Hand Infections: Principles, Diagnosis, and Surgical Management
Key Takeaway
Hand infections require prompt diagnosis and aggressive surgical management to prevent devastating functional loss. This guide details the anatomical factors, microbiological profiles, and systemic considerations influencing infection spread. It provides an evidence-based approach to empirical antibiotic therapy, differential diagnosis, and step-by-step surgical techniques for incision and drainage, ensuring optimal outcomes for complex hand infections.
Introduction to Hand Infections
Hand infections represent a critical category of orthopedic emergencies that demand prompt recognition, precise anatomical knowledge, and aggressive surgical and medical intervention. The unique and intricate anatomy of the hand—characterized by tightly compartmentalized spaces, synovial sheaths, and a delicate balance of gliding structures—renders it highly susceptible to the rapid spread of infection. Delay in treatment or inadequate surgical débridement can lead to devastating consequences, including tendon rupture, joint destruction, osteomyelitis, and irreversible loss of hand function.
The clinical course of most hand infections is dictated by a triad of variables: the anatomical characteristics of the hand, the virulence and inoculum size of the invading pathogen, and the systemic immunocompetence of the host. Successful management relies on a systematic approach encompassing accurate microbiological identification, targeted antimicrobial therapy, and meticulous surgical decompression and débridement.
Factors Influencing Hand Infections
Anatomical Considerations
The structural design of the hand facilitates precise motor function but paradoxically provides distinct pathways for the propagation of infection. Key anatomical factors that determine the localization and spread of purulence include:
- Superficial Soft Tissue Envelope: The dorsal skin and subcutaneous tissues are thin and highly compliant, allowing for significant edema accumulation. Conversely, the palmar skin is thick, tethered by dense fascial septa, and highly unyielding, which drives palmar infections deep into the fascial spaces rather than allowing superficial decompression.
- Closed Spaces of the Distal Pulp: The volar aspect of the distal phalanx is divided into multiple small, closed compartments by dense fibrous septa extending from the periosteum to the dermis. Infection in this space (a felon) rapidly increases compartmental pressure, leading to microvascular compromise, ischemic necrosis of the pulp, and secondary osteomyelitis of the distal phalanx.
- Flexor Tendon Sheaths: The synovial sheaths surrounding the flexor tendons lie in intimate proximity to the phalanges and interphalangeal joints. Purulence within these sheaths (suppurative flexor tenosynovitis) can rapidly destroy the gliding mechanism and compromise the tendon's blood supply via the vincula.
- Bursal Connections: The proximal extent of the flexor sheaths of the thumb and small finger frequently communicate with the radial and ulnar bursae, respectively. These bursae extend proximally into the palm and wrist, creating a conduit for a "horseshoe abscess" that can spread into the space of Parona (the deep fascial space of the distal forearm, located between the pronator quadratus and the deep flexor tendons).
- Deep Fascial Spaces: The thenar and midpalmar spaces are potential spaces within the hand that can harbor massive amounts of purulence, often presenting with profound dorsal edema due to the lymphatic drainage patterns of the hand.
Local and Systemic Factors
Local Factors:
The nature of the initial injury heavily influences the infection risk. Extensive soft-tissue crush injuries, high-velocity trauma, and the presence of devitalized tissue provide an ideal nidus for bacterial proliferation. Furthermore, the amount of bacterial contamination and the persistence of foreign bodies (e.g., wood splinters, glass, soil) significantly increase the likelihood of a recalcitrant infection.
Systemic Factors:
Host immunocompetence is a primary determinant of infection severity. Systemic factors that predispose patients to aggressive or atypical hand infections include:
* Diabetes mellitus (frequently associated with polymicrobial infections and impaired microcirculation).
* Intravenous drug abuse (predisposing to MRSA, atypical organisms, and necrotizing fasciitis).
* Malnutrition and chronic alcoholism.
* Long-term use of corticosteroids or immunomodulators (e.g., anti-TNF-α medications).
* Immunosuppression secondary to solid organ or bone marrow transplantation.
* Human Immunodeficiency Virus (HIV) infection.
Clinical Pearl: In diabetic patients or those with profound immunosuppression, the classic signs of inflammation (erythema, calor, dolor) may be blunted. A high index of suspicion and a lower threshold for surgical exploration are mandatory in these populations.
Anatomy of the Perionychium and Distal Pulp
Understanding the microanatomy of the distal digit is essential for managing common infections such as paronychia and felons. The perionychium consists of the nail bed (germinal and sterile matrices) and the surrounding soft tissues (eponychium and paronychium).
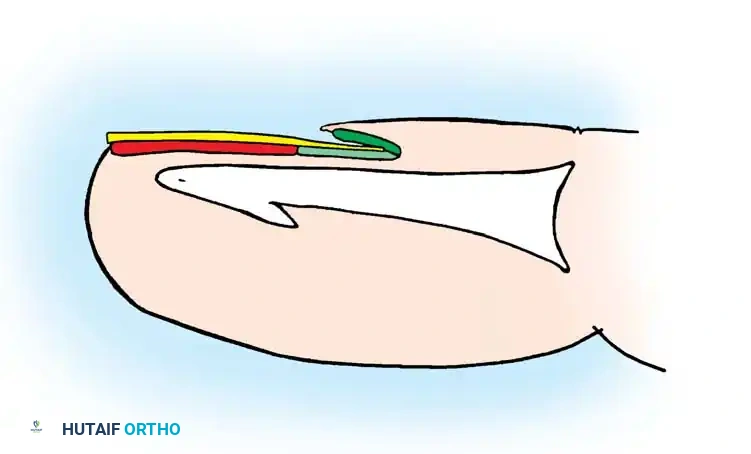
Infections in this region often begin in the lateral nail fold (paronychia) and can track proximally under the eponychial fold or beneath the nail plate itself, necessitating partial or complete nail plate removal for adequate drainage.
General Approach to Hand Infections
Clinical Evaluation
A meticulous history and physical examination are paramount. The surgeon must determine the exact mechanism of injury, the time elapsed since the onset of symptoms, and any specific environmental exposures (e.g., animal bites, marine environments, soil).
Physical examination should systematically assess:
* Location and Extent: Identify the epicenter of the infection and map its proximal spread.
* Swelling and Erythema: Note the presence of lymphangitis (erythematous streaking) and regional lymphadenitis (epitrochlear or axillary adenopathy).
* Joint and Tendon Involvement: Assess for Kanavel's cardinal signs of flexor tenosynovitis (fusiform swelling, flexed resting posture, tenderness along the flexor sheath, and severe pain with passive extension).
Differential Diagnosis: The Non-Infectious Mimics
Not all erythematous, swollen hands are infected. Misdiagnosing an inflammatory condition as an infection can lead to unnecessary surgical interventions. The differential diagnosis includes:
* Crystal Arthropathies: Gout and pseudogout can present with acute, severe erythema and swelling mimicking septic arthritis or cellulitis.
* Acute Calcific Periarthritis: Often presents with acute pain and localized erythema, typically near the insertion of the flexor carpi ulnaris or collateral ligaments.
* Pyoderma Gangrenosum: A neutrophilic dermatosis that can rapidly ulcerate and worsen with surgical débridement (pathergy).
* Sweet Syndrome: An acute febrile neutrophilic dermatosis that can affect the hand, presenting with tender, erythematous plaques resembling an abscess.
* Other Mimics: Foreign body reactions, herpetic whitlow (which should not be incised), metastatic lesions, silicone synovitis, granuloma annulare, and reactions to intravenous chemotherapeutic agents.
Diagnostic Imaging and Laboratory Analysis
- Radiographs: Standard anteroposterior, lateral, and oblique views are mandatory to rule out fractures, retained radiopaque foreign bodies, subcutaneous gas (suggestive of clostridial or necrotizing infections), and osteomyelitis (though bony changes may lag clinical infection by 10-14 days).
- Advanced Imaging: Ultrasound is highly effective for identifying localized fluid collections (abscesses) and guiding aspiration. Magnetic Resonance Imaging (MRI) with contrast is the gold standard for delineating deep fascial space infections, osteomyelitis, and occult tenosynovitis, though it should not delay emergent surgical intervention.
- Laboratory Studies: A complete blood count (CBC) with differential, serum C-reactive protein (CRP), and erythrocyte sedimentation rate (ESR) provide a baseline to monitor the systemic inflammatory response and the efficacy of treatment.
- Microbiology: Any fluid or tissue obtained must be sent for Gram stain, aerobic and anaerobic cultures, and antibiotic susceptibility testing. In chronic or atypical cases, specific requests for mycobacterial (AFB) and fungal cultures are required.
Microbiology of Hand Infections
The microbiological profile of hand infections is evolving, with a notable increase in polymicrobial presentations and antibiotic-resistant strains.
- Common Pathogens: Staphylococcus aureus remains the most frequently isolated organism in community-acquired hand infections. However, up to 80% of wounds cultured via swab yield multiple organisms, whereas deep tissue specimens typically isolate a single causative pathogen in 75% of cases. Other common isolates include Streptococcus species, enterobacteria, Pseudomonas, Enterococcus, and Bacteroides.
- Methicillin-Resistant S. aureus (MRSA): The prevalence of community-acquired MRSA has surged, necessitating the empirical use of agents like vancomycin, clindamycin, or trimethoprim-sulfamethoxazole in endemic areas.
- Exposure-Specific Pathogens:
- Cat and Dog Bites: Pasteurella multocida (rapid onset, intense inflammatory response).
- Human Bites (Clenched Fist Injuries): Eikenella corrodens, alongside S. aureus and oral anaerobes.
- Freshwater Exposure: Aeromonas hydrophila.
- Marine/Saltwater Exposure: Vibrio vulnificus and Mycobacterium marinum.
- Pediatric Populations (2 months to 3 years): Haemophilus influenzae (though decreasing due to vaccination).
- Surgical Site Infections: Postoperative infections are predominantly caused by gram-positive organisms (S. aureus, Staphylococcus epidermidis), though gram-negative bacilli are increasingly isolated.
Pharmacological Management
Initial antibiotic therapy is typically empirical, guided by the Gram stain, the clinical presentation, and local antibiograms. Once culture and sensitivity results are available, therapy must be narrowed to the most effective, least broad-spectrum agent.
Surgical Warning: Antibiotics are an adjunct to, not a replacement for, adequate surgical drainage. Failure to recognize the polymicrobial nature of an infection or inadequate surgical débridement are the most frequent causes of treatment failure.
Antibiotic Selection Guidelines
- Penicillins: Natural penicillins (Penicillin G) remain effective for Streptococcus viridans and Pasteurella (bite wounds). Penicillinase-resistant penicillins (Nafcillin) are excellent for susceptible staphylococcal osteomyelitis. Amoxicillin-clavulanate provides robust first-line oral coverage for human/animal bites and diabetic hand infections.
- Cephalosporins: First-generation agents (Cefazolin, Cephalexin) are standard for prophylaxis and simple gram-positive infections. Third-generation agents (Ceftriaxone) are utilized for gonococcal tenosynovitis, while Ceftazidime covers Pseudomonas.
- Glycopeptides and Oxazolidinones: Vancomycin (IV) is the workhorse for severe MRSA infections. Linezolid offers excellent oral bioavailability and bone penetration for VRE and MRSA.
- Fluoroquinolones: Ciprofloxacin and Levofloxacin provide broad gram-negative coverage and excellent bone penetration, making them useful for osteomyelitis, though they should be used judiciously due to tendon rupture risks.
- Lincosamides: Clindamycin covers staphylococci and anaerobes, serving as a valuable alternative for penicillin-allergic patients, though it carries a risk of Clostridium difficile colitis.
Antifungal and Antiviral Agents
- Antifungals: Polyenes (Amphotericin B) are reserved for severe systemic fungal infections. Azoles (Fluconazole, Itraconazole) are well-tolerated for systemic use. Terbinafine is the systemic drug of choice for severe onychomycosis.
- Antivirals: Acyclovir or Valacyclovir are utilized for the treatment and prophylaxis of herpetic whitlow. It is critical to differentiate herpetic whitlow (vesicular lesions, clear fluid) from a bacterial felon, as incising a herpetic lesion can lead to viral dissemination and secondary bacterial superinfection.
Surgical Management: Principles of Incision and Drainage
When an abscess is present, or when an infection fails to respond to 24-48 hours of appropriate intravenous antibiotics, surgical incision and drainage (I&D) is mandated. The goal is to evacuate purulence, decompress tight fascial compartments, excise necrotic tissue, and obtain deep tissue cultures.
Preoperative Preparation and Positioning
- Anesthesia: General anesthesia or a distant regional block (e.g., axillary or supraclavicular brachial plexus block) is strongly recommended.
- Pitfall: Local infiltration directly into the infected area must be avoided. The acidic environment of infected tissue neutralizes local anesthetics, rendering them ineffective. Furthermore, injecting volume into an already compromised, swollen space can precipitate ischemia and mechanically disseminate bacteria into adjacent uninfected planes.
- Tourniquet Application: A pneumatic tourniquet is essential for a bloodless surgical field, allowing precise identification of neurovascular structures.
- Critical Step: Prior to inflation, elevate the hand and arm for 3 to 6 minutes to allow for gravity exsanguination. Do not use an elastic wrap (Esmarch bandage) to exsanguinate the limb, as the mechanical compression can force purulence proximally into the forearm or systemic circulation.
Operative Technique (Technique 75-1)
- Incision Design: Make the skin incision based on the specific anatomical compartment involved. Incisions should be extensile, avoid crossing flexion creases at right angles (to prevent flexion contractures), and be placed in mid-axial lines when approaching the digits.
- Blunt Dissection: Once the dermis is incised, immediately transition to blunt dissection using a hemostat or blunt scissors. Spread the deeper structures parallel to the neurovascular bundles and tendons to avoid iatrogenic injury.
- Evacuation and Culturing: Upon entering the abscess cavity, immediately obtain deep tissue and fluid specimens for aerobic, anaerobic, mycobacterial, and fungal cultures. Swabs are inferior to actual tissue biopsies.
- Débridement: Excise all frankly necrotic skin, subcutaneous tissue, and devitalized fascia. In cases of necrotizing fasciitis, radical excision back to bleeding, healthy tissue is life-saving.
- Irrigation: Copious irrigation is critical to decrease the bacterial load. Use a pulsatile lavage system or high-volume syringe irrigation with normal saline. The mechanical flushing action is more important than the addition of antibiotic solutions to the irrigant.
- Wound Management: An incision for drainage creates an open wound that must heal by secondary intention or delayed primary closure.
- Do not close infected wounds primarily.
- Pack the wound loosely with moist gauze or utilize a small Penrose drain or pediatric feeding tube to maintain patency of the drainage tract.
- In severe cases, application of a negative pressure wound therapy (NPWT) device may be considered after gross purulence is controlled, though its use in acute hand infections requires caution to avoid exposing vital structures.
Postoperative Protocol
- Immobilization: Postoperatively, the hand should be immobilized in a bulky, non-compressive dressing with a volar plaster splint. The hand is placed in the "position of safe immobilization" (intrinsic-plus position): wrist extended 20-30 degrees, metacarpophalangeal (MCP) joints flexed 70-90 degrees, and interphalangeal (IP) joints in full extension. This prevents collateral ligament contracture.
- Elevation: Strict elevation of the hand above the level of the heart is mandatory to reduce edema, improve microcirculation, and decrease pain.
- Rehabilitation: Once the acute infection is controlled (typically 48-72 hours postoperatively), the splint is removed, and aggressive active and passive range-of-motion exercises are initiated under the guidance of a certified hand therapist. Early mobilization is the key to preventing tendon adhesions and permanent joint stiffness.
- Antibiotic Duration: Intravenous antibiotics are transitioned to oral agents once clinical improvement is noted (decreased erythema, resolving edema, normalized inflammatory markers). The total duration of therapy is dictated by the severity of the infection and the presence of bone or joint involvement (e.g., 1-2 weeks for soft tissue, 4-6 weeks for osteomyelitis).
You Might Also Like
