Proximal Hamstring Injuries: br j sports Insights for Faster Recovery

Key Takeaway
We review everything you need to understand about Proximal Hamstring Injuries: br j sports Insights for Faster Recovery. Proximal hamstring injuries in athletes range from musculotendinous junction strain to partial tears or complete avulsion from the ischial tuberosity. These stretch-induced injuries typically occur during eccentric activation in high-speed sports, a topic covered in sources such as *br j sports*. Severity dictates recovery, with avulsions causing significant disability and often requiring surgical intervention.
Introduction and Epidemiology
Stretch-induced proximal hamstring injury represents a frequent and clinically significant pathology among the athletic population. These injuries exist along a definitive continuum, ranging from mild strains at the musculotendinous junction to partial tears of the tendon, and ultimately to complete avulsions of the hamstring muscle complex from the ischial tuberosity. The natural history of these injuries varies considerably based on the anatomical location and the severity of the structural failure. A more proximal injury, particularly an avulsion, typically results in a substantially longer recovery trajectory to pre-injury status and carries a significantly greater likelihood of requiring surgical intervention due to the persistent and profound disability associated with loss of the ischial anchor.
Epidemiological data indicate that proximal hamstring injuries are particularly prevalent in sports requiring high-speed sprinting, rapid acceleration, and sudden changes in direction. Furthermore, the greatest recognized risk factor for injury to the hamstring muscle complex is a history of previous injury to the ipsilateral extremity. Literature reports recurrence rates for hamstring injuries ranging from 12% to 31%. This high rate of reinjury is frequently attributed to either insufficient rehabilitation, premature return to sport, or the persistence of pre-existing biomechanical risk factors. Consequently, the treating orthopedic surgeon must possess the clinical acumen to accurately assess the degree of injury, a comprehensive knowledge of the reparative processes of healing muscle and tendon, and a thorough understanding of the rehabilitative and preventive measures required to mitigate recurrence.
Pathogenesis and Mechanism of Injury
The principal mechanism of injury involves eccentric activation of the hamstring complex while under significant stretch. This biomechanical scenario is classically observed when the hip is dynamically flexed and the knee is simultaneously extended, such as when the hamstrings attempt to decelerate the advancing leg during the terminal swing phase of high-speed running.
An additional, though less common, mechanism for proximal hamstring avulsion involves an extreme stretch with an uncertain or variable amount of active muscle contraction. This mechanism is frequently encountered in specific athletic scenarios, such as waterskiing, where the athlete is pulled forward forcefully with an extended knee and sudden, extreme hip flexion. The resultant force vector exceeds the ultimate tensile strength of the tendon-bone interface at the ischial tuberosity, leading to catastrophic failure.
Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy of the posterior thigh and gluteal region is paramount for the safe and effective operative management of proximal hamstring avulsions. The hamstring muscle group is composed of three distinct muscles: the biceps femoris (comprising long and short heads), the semitendinosus, and the semimembranosus. With the exception of the short head of the biceps femoris, which originates from the linea aspera of the posterior femur, all hamstring muscles originate from the ischial tuberosity of the pelvis.
Osteology and Musculotendinous Origins
The ischial tuberosity serves as the critical osseous anchor for the proximal hamstring complex. The footprint is anatomically divided into distinct facets. The biceps femoris long head and the semitendinosus share a common tendinous origin (the conjoined tendon) that attaches to the posteromedial facet of the ischial tuberosity. In contrast, the semimembranosus has a distinct, broad, and flat origin that attaches to the anterolateral facet, deep and slightly lateral to the conjoined tendon.
The hamstrings function as biarticular muscles, bridging both the hip and knee joints. This dual-joint architecture renders them highly susceptible to stretch-induced injuries during complex, multi-planar movements. Anatomical studies have demonstrated that the proximal tendons of the biceps femoris and semimembranosus extend distally for approximately 62% and 73%, respectively, of their total muscle belly lengths. This extensive musculotendinous architecture is clinically relevant, as strains most frequently occur in the biceps femoris, typically localized near the musculotendinous junction rather than the osseous origin.

Neurovascular Structures
The most critical neurovascular structure in the vicinity of the proximal hamstring origin is the sciatic nerve. The sciatic nerve exits the greater sciatic foramen deep to the piriformis muscle and descends through the posterior thigh. At the level of the ischial tuberosity, the sciatic nerve lies immediately lateral to the hamstring origin, typically separated by a distance of merely 1.0 to 1.5 centimeters.
During a complete avulsion, the normal anatomical tension of the hamstring complex is lost, and the retracted tendon stump can adhere to the adjacent sciatic nerve through intense inflammatory scarring. This perineural fibrosis can lead to significant sciatic neuropathy, presenting as radiating pain, paresthesias, or motor deficits in the distribution of the tibial and common peroneal nerves. Meticulous identification, neurolysis, and protection of the sciatic nerve are mandatory steps during any surgical exploration of the proximal hamstring.
Indications and Contraindications
The clinical presentation of a proximal hamstring injury typically involves the sudden onset of acute pain in the posterior proximal thigh during athletic competition or training. In cases of severe injury, such as a complete avulsion, physical examination may reveal a visible deformity in the posterior thigh, significant dependent swelling, extensive ecchymosis, and a palpable defect immediately distal to the ischial tuberosity. Focal tenderness to palpation over the ischium and pain provocation with resisted knee flexion are highly consistent findings.
Partial or complete hamstring avulsions must be carefully differentiated from isolated strains at the musculotendinous junction. While musculotendinous strains are generally managed successfully with non-operative rehabilitation protocols, avulsions can be profoundly disabling. Avulsions frequently cause persistent symptoms of weakness, deep gluteal pain, and a distinct loss of dynamic muscle control, particularly during fast-paced running or deceleration activities. Consequently, complete avulsions, and select partial avulsions, warrant strong consideration for surgical repair.
| Clinical Scenario | Operative Indications | Non Operative Indications |
|---|---|---|
| Complete Avulsion (3 Tendons) | Retraction > 2 cm, high-level athlete, acute injury (< 4 weeks) | Significant medical comorbidities, low-demand elderly patient |
| Partial Avulsion (1 to 2 Tendons) | Persistent pain and weakness after 3-6 months of conservative care | Acute partial tears with minimal retraction, intact semimembranosus |
| Musculotendinous Junction Strain | Rarely indicated; only for massive hematoma evacuation (exceptional) | Standard of care; rest, progressive loading, physical therapy |
| Chronic Avulsion (> 6 months) | Severe sciatic neuropathy, debilitating weakness, acceptable muscle quality | Severe fatty infiltration/atrophy on MRI, asymptomatic patient |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential to achieve optimal surgical outcomes and minimize the risk of intraoperative complications. The cornerstone of preoperative evaluation relies heavily on advanced diagnostic imaging to quantify the extent of the injury and map the altered local anatomy.
Diagnostic Imaging Modalities
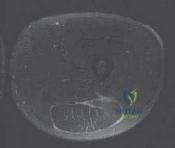
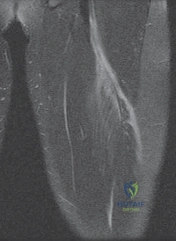
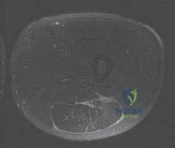
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating proximal hamstring injuries. Proper imaging protocols should include large field-of-view T1-weighted and fluid-sensitive (e.g., T2 fat-suppressed or STIR) sequences in the axial, coronal, and sagittal planes.
The MRI must be systematically evaluated for several critical parameters. First, the number of avulsed tendons (conjoined tendon vs. semimembranosus vs. all three) must be identified. Second, the degree of distal retraction of the free tendon stump must be measured, typically utilizing the coronal and sagittal sequences. Retraction greater than 2 centimeters is generally considered a strong indication for surgical intervention in the active patient. Third, the cross-sectional area of muscle involvement should be assessed, as recovery time correlates directly with the percentage of abnormal muscle signal. Injuries involving over 50% of the cross-sectional area portend a significantly protracted recovery period. Finally, the relationship of the retracted tendon to the sciatic nerve must be scrutinized to anticipate the necessity and complexity of intraoperative neurolysis.
Operating Room Setup and Patient Positioning
Surgical repair is performed with the patient under general anesthesia to ensure complete muscle relaxation, which is critical for mobilizing a retracted tendon. The patient is carefully transitioned to the prone position on a radiolucent operating table. Chest rolls or a specialized prone positioning frame should be utilized to ensure adequate pulmonary compliance and avoid abdominal compression.
The operative extremity is prepped and draped freely to allow for intraoperative manipulation. The knee is typically flexed to 90 degrees, and the hip is slightly extended. This specific positioning serves a dual purpose: it maximizes relaxation of the hamstring muscle-tendon unit, facilitating distal mobilization and reduction to the ischium, and it simultaneously relaxes the sciatic nerve, reducing the risk of iatrogenic traction injury during retraction. Fluoroscopy should be available to confirm the anatomical footprint of the ischial tuberosity if landmarks are obscured by chronic scarring.
Detailed Surgical Approach and Technique
The surgical technique for proximal hamstring repair demands meticulous dissection, respect for neurovascular planes, and robust biomechanical fixation. The approach must be tailored to the chronicity of the injury and the degree of tendon retraction.
Incision and Superficial Dissection
Two primary incision options exist: the transverse gluteal crease incision and the longitudinal posterior thigh incision.
The transverse incision is placed directly within the gluteal fold. It offers superior cosmetic results and is generally preferred for acute injuries with minimal tendon retraction (< 3 cm). However, it provides limited distal extensibility.
The longitudinal incision is centered over the palpable defect or the ischial tuberosity and extends distally along the posterior midline of the thigh. This approach is mandatory for chronic injuries or acute injuries with significant retraction (> 3-5 cm), as it allows for extensive distal dissection to mobilize the scarred tendon belly.
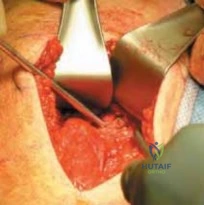
Following the skin incision, the subcutaneous tissue is sharply divided to expose the inferior border of the gluteus maximus fascia. The fascia is incised, and the inferior edge of the gluteus maximus muscle is mobilized and retracted superiorly. This maneuver exposes the deep subgluteal space, the ischial tuberosity, and the underlying proximal hamstring complex.
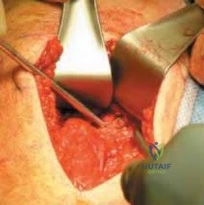
Sciatic Nerve Neurolysis
Identification and protection of the sciatic nerve represent the most critical phase of the dissection. The nerve is consistently found lateral to the ischial tuberosity, descending posterior to the quadratus femoris and adductor magnus muscles. In acute cases, a large hematoma is often present; this must be carefully evacuated to visualize the anatomical structures.
In chronic cases, the retracted hamstring tendon frequently forms dense fibrous adhesions to the sciatic nerve. Meticulous neurolysis must be performed using a combination of sharp and blunt dissection. The nerve should be traced from proximal (at the level of the piriformis, if necessary) to distal (beneath the retracted tendon stump). Once identified and freed from surrounding scar tissue, the sciatic nerve is gently isolated and protected with a vessel loop. Excessive traction on the nerve must be strictly avoided to prevent transient or permanent neuropraxia.
Tendon Mobilization and Ischial Preparation
Once the sciatic nerve is secured, attention is directed to the avulsed hamstring tendon. The tendon stump is identified, grasped with heavy traction sutures (e.g., Number 2 non-absorbable sutures) using a Krackow or similar locking configuration, and mobilized. In chronic cases, extensive release of fascial adhesions along the posterior thigh may be required to achieve adequate excursion. The knee is flexed to 90 degrees to assist with mobilizing the tendon toward the anatomical footprint.
The ischial tuberosity is then prepared to optimize the biology for tendon-to-bone healing. Soft tissue remnants and fibrous scar are excised from the anatomical footprint using a combination of electrocautery and rongeurs. The cortical surface of the ischial tuberosity is decorticated using a high-speed burr or a sharp curette until a bleeding, cancellous bone bed is exposed. This bleeding bed provides the necessary osteoprogenitor cells and vascularity to facilitate robust incorporation of the repaired tendon.
Anchor Placement and Tendon Fixation
Fixation is typically achieved utilizing multiple suture anchors. Depending on the size of the patient and the footprint, two to four metallic or radiolucent biocomposite suture anchors (typically 5.0 mm to 6.5 mm in diameter) are placed into the decorticated ischial tuberosity. The anchors are strategically positioned to recreate the native anatomical footprint, with careful attention to placing the anchors centrally within the robust bone of the tuberosity to prevent pullout.
The sutures from the anchors are then passed through the mobilized tendon stump. A variety of suture configurations can be utilized, but locked running stitches or modified Mason-Allen configurations provide superior biomechanical pullout strength. The sutures are systematically tied while an assistant maintains the knee in 90 degrees of flexion and the hip in neutral extension to eliminate tension on the repair. Following secure fixation, the repair is inspected, the wound is copiously irrigated, and a layered closure is performed. A subfascial closed-suction drain may be placed to prevent postoperative hematoma formation, particularly in cases with extensive dead space.
Complications and Management
Surgical repair of proximal hamstring avulsions is a highly successful procedure, but it carries a distinct risk profile. Thorough preoperative counseling regarding potential complications is mandatory.
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage Strategies and Management |
|---|---|---|---|
| Sciatic Neuropathy | 2% to 8% | Iatrogenic traction, entrapment in scar tissue, direct suture entrapment | Observation for neuropraxia, gabapentinoids, surgical exploration/neurolysis for refractory cases |
| Infection | 1% to 3% | Proximity to perianal region, hematoma formation, prolonged operative time | Intravenous antibiotics, aggressive surgical debridement, hardware retention if stable |
| Re Rupture | 2% to 5% | Non-compliance with rehabilitation, premature return to sport, poor tissue quality | Revision surgical repair, augmentation with allograft (e.g., Achilles tendon), conservative management |
| Deep Vein Thrombosis | < 2% | Prone positioning, postoperative immobilization, venous stasis | Chemical prophylaxis for high-risk patients, early mobilization, therapeutic anticoagulation if diagnosed |
| Heterotopic Ossification | 1% to 4% | Aggressive decortication, extensive muscle trauma, chronic injury | Prophylactic NSAIDs (indomethacin), physical therapy, delayed surgical excision if mechanically restrictive |
Management of complications requires a systematic approach. Sciatic nerve palsy is the most feared complication. If a patient awakens with a new, profound motor deficit (e.g., foot drop) that was not present preoperatively, immediate re-exploration may be warranted to rule out direct suture entrapment of the nerve. Conversely, delayed onset of radiating pain or paresthesias is often related to postoperative swelling or hematoma and can frequently be managed conservatively with neuropathic pain modulators and time.

Post Operative Rehabilitation Protocols
The success of a proximal hamstring repair is inextricably linked to a meticulously structured, phased postoperative rehabilitation protocol. The rehabilitative philosophy must balance the biomechanical necessity of protecting the healing tendon-to-bone interface with the physiological requirement to prevent debilitating joint contractures and muscle atrophy.
Early Protective Phase
Phase 1 encompasses the initial 0 to 6 weeks postoperatively. The primary objective during this phase is absolute protection of the surgical repair. Patients are typically placed in a hinged knee brace locked at 60 to 90 degrees of flexion to eliminate tension on the ischial footprint. Weight-bearing is strictly limited to toe-touch or non-weight-bearing using bilateral axillary crutches.
During the first two weeks, hip flexion is restricted to prevent passive stretching of the repair. Gentle, passive range of motion of the knee is initiated within safe, restricted arcs. Active hamstring contraction is strictly contraindicated. Modalities for pain and edema control, such as cryotherapy, are utilized extensively.
Intermediate and Advanced Rehabilitation
Phase 2 (Weeks 6 to 12) marks the transition to progressive loading and restoration of normal kinematics. The hinged knee brace is gradually unlocked, allowing progressive extension by 10 to 15 degrees per week until full extension is achieved. Weight-bearing is advanced incrementally to full weight-bearing as tolerated, with the goal of restoring a normalized, pain-free gait pattern. Active-assisted and active range of motion exercises are initiated, focusing on concentric hamstring activation within pain-free limits.
Phase 3 (Months 3 to 6) focuses on aggressive strengthening and the introduction of dynamic functional movements. Isotonic strengthening progresses to eccentric loading, which is critical for restoring the energy-absorbing capacity of the hamstring complex. Core stabilization, pelvic control, and closed-kinetic chain exercises are emphasized.
Phase 4 (6+ Months) is the return-to-sport phase. Progression to this phase requires full, symmetric range of motion, resolution of all pain, and isokinetic strength testing demonstrating at least 85% to 90% strength compared to the uninjured contralateral limb. Sport-specific drills, sprinting mechanics, and plyometric training are integrated. Return to unrestricted high-level competition typically occurs between 6 and 9 months postoperatively, depending on the chronicity of the initial injury and the specific demands of the sport.
Summary of Key Literature and Guidelines
Recent meta-analyses and systematic reviews published in prominent orthopedic and sports medicine journals, including insights from the British Journal of Sports Medicine (br j sports), have significantly refined our understanding of proximal hamstring injury management.
Conservative management remains the unequivocal standard of care for isolated musculotendinous junction strains. Rehabilitation paradigms emphasizing early, progressive eccentric loading (such as the Nordic hamstring exercise protocol) have demonstrated superior efficacy in accelerating recovery and reducing recurrence rates compared to traditional concentric strengthening programs.
However, for complete proximal hamstring avulsions, the literature strongly supports early surgical intervention. Studies comparing operative versus non-operative management of complete, retracted avulsions consistently demonstrate that surgical repair yields significantly higher rates of return to pre-injury levels of athletic participation, superior restoration of isokinetic hamstring strength, and higher patient-reported outcome scores. Furthermore, acute surgical repair (performed within 4 to 6 weeks of injury) is associated with lower complication rates, less requirement for extensive sciatic neurolysis, and technically easier anatomic reduction compared to chronic, delayed reconstructions.
In conclusion, the management of proximal hamstring injuries requires a nuanced, individualized approach. Accurate diagnostic imaging, precise surgical technique with meticulous attention to the sciatic nerve, and strict adherence to biologically sound rehabilitation protocols are the essential pillars for achieving optimal clinical outcomes and facilitating a faster, safer recovery for the athlete.
Clinical & Radiographic Imaging