Acetabular and Pelvic Fractures: A Comprehensive Surgical Guide
Key Takeaway
Acetabular fractures represent one of the most formidable challenges in orthopaedic trauma. Successful management demands a profound understanding of pelvic osteology, precise radiographic interpretation, and mastery of complex surgical approaches. This guide details the evidence-based protocols for initial resuscitation, anatomical reduction, and rigid internal fixation. By adhering to the principles established by Letournel and Judet, surgeons can optimize articular congruity, minimize neurovascular complications, and significantly improve long-term patient outcomes in high-energy pelvic trauma.
Introduction to Acetabular Fractures
The operative treatment of acetabular fractures remains one of the most complex and demanding disciplines within orthopaedic trauma surgery. Historically managed nonoperatively with prolonged traction—often yielding poor functional outcomes and early post-traumatic arthrosis—the modern era of acetabular reconstruction was pioneered by Emile Letournel and Robert Judet. Their establishment of the two-column anatomical concept, standardized radiographic evaluation, and specific surgical approaches revolutionized patient care.
However, mastering these techniques involves a steep and well-documented learning curve. As demonstrated in landmark studies by Matta and Merritt, the chronological grouping of a surgeon’s first 100 operatively treated acetabular fractures reveals a direct correlation between surgical experience and the incidence of anatomical reductions.
Similarly, Kebaish, Roy, and Rennie highlighted that experienced pelvic trauma surgeons achieve significantly higher rates of anatomical reduction compared to their less experienced counterparts. Because the quality of articular reduction is the single most critical prognostic factor for long-term native hip survivorship, these procedures should ideally be performed in specialized trauma centers by surgeons with dedicated pelvic training.
Initial Trauma Management and Resuscitation
Advanced Trauma Life Support (ATLS) Protocol
Acetabular fractures are predominantly the result of high-energy blunt trauma, such as motor vehicle collisions or falls from significant heights. Consequently, patients frequently present with concomitant life-threatening injuries, including traumatic brain injury, thoracic trauma, and visceral abdominal injuries. The initial management must strictly adhere to Advanced Trauma Life Support (ATLS) protocols. Orthopaedic intervention is secondary to hemodynamic stabilization and the management of acute hemorrhage.
Skeletal Traction and Joint Distraction
Once the patient is hemodynamically stable, the injured hip must be evaluated. We advocate for the early application of skeletal traction (typically 20 to 35 pounds) via a distal femoral pin. Distal femoral traction is preferred over proximal tibial traction as it avoids tensioning the knee capsule and allows for knee flexion during subsequent surgical positioning.
Clinical Pearl: The primary goal of skeletal traction in the emergency setting is to distract the femoral head away from the sharp, abrasive edges of the fractured acetabular articular cartilage, thereby minimizing ongoing chondral damage and reducing the risk of osteonecrosis.
Management of Irreducible Dislocations
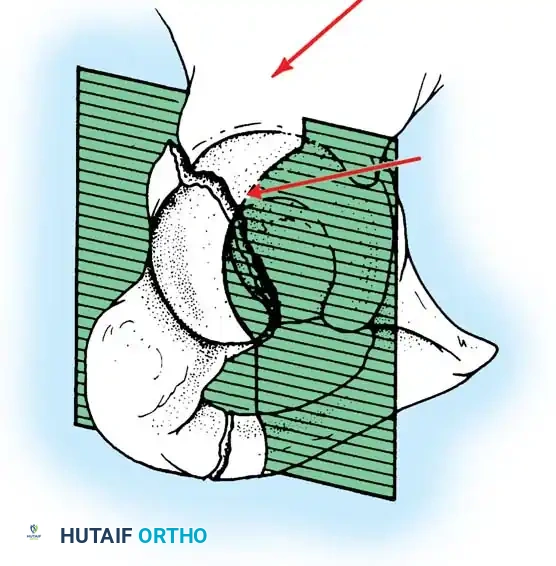
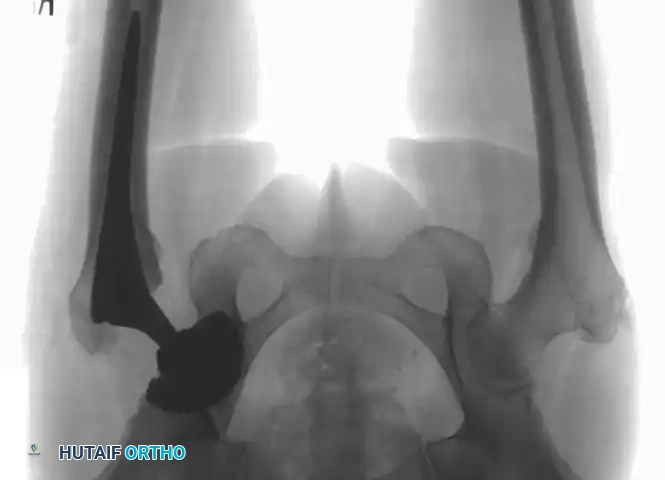
While most acetabular fractures are not surgical emergencies, an irreducible fracture-dislocation of the hip is a notable exception. The historical term "central fracture-dislocation" describes a severe medial subluxation of the femoral head into the true pelvis.

In these scenarios, the femoral head may become incarcerated between the superior and inferior fracture fragments, rendering closed reduction impossible.

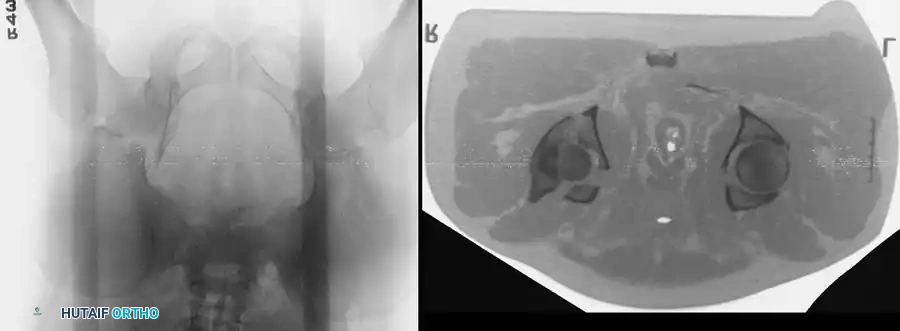
If closed reduction under conscious sedation or general anesthesia fails, urgent open reduction is mandated. A rapid, fine-cut (2-3 mm) Computed Tomography (CT) scan should be obtained to identify the incarcerating fragment—often a rotated posterior wall fragment or an intra-articular osteochondral loose body. Prolonged dislocation exponentially increases the risk of femoral head osteonecrosis and irreversible sciatic nerve ischemia.
Surgical Anatomy and Biomechanics
A profound three-dimensional understanding of pelvic osteology is non-negotiable for the acetabular surgeon.
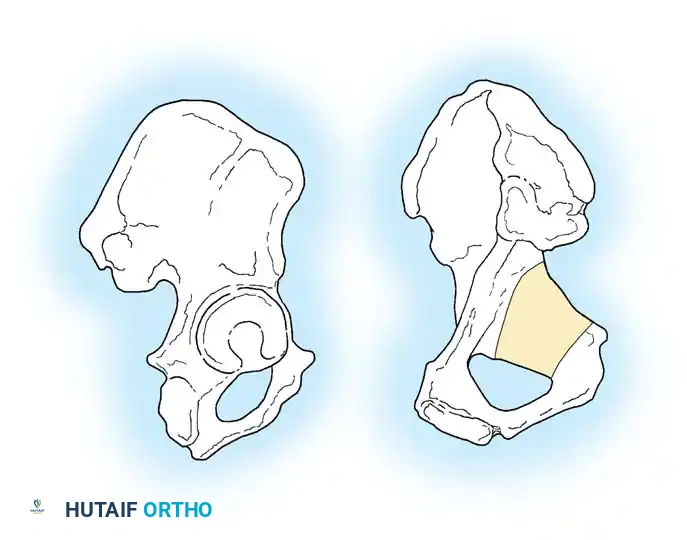
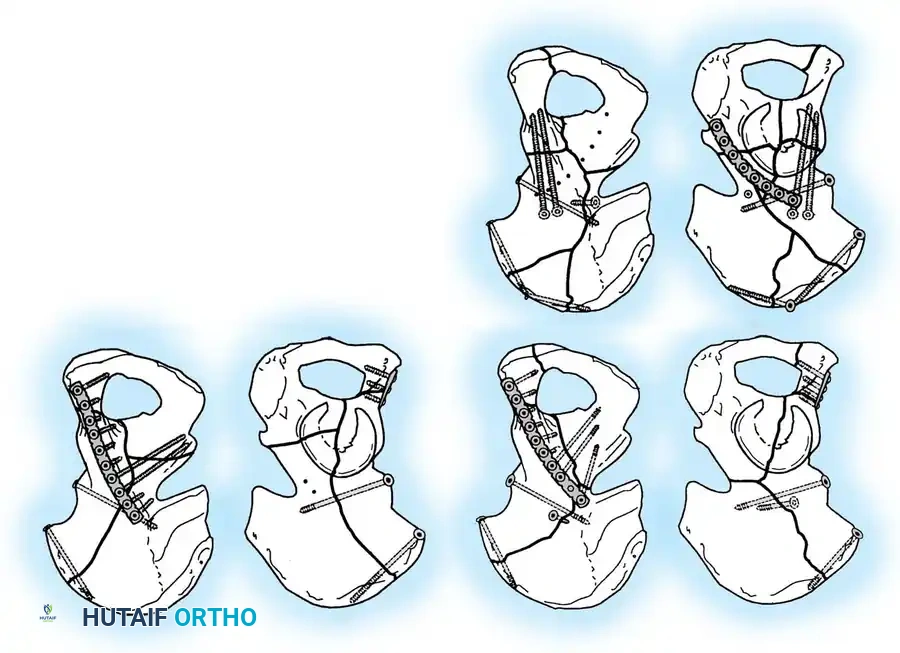
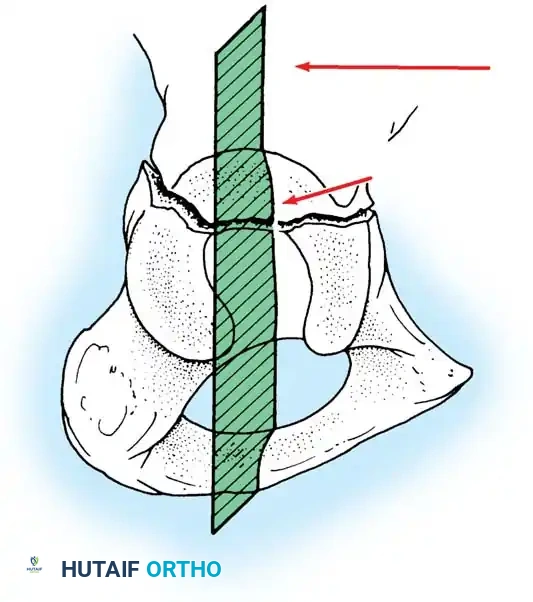
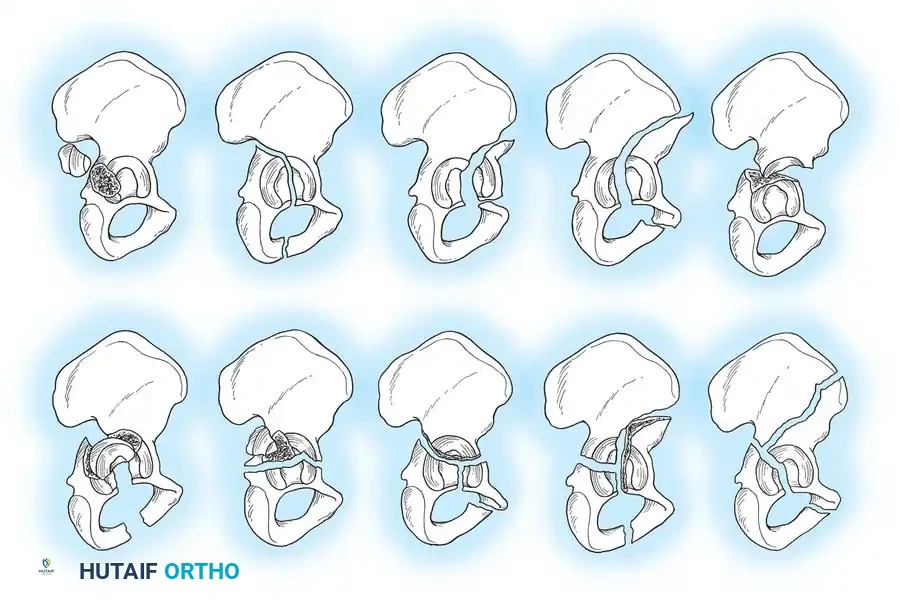
The Two-Column Concept of Letournel
Letournel described the acetabulum as an incomplete hemispherical socket supported by two distinct pillars of bone, resembling an inverted "Y".
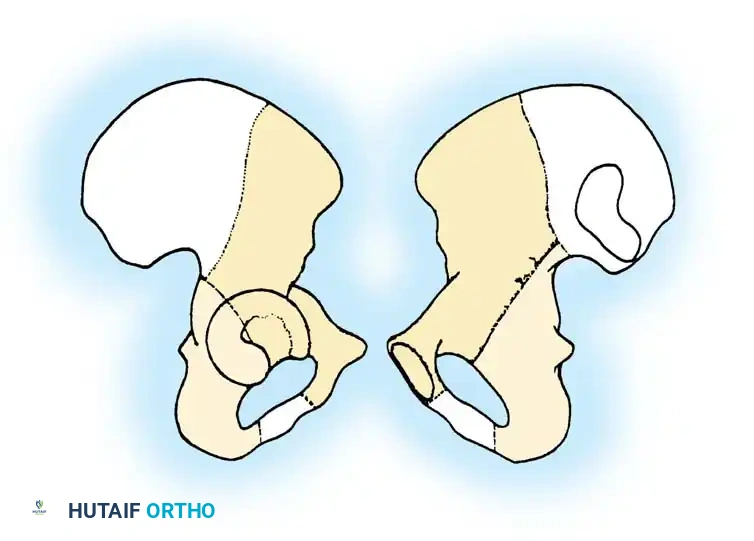
- The Anterior Column: Extends from the anterior iliac crest down to the pubic symphysis. It comprises the anterior iliac wing, the anterior superior and inferior iliac spines, the anterior half of the acetabular articular surface, and the superior and inferior pubic rami.
- The Posterior Column: A shorter, denser pillar of bone that begins at the dense bone of the greater sciatic notch and extends inferiorly to the ischial tuberosity. It includes the posterior half of the acetabulum, the ischial spine, and the ischium.
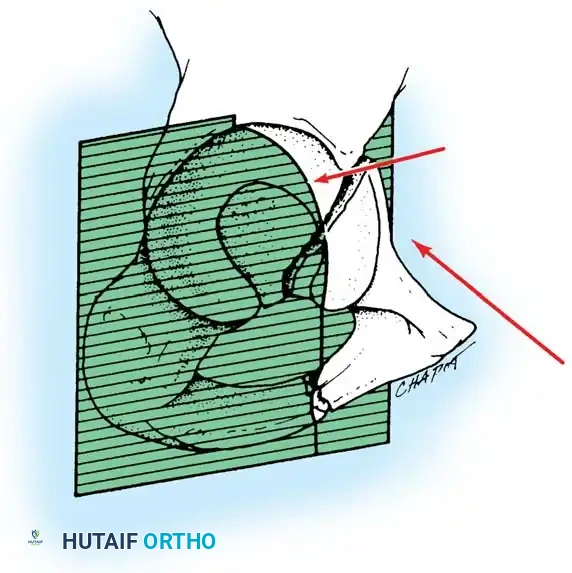
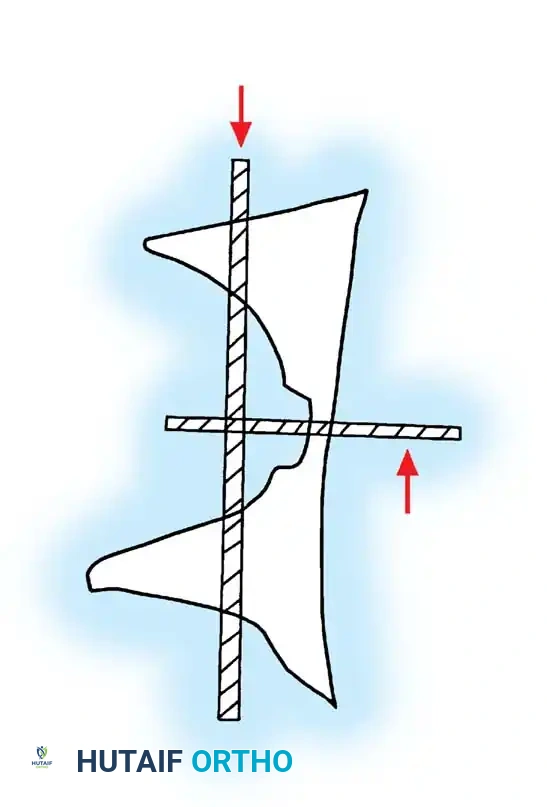
The Weight-Bearing Dome and Quadrilateral Surface
The superior aspect of the acetabulum, known as the "dome" or "roof," is the primary weight-bearing articular surface. Anatomical restoration of the dome is the ultimate goal of surgical intervention.
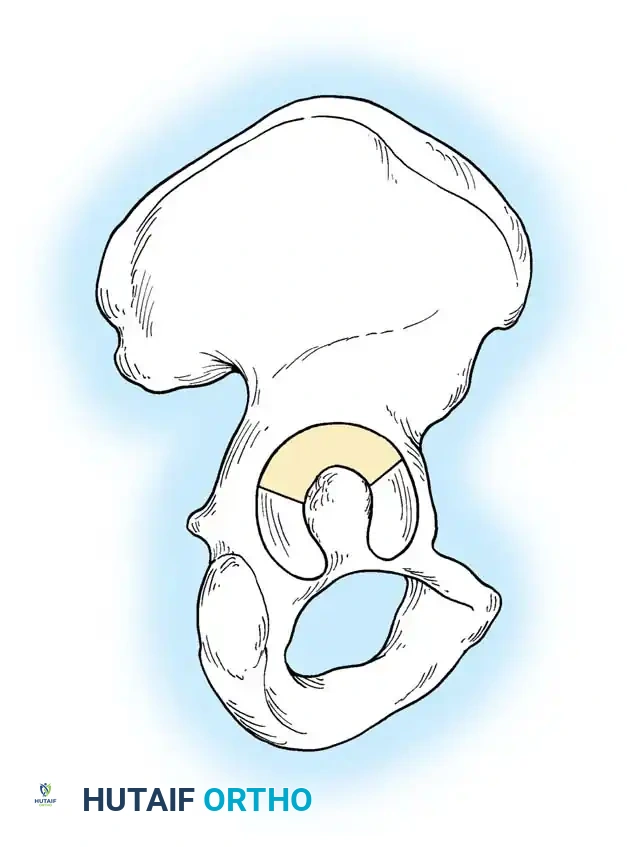
Medial to the acetabulum lies the quadrilateral surface (or quadrilateral plate), a thin, flat plate of bone forming the lateral wall of the true pelvis.
Directly overlying the femoral head anteriorly is the iliopectineal eminence. Because both the quadrilateral surface and the iliopectineal eminence are extremely thin, they offer poor purchase for standard cortical screws, necessitating specialized fixation techniques such as under-contoured spring plates or infra-pectineal plating.
Critical Neurovascular Structures
Surgical approaches to the acetabulum place several major neurovascular structures at risk:
- The Sciatic Nerve: Exits the pelvis through the greater sciatic notch, typically inferior to the piriformis muscle. It is highly susceptible to injury during posterior fracture-dislocations and during the Kocher-Langenbeck surgical approach.
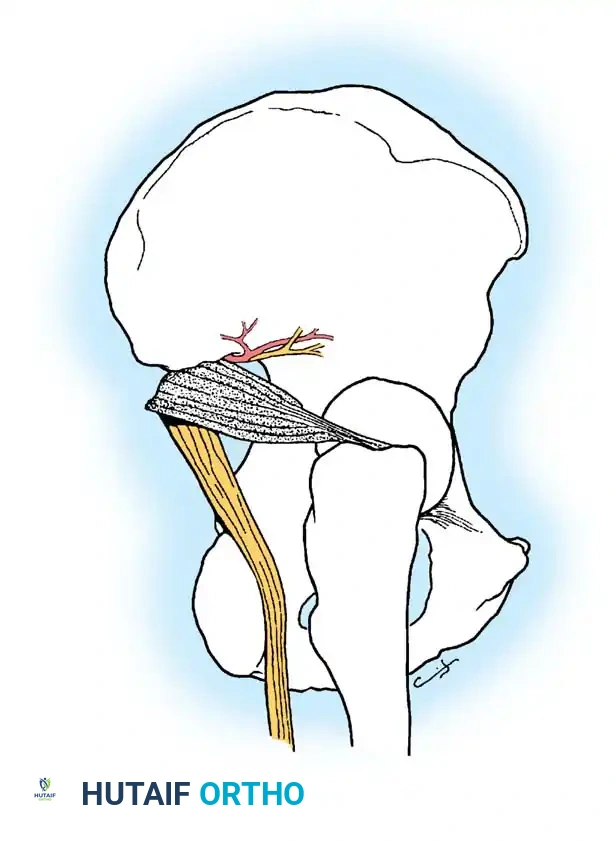
- The Superior Gluteal Artery and Nerve: Exit the greater sciatic notch at its most superior apex. Fractures extending into the apex of the notch can lacerate this artery, leading to massive, life-threatening retroperitoneal hemorrhage. Preoperative angiography and embolization may be required if active extravasation is identified.
- The Corona Mortis: A critical vascular anastomosis between the external iliac (or inferior epigastric) system and the obturator system, coursing over the superior pubic ramus. Tornetta et al. demonstrated that this anastomosis is present in up to 84% of hemipelves. Failure to identify and ligate the corona mortis during the ilioinguinal or modified Stoppa approach can result in catastrophic hemorrhage that retracts into the true pelvis.
Radiographic Evaluation
Accurate classification and surgical planning rely on a standardized radiographic series, supplemented by advanced cross-sectional imaging.
Standard Pelvic Radiography and Judet Views
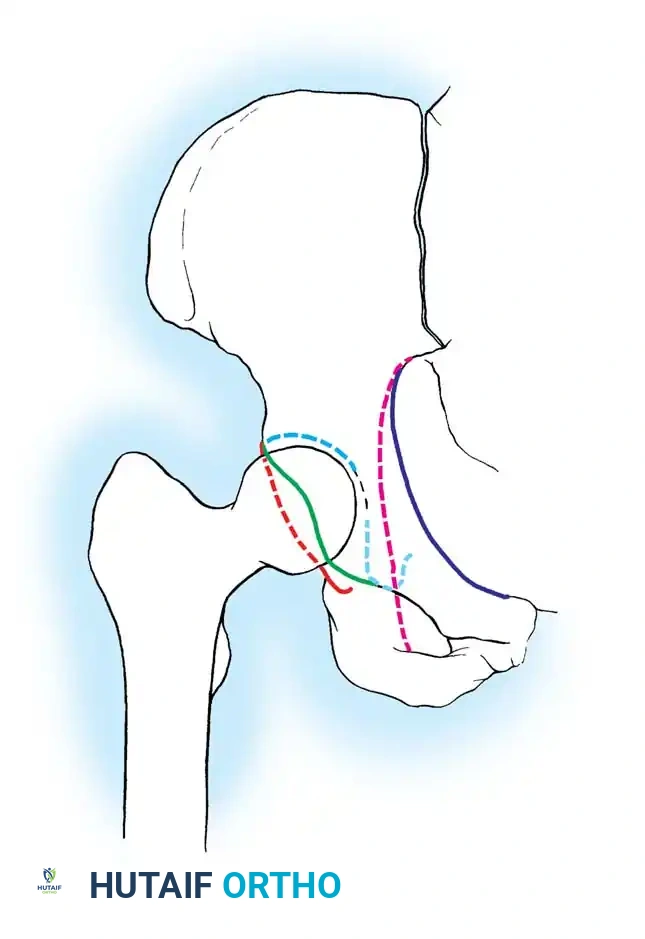
The initial evaluation begins with an Anteroposterior (AP) view of the pelvis. This view assesses the six fundamental radiographic landmarks of the acetabulum:
1. Iliopectineal line (Anterior column)
2. Ilioischial line (Posterior column)
3. Radiographic teardrop (Medial wall)
4. Acetabular roof (Weight-bearing dome)
5. Anterior lip of the acetabulum
6. Posterior lip of the acetabulum
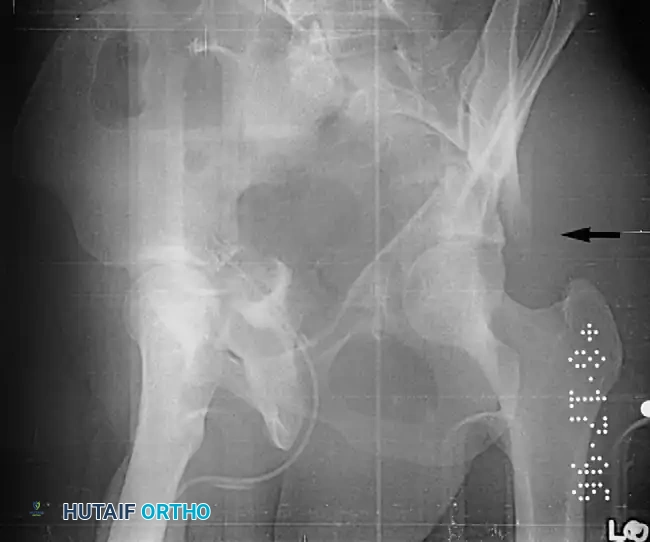
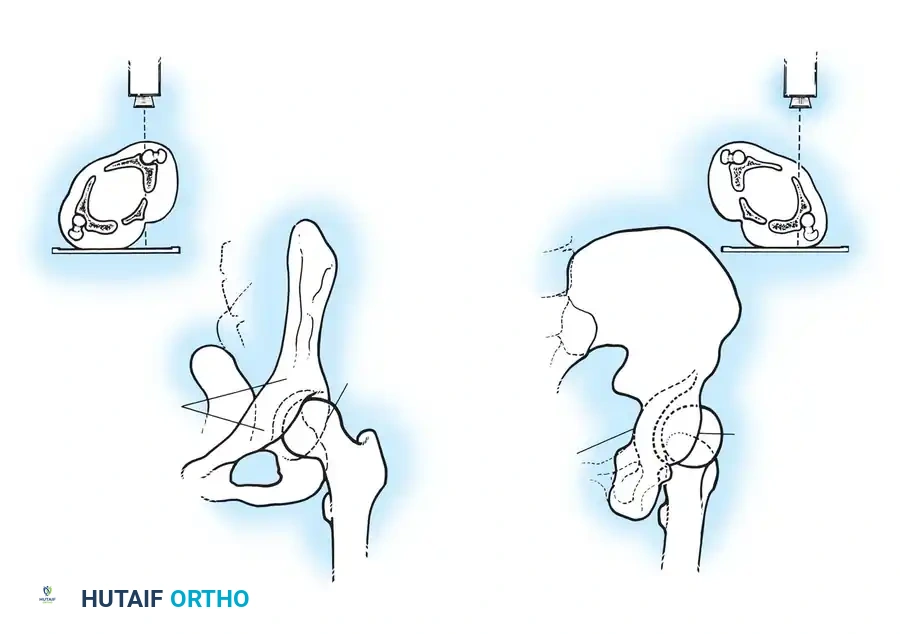
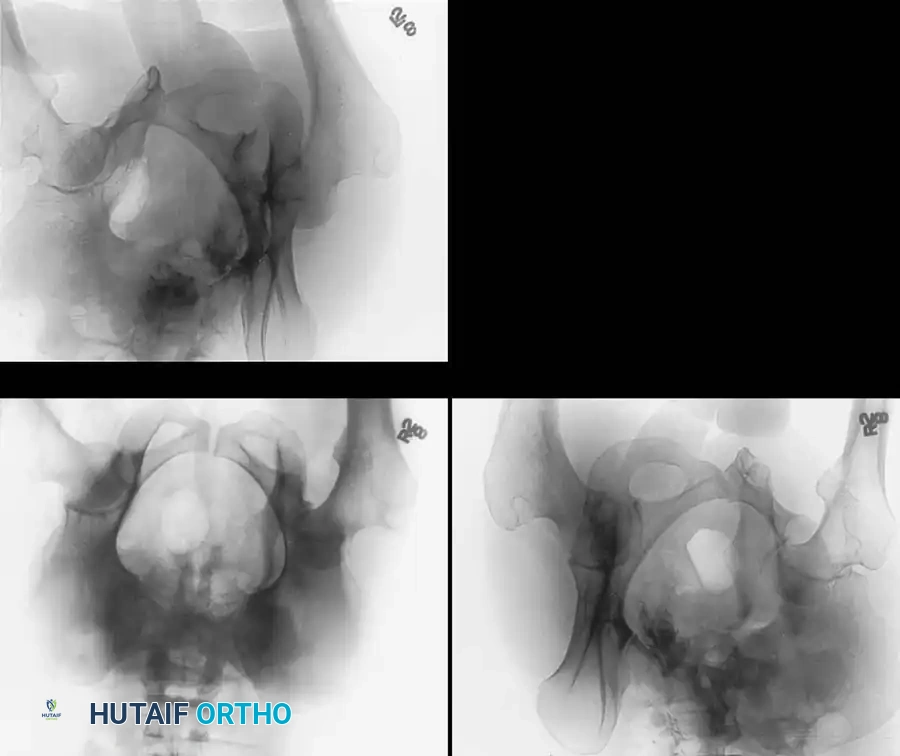
To fully conceptualize the fracture in three dimensions, the 45-degree oblique views described by Judet are mandatory:
* Iliac Oblique View: The patient is rolled 45 degrees toward the uninjured side. This view profiles the posterior column and the anterior wall of the acetabulum.
* Obturator Oblique View: The patient is rolled 45 degrees toward the injured side. This view profiles the anterior column and the posterior wall of the acetabulum.
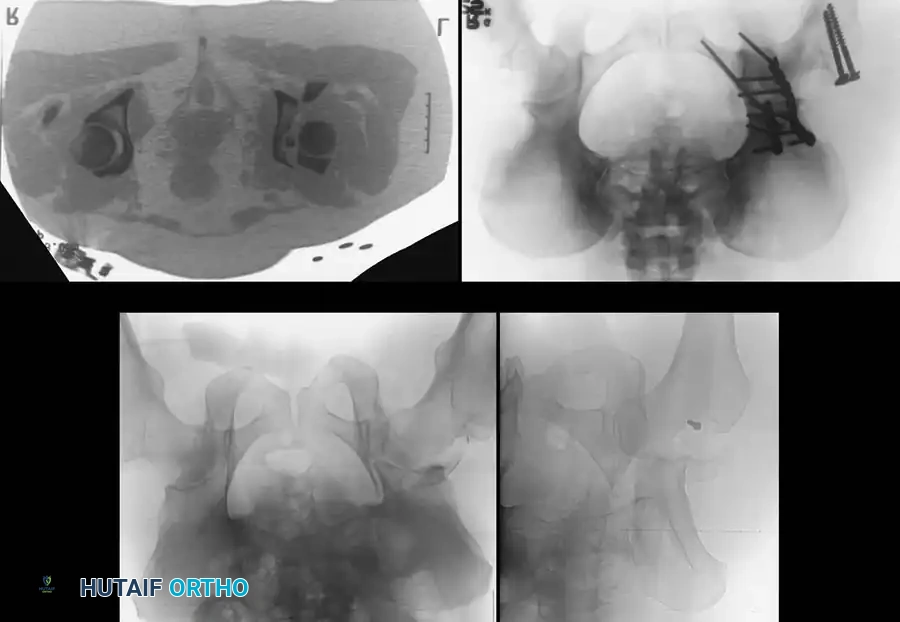
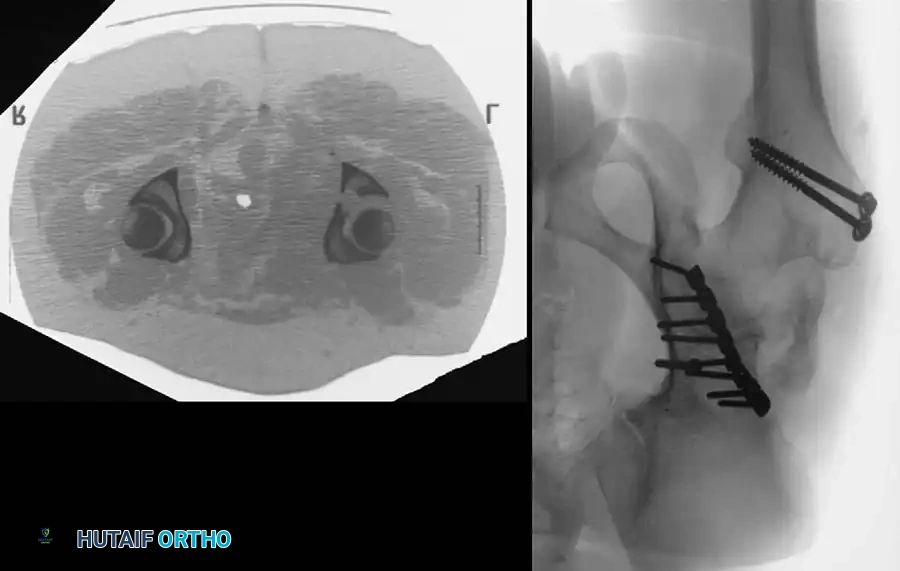
Advanced Imaging: Computed Tomography (CT)
While plain radiographs provide the foundation for classification, fine-cut CT scanning with 2D multiplanar and 3D surface-rendered reconstructions is the gold standard for modern surgical planning.

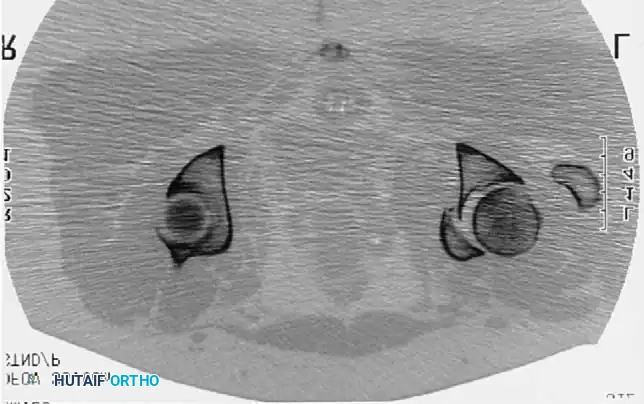
CT imaging excels at identifying:
* Intra-articular osteochondral fragments (loose bodies).
* Marginal impaction of the articular cartilage.
* The exact size and comminution of posterior wall fragments.
* The orientation of fracture lines to plan optimal screw trajectories.
Indications for Treatment
Indications for Nonoperative Management
Nonoperative management is reserved for a highly specific subset of fractures. The criteria, largely established by Matta, include:
1. Minimal Displacement: Less than 2 mm of displacement within the weight-bearing dome.
2. Intact Weight-Bearing Dome: Assessed via roof arc angles on CT or plain films. Medial, anterior, and posterior roof arc angles must be >45 degrees.
3. Joint Congruency: The femoral head must remain perfectly concentric with the intact portion of the acetabular roof on all radiographic views, both in and out of traction.
4. Absence of Intra-articular Fragments: No incarcerated bone or cartilage within the joint space.
Nonoperative protocols typically involve 6 to 8 weeks of strict toe-touch weight-bearing, aggressive deep vein thrombosis (DVT) prophylaxis, and serial radiographic monitoring to ensure no secondary displacement occurs.
Indications for Operative Management
Operative intervention is indicated for:
* Displacement > 2 mm in the weight-bearing dome.
* Incongruency of the hip joint (subluxation).
* Incarcerated intra-articular fragments.
* Posterior wall fractures involving > 20% of the articular surface or demonstrating dynamic instability on examination under anesthesia.
* Ipsilateral femoral fractures requiring mobilization.
Surgical Approaches
The choice of surgical approach is dictated entirely by the fracture pattern (classified via the Letournel and Judet system) and the location of maximal displacement.
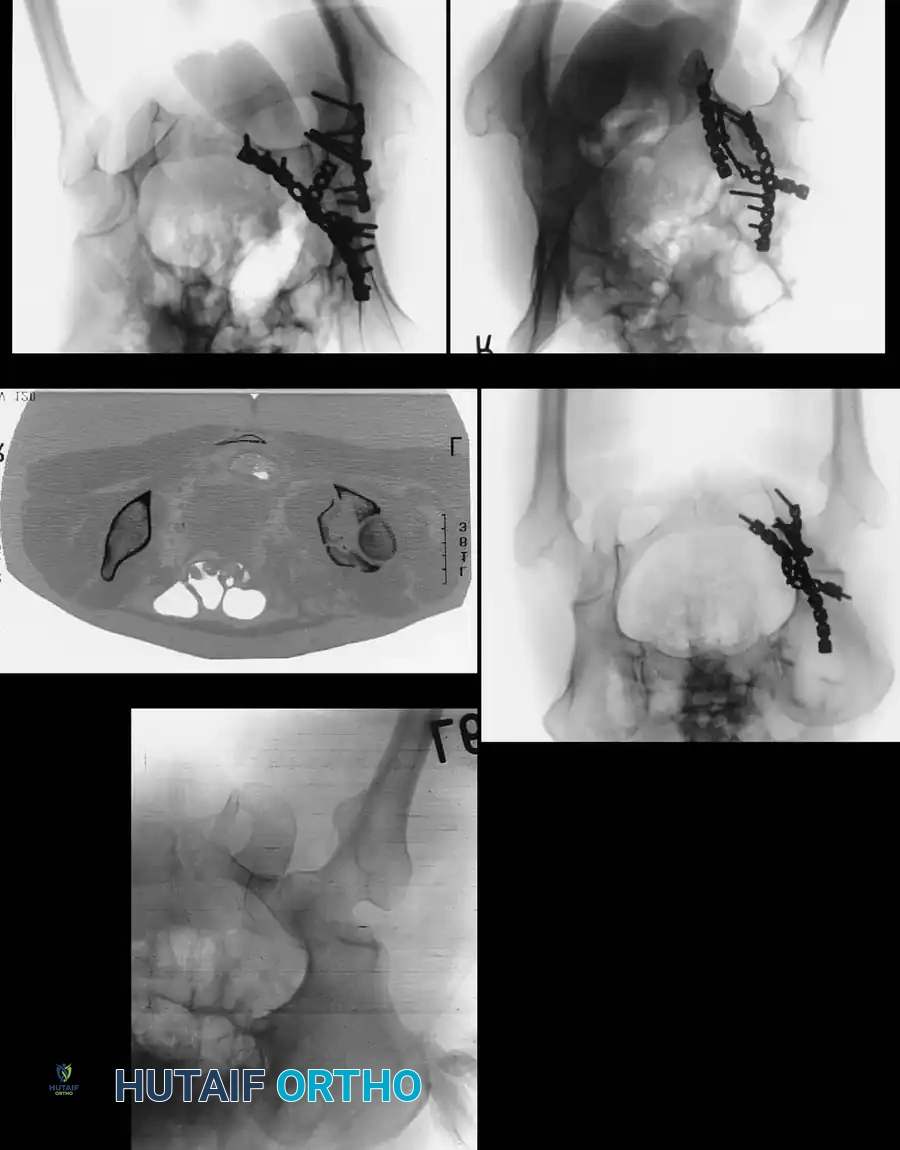
The Kocher-Langenbeck Approach
The Kocher-Langenbeck is the work
Associated Surgical & Radiographic Imaging














You Might Also Like

