Female Athlete Triad: Diagnosing Critical Sports Medicine Cases
Key Takeaway
Here are the crucial details you must know about Female Athlete Triad: Diagnosing Critical Sports Medicine Cases. ACL graft failure in younger individuals often relates to allograft use, inadequate fixation, or poor tunnel placement, frequently requiring revision. Staged revisions are indicated for wide or compromised tunnels. Graft impingement, causing limited extension, typically results from an anterior tibial tunnel. For female athletes, considering factors like the female athlete triad is crucial for comprehensive injury prevention and recovery.
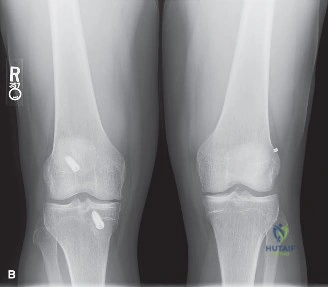
A 24-year-old competitive athlete presents with a suspected failed ACL reconstruction. He reports a "pop" and instability following a deceleration injury. Given his history of a primary allograft reconstruction 4 years ago, how would you approach the clinical assessment and what is your interpretation of these imaging findings?

Candidate: I would perform a thorough history and examination, specifically looking for rotatory instability using the pivot shift test. The radiographs suggest a failed previous reconstruction with tunnel widening and potential malposition. I would order a CT scan to quantify tunnel expansion and plan for either single or two-stage revision based on bone stock.
Failing to emphasize the pivot shift test as the gold standard for rotatory instability; simply mentioning "Lachman is positive" is insufficient. Candidates also often forget to mention the specific mechanism of tunnel widening (bungee/windshield wiper effect) and fail to mention that the choice of allograft was an initial surgical error.
Structure the response: 1. Clinical: Pivot shift is the key; assess concomitant injuries (meniscus/PLC) as these frequently contribute to early failure. 2. Radiographic Analysis: Recognize vertical, non-anatomic femoral tunnel placement (transtibial legacy) and quantify tunnel osteolysis. 3. Biological Context: Acknowledge allograft inferiority in young, active patients (MARS study data). 4. Decision Logic: State that if tunnel widening >14mm is confirmed on CT, a two-stage revision with bone grafting is mandatory to ensure reliable aperture fixation for the future autograft.
During your intraoperative assessment of the revision case, you identify that the knee lacks 5 degrees of terminal extension. What is your immediate clinical concern, and what is your intraoperative strategy to resolve this?
Candidate: I am concerned about roof impingement caused by an anteriorly placed tibial tunnel. I would check the positioning, potentially perform a notchplasty, or, if the tunnel is significantly too anterior, I would consider revising the tunnel position if bone stock allows.
Suggesting a "Cyclops lesion removal" without addressing the primary mechanical cause. If you don't fix the tunnel malposition or provide adequate clearance, the graft will fail again due to chronic attrition against the roof of the notch.
Define this as "Roof Impingement." Explain that the graft is intersecting Blumensaat's line during extension. Actionable Strategy: 1. Confirm position arthroscopically. 2. Perform a selective notchplasty to clear the roof. 3. If still restricted, re-evaluate the tibial tunnel aperture; if it's too anterior, you must re-drill or correct the trajectory. 4. Emphasize that full terminal extension MUST be achieved intraoperatively to prevent permanent post-operative arthrofibrosis.
