clinical examination must assess the degree of quadriceps atrophy and the mobility of the patella. Standard weight-bearing anteroposterior (AP) and lateral radiographs of both knees are mandatory. The contralateral uninjured knee serves as the template for determining the patient's native Insall-Salvati ratio, which is critical for restoring the correct patellar height intraoperatively. Magnetic Resonance Imaging (MRI) is highly recommended to evaluate the quality of the remaining extensor mechanism, the degree of quadriceps fatty infiltration, and the status of the intra-articular structures.
Surgical Technique: Step-by-Step Masterclass
1. Patient Positioning and Incision
The patient is placed supine on the operating table. A well-padded high thigh tourniquet is applied. The operative limb is prepped and draped free to allow full, unrestricted range of motion during the procedure.
Make a generous anterior longitudinal incision beginning just proximal and lateral to the superior pole of the patella. Extend the incision distally, crossing the midline of the limb inferior to the patella, and ending along the medial flare of the proximal tibia (approximately 4 to 5 cm distal to the tibial tuberosity). Elevate full-thickness fasciocutaneous flaps to preserve the vascular supply to the anterior skin.
2. Extensor Mechanism Mobilization and Z-Lengthening
Expose the patella, the quadriceps tendon, the remnants of the patellar tendon, and the tibial tuberosity. In chronic cases, the patella will be significantly retracted proximally, encased in dense scar tissue.
Aggressively remove all scar tissue from the remnants of the patellar tendon and the infrapatellar fat pad to mobilize the patella. Release the medial and lateral gutters. If the patella cannot be brought down to its anatomic position (matching the contralateral Insall-Salvati ratio) despite extensive soft tissue releases, a Z-lengthening of the quadriceps tendon is required. Conversely, the attenuated, scarred patellar tendon remnants may require Z-shortening to restore tension.
Figure A: Z-shortening of the attenuated patellar tendon and Z-lengthening of the contracted quadriceps tendon to restore anatomic patellar height.
3. Patellar Traction and Provisional Fixation
To maintain the patella at the correct distal position during the reconstruction, place a heavy Steinmann pin transversely through the mid-portion of the patella. Apply distal traction to the pin.
Once the patella is reduced to its anatomic position, place provisional tack sutures in the native tendon remnants to hold the alignment.
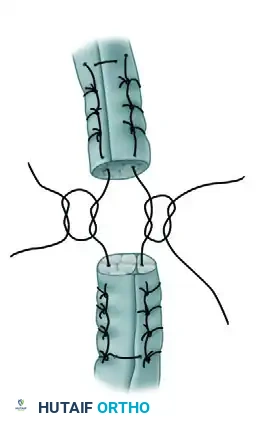
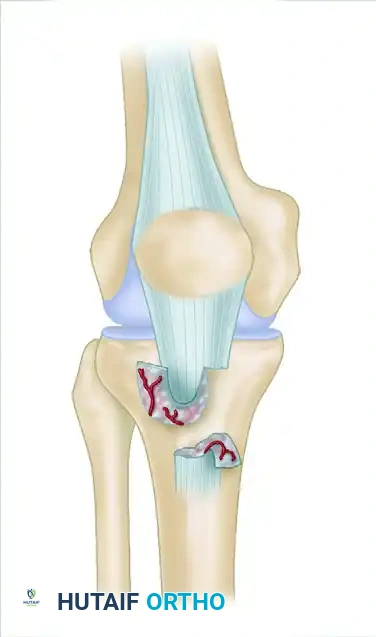
Figure B: Tack sutures are placed in the tendons to provisionally hold the Z-lengthened quadriceps and Z-shortened patellar tendon.
4. Hamstring Tendon Harvest
Flex the knee to 90 degrees and externally rotate the hip to expose the medial aspect of the proximal tibia. Identify the insertions of the gracilis and semitendinosus tendons at the pes anserinus.
Make a small incision over the pes anserinus if it is not adequately exposed by the primary incision. Carefully incise the sartorial fascia. Isolate the gracilis (superior) and semitendinosus (inferior) tendons. Ensure all fascial bands (especially the accessory bands of the semitendinosus extending to the medial gastrocnemius) are sharply released to prevent premature amputation of the graft.
Use an open-ended tendon stripper to release the tendons from their proximal musculotendinous junctions. Deliver the harvested tendons into the primary surgical field. Whipstitch the free ends of both tendons using a heavy, non-absorbable suture (e.g., #2 FiberWire) utilizing the Krackow technique. Suture the two tendons together to create a unified, robust graft complex.
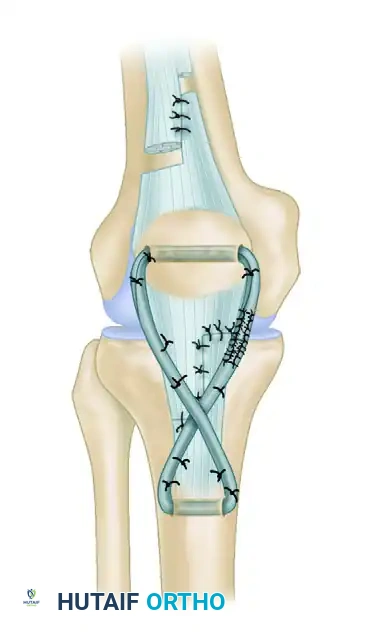
Figure C: The semitendinosus and gracilis tendons are harvested with a tendon stripper, prepared, and sutured together.
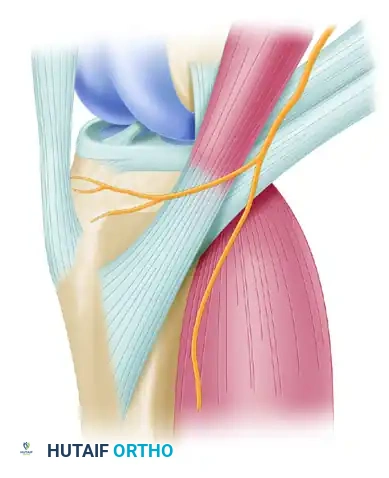
Surgical Warning: Meticulous care must be taken during the dissection of the pes anserinus to identify and protect the infrapatellar branch of the saphenous nerve, which frequently crosses the operative field. Iatrogenic injury can lead to painful neuromas and anterior knee numbness.
5. Osseous Tunnel Preparation
Attention is now turned to creating the osseous pathways for the autograft.
* Tibial Tunnel: Drill an oblique or transverse hole through the tibial tuberosity, posterior to the native tendon insertion. Ensure the bone bridge is at least 1.5 to 2.0 cm thick to prevent iatrogenic fracture of the tuberosity.
* Patellar Tunnels: Drill one or two transverse holes through the distal third of the patella.
Pitfall: Drilling the patellar tunnels too proximally or too anteriorly can alter the patellofemoral contact mechanics and significantly increase the risk of a transverse patellar fracture under load. Keep the tunnels in the distal, central-to-posterior half of the patella.
6. Graft Passage and Tensioning
Pass the combined semitendinosus and gracilis graft through the transverse hole in the patella.
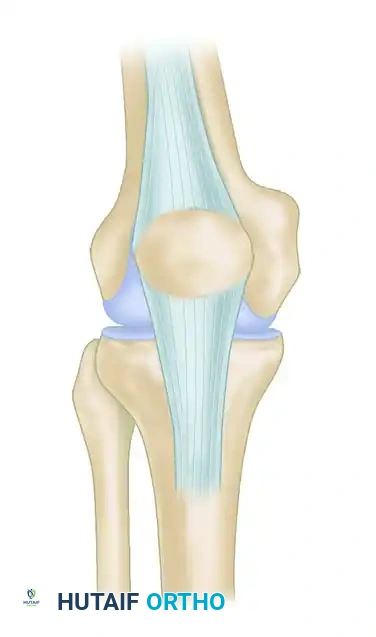
Figure D: The prepared hamstring tendons are passed through the transverse osseous hole in the distal patella and sutured together using the Krackow technique.
Next, route the free ends of the graft distally, crossing them in a figure-of-eight configuration (or keeping them parallel in a loop, depending on surgeon preference and graft length), and pass them through the osseous tunnel in the tibial tuberosity.
To ensure the patellar height is rigidly maintained during the suturing process, pass a heavy cerclage wire (or a heavy non-absorbable tape) through the patella and the tibial tuberosity. Tighten this wire to maintain a distance between the inferior pole of the patella and the tibial tuberosity that is exactly equal to the length of the patella (Insall-Salvati ratio of 1.0), or matched to the contralateral knee.
With the knee positioned in 30 degrees of flexion, tension the semitendinosus and gracilis tendons firmly. Suture the grafts to themselves, to each other, and tack them securely to the underlying native patellar tendon remnants using multiple interrupted non-absorbable sutures.
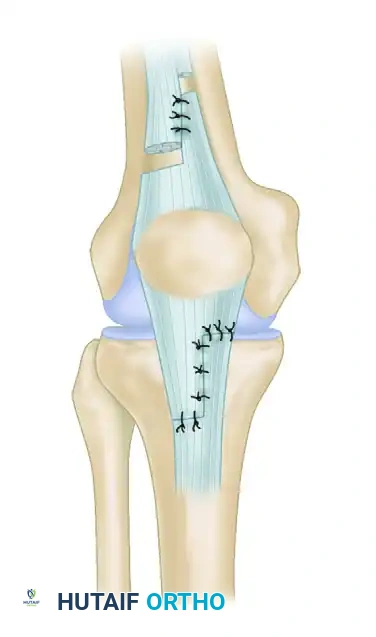
Figure E: The tendons are routed distally, passed through the tibial tuberosity, and tacked to the underlying vascularized, attenuated patellar tendon.
7. Final Construct Assembly and Closure
Verify the tension and tracking of the extensor mechanism by gently ranging the knee from 0 to 45 degrees. The construct should move synchronously without excessive tension or laxity.
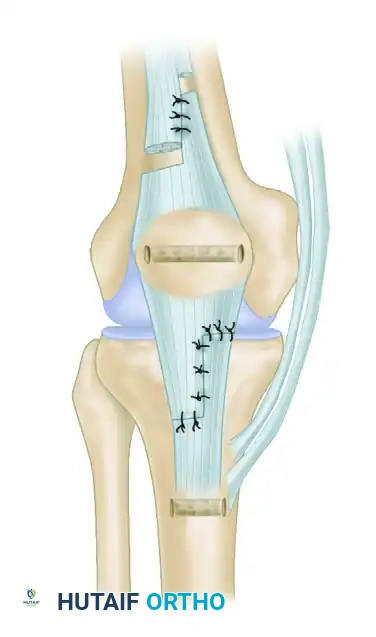
Figure F: Final overview of the reconstructed extensor mechanism. The semitendinosus and gracilis muscle tendons provide a robust, load-sharing augmentation over the scarred patellar tendon.
Once satisfied with the biomechanical integrity, remove the transverse Steinmann traction pin from the patella. Thoroughly irrigate the wound. Close the paratenon and subcutaneous tissues meticulously to ensure adequate soft tissue coverage over the grafts and hardware. Close the skin with staples or non-absorbable sutures. Apply a sterile dressing and immediately place the limb in a cylinder cast or a rigid locked hinged knee brace in full extension.
Postoperative Rehabilitation Protocol
The rehabilitation following a hamstring-augmented patellar tendon reconstruction must balance the need to protect the healing construct with the necessity of preventing profound arthrofibrosis, a common complication in chronic reconstructions. The timing of rehabilitation should be strictly adjusted based on the surgeon's intraoperative assessment of graft tension and tissue quality.
Phase I: Maximum Protection (Weeks 0 to 2)
- Immobilization: The knee is immobilized in full extension in a cylinder cast or a locked hinged knee brace.
- Weight-Bearing: Weight-bearing to tolerance with crutches is permitted, provided the knee is locked in absolute extension. The extensor mechanism must not be actively engaged.
- Clinical Review: At 10 to 14 days, the cast or brace is removed for comprehensive wound evaluation. Sutures or staples are removed if the incision is fully healed. A new cylinder cast or locked brace is applied.
Phase II: Controlled Mobilization (Weeks 2 to 6)
- Immobilization: A locked brace is worn continuously for ambulation.
- Range of Motion (ROM): Depending on intraoperative stability, active-assisted and passive range-of-motion exercises may be initiated at 4 to 6 weeks. Flexion is typically limited to 45 degrees initially, progressing slowly to 90 degrees by week 6.
- Muscle Activation: Isometric quadriceps sets and straight-leg raises (in the locked brace) are instituted to prevent profound quadriceps atrophy.
Phase III: Progressive Strengthening (Weeks 6 to 12)
- Immobilization: The brace is gradually unlocked for ambulation as quadriceps control improves. It may be discontinued once the patient can perform a straight-leg raise without an extensor lag.
- Range of Motion: Aggressive active and passive ROM exercises are advanced to achieve full flexion.
- Strengthening: Vigorous straight-leg raising with progressive weights is instituted. Closed kinetic chain exercises (e.g., mini-squats, leg presses) are introduced cautiously.
- Ambulation: Unassisted ambulation is allowed only when sufficient motion and quadriceps strength have been regained to stabilize the knee dynamically.
Phase IV: Return to Function (Months 3 to 6+)
A progressive strengthening, proprioception, and range-of-motion exercise program is essential to regain full functional capacity. Return to heavy manual labor or sports is generally delayed until 6 to 9 months postoperatively, contingent upon achieving at least 85% quadriceps strength compared to the contralateral limb and demonstrating no extensor lag.
Complications and Management
- Extensor Lag and Weakness: The most common complication. Often results from inadequate intraoperative tensioning or failure to aggressively rehabilitate the quadriceps. Managed with prolonged physical therapy.
- Arthrofibrosis: Due to the extensive surgical dissection and required immobilization, stiffness is frequent. If ROM plateaus at less than 90 degrees by 12 weeks, manipulation under anesthesia or arthroscopic lysis of adhesions may be indicated.
- Patella Fracture: Can occur through the transverse drill holes. Prevented by placing tunnels in the distal third of the patella and avoiding oversized drill bits.
- Infection and Wound Breakdown: The anterior knee has tenuous vascularity, especially after multiple incisions. Meticulous handling of full-thickness flaps is paramount.
- Hardware Irritation: The cerclage wire used to maintain patellar height may become symptomatic once the swelling subsides. It can be electively removed after 6 months once the tendon reconstruction has fully biologically integrated.
You Might Also Like