Proximal Phalanx Fracture: What's the Best Treatment?
Introduction & Epidemiology
Proximal phalanx fractures represent a significant portion of hand fractures, accounting for approximately 10% of all upper extremity fractures. These injuries are prevalent across all age groups but are particularly common in younger, active individuals involved in sports or work-related activities. The unique anatomy of the proximal phalanx, with its critical role in digital motion, grip, and pinch, dictates that even seemingly minor displacements can lead to substantial functional deficits if not managed appropriately. The goal of treatment, whether operative or non-operative, is to achieve stable anatomical reduction, preserve articular congruity, and facilitate early mobilization to prevent post-traumatic stiffness, which is the most debilitating complication. A thorough understanding of fracture morphology, associated soft tissue injuries, and patient-specific factors is paramount for optimizing outcomes.
Surgical Anatomy & Biomechanics
The proximal phalanx is the longest of the three phalanges in each digit, forming the metacarpophalangeal (MCP) joint proximally and the proximal interphalangeal (PIP) joint distally. Its anatomy is critical to digital function.
Bony Anatomy
- Base: Articulates with the metacarpal head, forming a condyloid joint. The palmar plate and collateral ligaments attach here, contributing to MCP joint stability.
- Shaft: Cylindrical proximally, flattening distally. Fractures here are susceptible to angular and rotational deformities due to muscle forces.
- Head: Forms two condyles that articulate with the base of the middle phalanx, creating a hinge joint (PIP). The collateral ligaments and accessory collateral ligaments attach to the head, providing crucial PIP joint stability.
Soft Tissue Attachments and Biomechanics
- Extensor Mechanism: The central slip of the extensor digitorum communis (EDC) inserts into the base of the middle phalanx, traversing the dorsal aspect of the proximal phalanx. The lateral bands, formed by the lumbricals and interossei, merge dorsally to form the terminal tendon. Fractures of the proximal phalanx can disrupt this intricate mechanism, leading to extensor lag or boutonnière deformities. The interossei and lumbricals attach to the base and shaft of the proximal phalanx.
- Flexor Tendons: The flexor digitorum superficialis (FDS) inserts into the middle phalanx, while the flexor digitorum profundus (FDP) continues to the distal phalanx. The flexor tendons run within a fibro-osseous sheath along the palmar aspect of the proximal phalanx. Swelling and adhesions around the fracture site can restrict tendon glide, leading to significant functional impairment.
- Collateral Ligaments: The proper and accessory collateral ligaments of the MCP and PIP joints are critical stabilizers. Injury to these structures or malunion of the phalanx can lead to joint instability or restricted motion.
-
Muscle Forces:
The intrinsic muscles (interossei and lumbricals) insert into the base of the proximal phalanx and lateral bands.
- Shaft Fractures: Depending on the fracture location, the deforming forces vary. Proximal shaft fractures (proximal to the insertion of the intrinsics) tend to apex volarly due to the pull of the intrinsics on the distal fragment and the extensor mechanism on the proximal fragment. Distal shaft fractures (distal to the intrinsic insertion) tend to apex dorsally due to the pull of the FDS/FDP.
- Rotational Deformity: This is a critical consideration. The natural cascade of the fingers (converging towards the scaphoid tubercle with MCP, PIP, and DIP joints flexed) must be preserved. Any rotational malunion is poorly tolerated functionally.

Indications & Contraindications
The decision-making process for proximal phalanx fractures involves a careful assessment of fracture characteristics, patient factors, and functional demands. The primary goal is to restore anatomical alignment and stability to allow for early, controlled motion and minimize complications.
Operative Indications
- Unstable Fractures: Any fracture that cannot be maintained in an acceptable position with closed reduction and casting/splinting. This includes fractures with significant displacement, comminution, or instability under stress.
- Irreducible Fractures: Fractures that cannot be anatomically reduced by closed means, often due to soft tissue interposition (e.g., volar plate, flexor tendon, collateral ligament).
- Open Fractures: Require surgical debridement, irrigation, and stabilization to prevent infection and promote healing.
- Articular Fractures: Intra-articular fractures with displacement or step-off of >1mm (especially in the condyles) to prevent post-traumatic arthritis and preserve joint mechanics.
-
Significant Angulation/Rotation:
- Angulation >10-20 degrees (varies by digit and location).
- Any perceptible rotational deformity (often assessed by comparing finger cascade).
- Polytrauma: May necessitate early surgical stabilization to facilitate overall patient care and rehabilitation.
- Pathologic Fractures: Fractures occurring through abnormal bone (e.g., tumor, osteomyelitis) may require biopsy and stabilization.
Non-Operative Indications
- Stable, Minimally Displaced Fractures: Fractures that maintain acceptable alignment after closed reduction, with minimal comminution and no rotational deformity.
- Closed, Non-Articular Fractures: With minimal or no displacement, or where displacement is clinically and radiographically insignificant.
- Patient Factors: Patients with significant comorbidities precluding surgery, or those who are non-ambulatory and have low functional demands for the affected hand.
- Lack of Rotational Deformity: Essential for successful non-operative management.
Summary of Indications: Operative vs. Non-Operative
| Feature / Indication | Operative Management | Non-Operative Management |
|---|---|---|
| Displacement | Significant (>2mm), unstable after reduction | Minimally displaced (<2mm), stable after reduction |
| Angulation | >10-20 degrees (depending on digit/location), apex volar/dorsal malalignment | <10-20 degrees, acceptable alignment |
| Rotation | Any perceptible rotational deformity (scissoring) | No rotational deformity |
| Articular Involvement | >1mm step-off or gap, comminution, unstable | <1mm step-off/gap, stable, non-displaced |
| Open Fracture | Always operative (debridement, stabilization) | N/A |
| Irreducibility | Due to soft tissue interposition | Easily reducible by closed means |
| Comminution | Significant, impacting stability and load-bearing | Minimal, stable comminution |
| Associated Injuries | Ligament avulsion, tendon entrapment, neurovascular compromise | Isolated fracture, no significant soft tissue injury |
| Patient Factors | Active, high functional demand, good surgical candidate | Elderly, low functional demand, significant comorbidities, non-compliant with rehab |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for achieving optimal outcomes and avoiding complications.
Pre-Operative Planning
- Clinical Assessment: Detailed history of injury mechanism, hand dominance, occupation, and functional demands. A thorough physical exam should assess for skin integrity, neurovascular status, rotational deformity (finger cascade), and any associated soft tissue injuries.
-
Imaging:
- Plain Radiographs: Standard anteroposterior, lateral, and oblique views of the affected digit are mandatory. Ensure the lateral view is true lateral to accurately assess displacement and angulation. Compare to the contralateral hand if normal anatomy is uncertain.
- Computed Tomography (CT): Indicated for complex intra-articular fractures (pilon fractures, condylar fractures) to delineate articular comminution, displacement, and guide surgical approach and implant selection.
- Magnetic Resonance Imaging (MRI): Rarely used for acute phalanx fractures but may be considered if significant soft tissue (ligament, tendon) injury is suspected that would alter management.
- Fracture Classification: Utilize a standardized classification system (e.g., AO/OTA) to describe the fracture type, location (base, shaft, head), and involvement (intra-articular, extra-articular). This aids in communication and prognosis.
-
Implant Selection:
Based on fracture pattern, location, and surgeon's preference. Options include:
- K-wires: Most versatile, simple, low profile. Used for stable fixation of shaft fractures, condylar fractures, and as temporary fixation.
- Mini-fragment Screws: Lag screws for transverse or oblique fractures, providing interfragmentary compression. Can be combined with K-wires or plates.
- Mini-fragment Plates and Screws: Dorsal plating is common for comminuted, unstable shaft fractures, or when K-wire fixation is insufficient. Locking plates offer angular stability in osteoporotic bone.
- External Fixation: Rarely used for simple proximal phalanx fractures, but may be considered for highly comminuted open fractures with significant soft tissue loss, or as a temporary measure.
- Tourniquet Time: Plan for a maximum of 90-120 minutes. Consider dual tourniquets for complex cases.
- Antibiotic Prophylaxis: Standard for open fractures and typically administered pre-incision for all operative cases.
Patient Positioning
- Anesthesia: Regional block (axillary, supraclavicular) combined with sedation, or general anesthesia.
- Position: Supine on the operating table.
- Arm Preparation: The affected arm is typically placed on a dedicated hand table.
- Tourniquet: An upper arm tourniquet is applied after appropriate padding.
- Sterile Field: The entire hand and forearm are prepped and draped to allow for full range of motion of the digits during intraoperative assessment, especially for rotational stability.
Detailed Surgical Approach / Technique
The choice of surgical approach and fixation technique depends heavily on the fracture pattern, location, and the surgeon's experience. The goal is to achieve stable anatomical reduction with minimal soft tissue stripping, allowing for early mobilization.
General Principles
- Gentle Tissue Handling: Minimize devascularization of bone fragments and soft tissue trauma.
- Anatomic Reduction: Crucial for restoring joint congruity and digital cascade.
- Stable Fixation: Sufficient to withstand early controlled motion.
Surgical Approaches
-
Dorsal Approach (Most Common):
- Incisions: Longitudinal or transverse (Bruner-type) incisions are typically employed. For shaft fractures, a longitudinal incision directly over the fracture site is common. For condylar fractures, a Y-shaped incision or parallel longitudinal incisions may be used.
-
Dissection:
- Skin and subcutaneous tissues are incised. Careful attention must be paid to preserve dorsal veins and sensory nerves.
- The extensor mechanism is identified. For shaft fractures, the extensor hood can be split longitudinally between the central slip and a lateral band. Alternatively, a portion of the sagittal band can be incised and reflected to expose the underlying phalanx.
- For proximal fractures near the MCP joint, the attachment of the sagittal bands to the extensor mechanism needs careful handling. For more distal fractures, reflection of the extensor mechanism may be required.
-
 - Elevate the periosteum cautiously to expose the fracture site.
- Advantages: Direct visualization of the dorsal and lateral surfaces, good access for plating.
- Disadvantages: Risk of extensor mechanism adhesions, boutonnière deformity if central slip is disrupted.
-
Lateral Approach:
- Incisions: Longitudinal incision along the mid-axial line of the finger.
- Dissection: Dorsal and volar neurovascular bundles are retracted. The collateral ligaments are identified. This approach may be suitable for condylar fractures where direct visualization of the articular surface is needed, or for inserting interfragmentary screws.
- Advantages: Less disruption to the extensor and flexor mechanisms.
- Disadvantages: Limited exposure, risk to neurovascular bundles.
-
Volar Approach:
- Generally avoided for shaft fractures due to the risk of adhesions to the flexor tendons and damage to the neurovascular bundles.
- May be indicated for rare volar plate avulsion fractures of the PIP joint or highly specific fracture patterns.
Reduction and Fixation Techniques
-
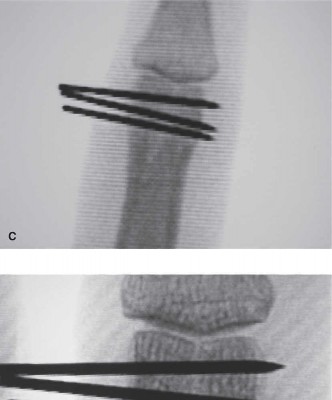
K-wire Fixation:
-
Technique:
After achieving closed or open reduction, K-wires (0.035" or 0.045") are drilled across the fracture site.
- Crossed K-wires: Two K-wires are inserted obliquely, crossing at the fracture site. This is common for transverse or short oblique shaft fractures.
- Oblique/Divergent K-wires: For long oblique or spiral fractures, multiple wires can be placed perpendicular to the fracture plane for interfragmentary compression.
- Intramedullary K-wires: Less common, but can provide axial stability, often supplemented with oblique wires.
- Pearls: Wires should be divergent, engage both cortices, and avoid damaging adjacent joints, tendons, or neurovascular structures. Wires are typically cut and bent outside the skin to allow for easy removal.
- Advantages: Simple, inexpensive, minimally invasive, allows for early mobilization in some stable patterns.
- Disadvantages: Less rigid fixation, risk of pin tract infection, potential for loss of reduction, tendon impingement.
-
Technique:
After achieving closed or open reduction, K-wires (0.035" or 0.045") are drilled across the fracture site.
-
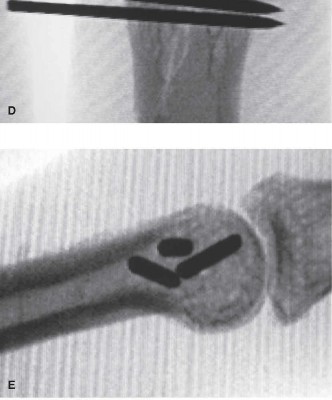
Mini-Fragment Screws (Interfragmentary Compression):
- Technique: Used for long oblique or spiral fractures where interfragmentary compression can be achieved. Typically 1.5mm or 2.0mm cortical screws.
- Lag Screw Principle: Overdrill the near cortex, glide hole in the near cortex, measure depth, tap far cortex, insert screw.
- Pearls: Requires meticulous technique to avoid stripping small bone fragments. Can be used in conjunction with K-wires or plates for additional stability.
- Advantages: Provides rigid fixation, allows for earlier mobilization, low profile.
- Disadvantages: Technically demanding, not suitable for highly comminuted fractures or short oblique patterns.
-
Mini-Fragment Plates and Screws (Dorsal Plating):
- Technique: After reduction, a small, low-profile dorsal locking plate (e.g., 1.3mm, 1.5mm, or 2.0mm systems) is contoured and applied to the dorsal surface of the phalanx. Screws are inserted through the plate into the phalanx.
- Locking Plates: Provide angular stability, particularly useful in comminuted fractures or osteoporotic bone, where purchase in cortical bone may be limited.
- Dynamic Compression Plates: Can be used to achieve interfragmentary compression.
- Pearls: Ensure careful contouring to avoid impingement on the extensor mechanism. Minimize soft tissue stripping during plate application.
-
 - Advantages: Very rigid fixation, allows for early active range of motion, excellent for comminuted or unstable fractures.
- Disadvantages: More invasive, higher risk of soft tissue adhesions, implant prominence, potential for hardware irritation requiring removal.
-
External Fixation:
- Technique: A small external fixator (e.g., mini-external fixator or a specially designed finger fixator) is applied to maintain length and alignment.
- Indications: Reserved for highly comminuted fractures, open fractures with significant soft tissue loss, or as a temporary measure when definitive internal fixation is delayed.
- Advantages: Allows for wound access, preserves length, avoids internal hardware at the fracture site.
- Disadvantages: Bulky, risk of pin tract infection, limited stability, potential for stiffness.
Intraoperative Assessment
- Radiographic Confirmation: Use intraoperative fluoroscopy to confirm reduction, alignment, and implant position in multiple planes.
- Stability Check: Assess stability of fixation manually.
- Range of Motion: Check full passive and active (if possible) range of motion of the MCP and PIP joints to ensure no impingement or restriction.
- Digital Cascade: Recheck rotational alignment with the hand fully flexed to ensure fingers converge naturally.
- Tourniquet Release: Release the tourniquet to check for hemostasis.
Wound Closure
- Meticulous wound closure in layers.
- Skin closure with fine sutures.
- Apply a sterile dressing and a protective splint.
Complications & Management
Proximal phalanx fractures, regardless of treatment method, carry a significant risk of complications, predominantly related to stiffness and malunion.
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Joint Stiffness (PIP, MCP) | 20-50% | Early controlled motion, intensive hand therapy, dynamic splinting, tenolysis/arthrolysis, capsulotomy, joint replacement (rare), fusion (salvage). |
| Malunion | 10-30% | If symptomatic (pain, limited ROM, scissoring): corrective osteotomy with internal fixation. Less severe may be managed with therapy. |
| Nonunion | 1-5% | Revision surgery with debridement, bone grafting (autograft/allograft), and rigid internal fixation (plate and screws). External fixation may be an option. |
| Hardware Complications | 5-15% | Pin tract infection (K-wires), hardware loosening/migration, plate prominence/irritation, tendon impingement. Removal of symptomatic hardware, antibiotics for infection. |
| Infection | <5% (closed) | Debridement, irrigation, culture-specific antibiotics. For deep infection, hardware removal may be necessary, followed by re-stabilization once infection is controlled. |
| Tendon Adhesions | 5-15% | Intensive hand therapy, dynamic splinting, tenolysis (surgical release of adhesions). |
| Nerve Injury | <1% | Careful dissection. If identified intraoperatively, primary repair. Post-op, observation for neurapraxia, neurolysis, or nerve graft for persistent deficit. |
| Extensor Lag / Boutonnière | 5-10% (post-op) | Intensive hand therapy, dynamic splinting (PIP extension), central slip repair/reconstruction. |
| CRPS (Complex Regional Pain Syndrome) | 2-10% | Early diagnosis and multi-modal treatment: pain management (medications, nerve blocks), hand therapy, psychological support. |
Management Principles
- Early Recognition: Vigilant post-operative monitoring and prompt investigation of symptoms.
- Aggressive Rehabilitation: The cornerstone of preventing and managing stiffness.
- Surgical Revision: Indicated for symptomatic malunion, nonunion, or persistent hardware complications. Timing is critical to balance bone healing with soft tissue recovery.
Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol is as critical as the surgery itself for optimizing functional outcomes. The overarching principle is early, controlled motion to prevent stiffness while protecting the healing fracture.
Initial Phase (Days 0-14)
-
Immobilization:
- A protective dorsal or volar splint is applied immediately post-operatively, holding the MCP joints in 60-70 degrees of flexion (to maintain collateral ligament length) and the PIP/DIP joints in slight flexion (10-20 degrees).
- The splint protects the fracture site and the surgical repair.
- Edema Control: Elevation of the hand, gentle massage, and active range of motion of uninvolved joints (shoulder, elbow, wrist) to minimize swelling.
- Pain Management: Oral analgesics as needed.
- Wound Care: Daily dressing changes as per protocol, monitor for signs of infection.
Early Motion Phase (Weeks 2-6)
- Initiation: Once radiographic stability is confirmed and pain allows, controlled active and passive range of motion exercises begin. Hand therapist involvement is crucial.
-
Exercises:
- MCP Joint: Active and passive flexion/extension. Maintaining MCP flexion helps prevent collateral ligament shortening.
- PIP/DIP Joints: Active and passive flexion/extension within the limits of stability. Often, dynamic splints (e.g., dynamic extension splint for PIP flexion contracture, dynamic flexion splint for PIP extension lag) are utilized to apply gentle, prolonged stretch.
- Tendon Gliding: Flexor and extensor tendon gliding exercises to prevent adhesions.
- Intrinsic/Extrinsic Stretching: As appropriate.
- Protection: The splint is used between exercise sessions and for protection during activities. Avoid heavy lifting or direct impact.
- K-wire Removal: K-wires are typically removed around 4-6 weeks post-op, once sufficient fracture healing is evident radiographically.
Strengthening and Return to Activity Phase (Weeks 6-12+)
- Progression: As fracture union progresses and pain subsides, rehabilitation advances to strengthening exercises.
-
Exercises:
- Grip Strengthening: Using putty, stress balls.
- Pinch Strengthening: Using small objects, pinch gauges.
- Functional Activities: Incorporating the hand into daily activities.
- Scar Management: Massage, silicone sheeting, desensitization techniques.
- Gradual Return: Slowly progress to work-specific or sport-specific activities. Full return to unrestricted activities may take 3-6 months, depending on the fracture severity and patient's demands.
- Hardware Removal: Plates and screws are generally left in situ unless they cause symptoms (e.g., irritation, tendon impingement), in which case removal is considered after 6-12 months.
Summary of Key Literature / Guidelines
Current management of proximal phalanx fractures is guided by principles established through decades of clinical experience and biomechanical studies, emphasizing anatomical reduction, stable fixation, and early mobilization.
- AO Principles: The Arbeitsgemeinschaft für Osteosynthesefragen (AO) Foundation's principles of fracture management (anatomic reduction, stable fixation, preservation of blood supply, early mobilization) are paramount in the treatment of hand fractures. For proximal phalanges, this often translates to achieving stable internal fixation that allows early, controlled range of motion.
-
K-wire Fixation vs. Plate Fixation:
- Traditional mainstay for stable patterns, especially transverse or short oblique shaft fractures, and some articular fractures. K-wires offer simplicity and lower invasiveness.
- Mini-fragment plating, particularly locking plates, have gained favor for unstable, comminuted, or segmental fractures, where rigid fixation is needed for early motion. Studies by authors like Fan et al. (2014) and others have demonstrated comparable functional outcomes but suggest potential for earlier return to function with plates in select unstable patterns, though with higher rates of hardware-related complications.
- Biomechanical studies (e.g., by Huch et al., 2011) often show superior stability with plate fixation compared to K-wires, especially for rotational and bending loads, justifying their use in complex fractures.
- Interfragmentary Screws: Highly effective for long oblique or spiral fractures, providing excellent compression and rigid fixation with minimal soft tissue disruption, as highlighted in various hand surgery texts.
- Articular Fractures: Management guidelines emphasize anatomical reduction of articular step-off (>1mm is generally unacceptable) to prevent post-traumatic arthrosis. Both K-wires and small screws (cannulated or non-cannulated) are utilized, often with direct visualization.
- Complication Management: The literature consistently points to stiffness as the most common and debilitating complication. Aggressive, individualized hand therapy is universally advocated. Early referral to a certified hand therapist significantly improves outcomes. Revision surgery for malunion or nonunion, while less frequent, can be complex and requires careful planning.
- Controversies: The debate between the optimal fixation method (K-wires vs. plates), particularly for mid-shaft fractures, continues. Factors such as fracture morphology, soft tissue envelope, surgeon experience, and patient functional demands often dictate the final choice. The trend leans towards more stable fixation for more complex injuries to facilitate early mobilization, recognizing the trade-off with potential hardware-related issues.
In conclusion, the best treatment for a proximal phalanx fracture is a tailored approach, integrating a thorough understanding of the unique anatomy, biomechanics, fracture characteristics, and patient-specific factors, always with an eye toward preserving motion and minimizing long-term disability.
Clinical & Radiographic Imaging