Posterior Cruciate Ligament-Retaining TKA: Navigating Pitfalls
Key Takeaway
This article provides essential research regarding Posterior Cruciate Ligament-Retaining TKA: Navigating Pitfalls. Posterior cruciate ligament-retaining total knee arthroplasty (TKA) is indicated for end-stage joint destruction with a structurally intact PCL, fixed flexion under 30°, varus under 20°, and valgus under 25°. It is contraindicated with severe fixed deformities, PCL absence or degeneration, or technical inability to properly balance the PCL.
P ITFALLS
-
Contraindications include severe fixed deformities; anatomic abnormality, degeneration,
or absence of the PCL; and technical inability to properly balance the PCL.
PCL-Retaining TKA
Indications
1. End-stage joint destruction due to osteoarthritis, or due to primary synovial conditions, crystal deposition disease, rheumatoid arthritis and other inflammatory arthritides, osteonecrosis, and posttraumatic arthritis
2. Structurally intact posterior cruciate ligament (PCL)
3. Fixed flexion of less than 30°
4. Varus of less than 20°
Controversies
1. The surgeon’s ability to balance the PCL is critically important.
2. A PCL that is too tight may result in decreased range of motion and abnormal
polyethylene wear patterns, and may be a source of pain.
3. A PCL that is too loose may result in anterior-posterior instability causing pain, effusion, malfunction, and poor wear characteristics due to increased contact stresses.
5. Valgus of less than 25°
6. Joint subluxation of less than 1 cm
7. Technical ability of the surgeon
Examination/Imaging
8. In addition to examination of the knee, a thorough general history and physical examination are essential to ensure symptoms are indeed originating from the knee joint.
9. Any previous knee surgeries or injuries need to be documented.
10. It is essential to determine the presence of any chronic or acute infections that require treatment prior to joint replacement surgery.
Treatment Options
1. When possible, nonoperative management (activity modifications, injections, oral anti-inflammatory and/or pain medications, weight loss, etc.) should be entertained before total joint replacement.
11. Examination of the knee should include accurate range of motion, documentation of any flexion contracture, stability of the joint and integrity of ligamentous structures (in particular the PCL by posterior drawer testing or presence of posterior sag), and patellar tracking.
12. Plain radiographs
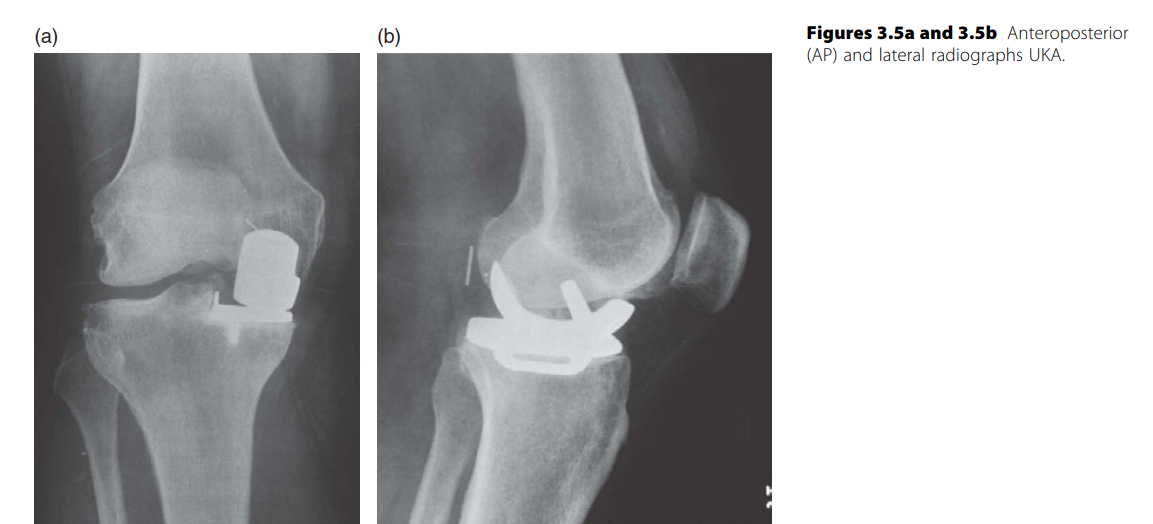
1. Standing anteroposterior and lateral views, with patellar views
2. Long-leg standing hip-to-ankle views to evaluate overall alignment of the limb.
Surgical Anatomy
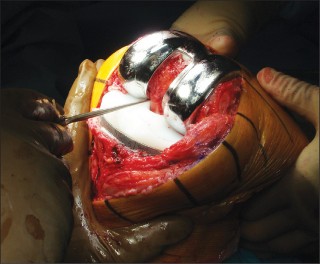
13. Tibial attachment of the PCL is posterior and distal to the tibial plateau, making that structure vulnerable to injury during the tibial bone resection.
14. Excessive bone resection from the proximal tibia or a large posteriorly sloped cut may jeopardize the tibial attachment of the PCL. Posterior tibial slope should not exceed 10°.
15. It is also possible to injure the PCL during correct tibial resection by making an overaggressive cut with the saw blade traveling too far posterior.
16. The PCL can be protected during the tibial resection by placing an osteotome anterior to it (Fig. 1).
PCL-Retaining TKA
FIGURE 1 27
Positioning
1. Supine positioning on standard operating room table is used.
2. A thigh-high tourniquet should be utilized.
P EARLS
- If possible, incisions from previous procedures should be used.
-
Large skin flaps and undermining of the subcutaneous tissues should be avoided, as this can lead to devascularization of skin margins.
Portals/Exposures - Routine surgical exposure for total knee arthroplasty (TKA) should be utilized.
- This typically involves an anterior longitudinal skin incision just medial to the midline followed by medial parapatellar arthrotomy.
- Following the skin incision, dissection is continued directly to the interval between the quadriceps tendon and the vastus medialis.
- The quadriceps tendon is incised sharply in one layer, leaving several millimeters of tendon attached to the vastus medialis to allow tendon-to-tendon closure at the conclusion of the procedure.
- The medial parapatellar arthrotomy continues with the capsular incision extending around the medial aspect of the patella, extending just medial and distal to the tibial tubercle.
- Approximately 1 cm of soft tissue medial to the tibial tubercle is preserved to allow repair of the capsule at the time of closure. 28 ## P EARLS
- Maintenance of the correct epicondylar axis of the femur is critical to ensure correct patellar tracking and extensor mechanism function, improve knee kinematics, and minimize the need for collateral ligament releases (Fig. 3).
- Femoral notchplasty can help avoid impingement of the PCL (Fig. 4).
- Posterior femoral osteophytes should be removed to remove tension from the posterior capsule (Fig. 5) and prevent flexion contracture (Fig. 6A and 6B).
PCL-Retaining TKA
Procedure
Step 1
- After exposure of the knee joint, the bone cuts are performed (femur-first or tibia-first according to surgeon preference).
- In the absence of a flexion contracture and to most accurately reproduce the joint line, the distal femoral cut should be 2 mm less than the thickness of the actual femoral component.
- This will account for lost distal femoral articular cartilage, and minimize the chance of creating an imbalance in the femoral-tibial gaps.
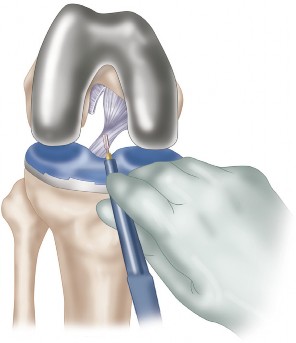
- The amount of proximal tibia removed from the less involved plateau should be equal to the composite thickness of the tibial component.
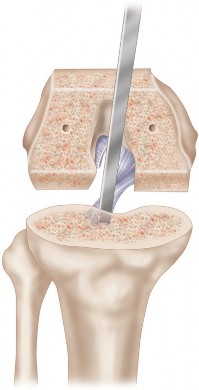
-
Once the tibial plateau bone has been removed, any remaining bone island anterior to the PCL can be trimmed to allow flush placement of the tibial component (Fig. 2).
--- FIGURE 2
--- FIGURE 3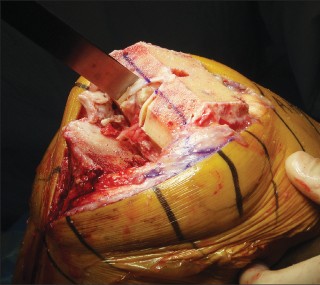
--- 29
PCL-Retaining TKA FIGURE 4 FIGURE 5


A B
FIGURE 6 30
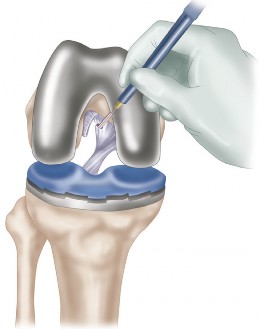
## P EARLS
1.
PCL tension is best tested with the trial components in place.
PCL-Retaining TKA
Step 2
You Might Also Like