Lunate Fractures and Kienböck Disease: Comprehensive Surgical Management
Key Takeaway
Kienböck disease and lunate fractures present complex biomechanical challenges in hand surgery. This comprehensive guide details the vascular anatomy of the lunate, the Lichtman staging system for avascular necrosis, and evidence-based surgical interventions. From joint-leveling procedures like radial shortening osteotomy to metaphyseal core decompression and salvage operations, master the indications, operative techniques, and postoperative protocols required to restore carpal stability and alleviate radiocarpal degeneration.
FRACTURES OF THE LUNATE AND KIENBÖCK DISEASE
The lunate is the keystone of the proximal carpal row, playing a critical role in the complex biomechanics of the wrist. Pathologies affecting the lunate—ranging from acute traumatic fractures to the insidious progression of Kienböck disease (avascular necrosis of the lunate)—demand a profound understanding of carpal kinematics, vascular anatomy, and advanced surgical techniques.
Vascular Anatomy and Biomechanics of the Lunate
Trauma to the lunate may be sufficient to disrupt its tenuous intraosseous circulation, leading to osteonecrosis. Gelberman et al. meticulously described the extraosseous and intraosseous vascularity of the lunate, identifying three distinct patterns of vessels entering the bone.

The lunates believed to be at the highest risk for osteonecrosis are those with a single vessel or only one surface exposed to the blood supply. This high-risk vascular pattern represents approximately 20% of all lunates. When this fragile blood supply is compromised by trauma or repetitive microtrauma, the biomechanical compressive forces exerted by the capitate exacerbate ischemia, leading to structural collapse.
Clinical Pearl: Always consider the vascular watershed of the lunate. The lack of robust anastomoses in 20% of the population explains why seemingly innocuous wrist sprains can evolve into devastating Kienböck disease if an occult lunate fracture is missed.
ACUTE LUNATE FRACTURES
Diagnosis and Imaging
Fractures of the lunate are notoriously difficult to detect on standard posteroanterior (PA) and lateral plain radiographs due to the superimposition of the radial styloid, scaphoid, and triquetrum.
- Advanced Imaging: Thin-slice computed tomography (CT) or complex motion tomography is frequently required to definitively identify and characterize the fracture pattern.
- Fracture Patterns: Lunate fractures may present as nondisplaced, displaced with large fragments, avulsed (especially at the dorsal pole where critical radiocarpal ligaments attach), or highly comminuted.
Management of Lunate Fractures
Conservative Management:
Nondisplaced and nondisplaced comminuted fractures can be managed nonoperatively. Treatment consists of strict cast immobilization (typically a short-arm thumb-spica cast) for 6 to 8 weeks, followed by serial imaging to ensure no interval displacement or early signs of avascular necrosis.
Operative Management:
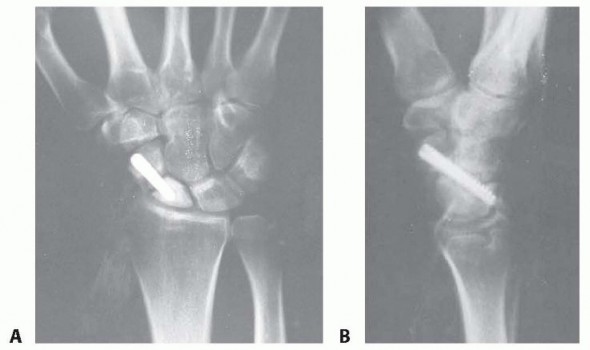
Fractures demonstrating more than 1 mm of articular step-off, gap, or significant avulsion fractures usually require open reduction and internal fixation (ORIF) to restore carpal kinematics and prevent radiocarpal arthrosis.
- Surgical Approach: A dorsal approach to the wrist (through the third extensor compartment) is most commonly utilized, allowing direct visualization of the proximal carpal row.
- Fixation Techniques: Depending on fragment size and comminution, fixation may be achieved using:
- 0.045-inch or 0.062-inch Kirschner wires (K-wires).
- Small headless cannulated compression screws (e.g., 1.5 mm or 2.0 mm).
- Suture anchors for dorsal pole avulsions involving the dorsal radiocarpal ligament.
KIENBÖCK DISEASE: PATHOPHYSIOLOGY AND DIAGNOSIS
Kienböck disease is a painful, progressive disorder of the wrist characterized by osteonecrosis of the carpal lunate. The exact etiology remains idiopathic, though it is widely considered multifactorial—combining the aforementioned vascular susceptibility with adverse biomechanical loading.
Demographics and Clinical Presentation
- Age and Gender: Most frequently observed in patients between 15 and 40 years of age.
- Occupation: Predominantly affects the dominant wrist of men engaged in heavy manual labor.
- Symptoms: Patients present with dorsal wrist pain, swelling, decreased grip strength, and restricted range of motion. Symptoms can precede radiographic evidence of the disease by up to 18 months.
The Role of Ulnar Variance (Hultén's Theory)
Hultén described a biomechanical condition known as the "ulna-minus variant" (negative ulnar variance). He found that in 78% of patients with Kienböck disease, the ulna was shorter than the radius at their distal articulation, compared to only 23% in normal wrists. Negative ulnar variance increases the shear and compressive forces transmitted directly from the radius to the lunate, accelerating fragmentation.
Imaging and Occult Fractures
Armistead et al., utilizing CT imaging, demonstrated that occult fractures of the lunate are present in a significant subset of Kienböck patients.

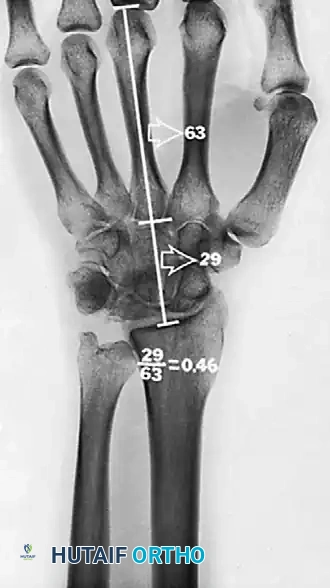
A common fracture pattern is the anterior pole type, which isolates the anterior pole from the remaining bone. The compressive force exerted by the capitate distracts the fracture, diminishing the likelihood of healing. As the dorsal portion of the lunate collapses, the anterior pole may be extruded volarly. Furthermore, the ratio of carpal height to the length of the third metacarpal is reduced (normal is 0.54 ± 0.03), indicating overall carpal collapse.
Magnetic Resonance Imaging (MRI) is the gold standard for diagnosing early avascular changes. Correlation of clinical findings with MRI helps differentiate Kienböck disease from ulnar impaction syndrome.
LICHTMAN CLASSIFICATION OF KIENBÖCK DISEASE
The staging classification proposed by Lichtman et al. is the universally accepted framework for guiding surgical decision-making. The natural history, if left untreated, progresses from sclerosis to fragmentation, carpal collapse, and ultimately pancarpal arthritis.





Stage I
- Description: No visible changes on plain radiographs. Diagnosis is made via MRI, which shows decreased signal intensity on T1-weighted images and increased signal on T2-weighted images (edema).
- Treatment: Immobilization and NSAIDs. If symptoms persist, treat as Stage II.
Stage II
- Description: Sclerosis of the lunate is visible on plain radiographs. The lunate retains its anatomic shape without collapse.
- Treatment:
- Ulnar-negative variance: Joint leveling procedure (radial shortening or ulnar lengthening).
- Ulnar-neutral variance: Radial wedge osteotomy or Scaphotrapeziotrapezoid (STT) fusion.
- Alternative: Distal radial core decompression to stimulate a local vascular healing response.



Stage IIIA
- Description: Fragmentation and collapse of the lunate occur, but carpal alignment is maintained. The scaphoid remains normally aligned.
- Treatment: Joint leveling procedures remain the gold standard if the radiocarpal joint is preserved. Revascularization procedures (pedicled bone grafts) are also utilized.
Stage IIIB
- Description: Lunate fragmentation is accompanied by fixed rotation of the scaphoid (dorsal intercalated segmental instability - DISI pattern) and proximal migration of the capitate.
- Treatment: Proximal row carpectomy (PRC) or STT fusion. The internal collapse pattern must be addressed.


Stage IV
- Description: Advanced degeneration. Secondary osteoarthritic changes extend to the adjacent intercarpal and radiocarpal joints.
- Treatment: Salvage procedures including wrist arthrodesis (total wrist fusion), proximal row carpectomy, or limited intercarpal fusions.
SURGICAL MANAGEMENT OF KIENBÖCK DISEASE
Because the natural course of Kienböck disease is unpredictable, treatment must be tailored to the Lichtman stage, ulnar variance, and patient demands.
1. Joint Leveling Procedures
Joint leveling procedures aim to unload the lunate by altering the radioulnar variance, thereby redistributing forces across the radiocarpal joint. These are primarily indicated for Lichtman Stage I through IIIA with an ulnar-minus variance.
Ulnar Lengthening:
Historically described by Persson (1945) and later popularized by Armistead et al., ulnar lengthening involves an osteotomy of the distal ulna, distraction, and interposition of an iliac crest bone graft.

While effective (Armistead reported pain relief in 18 of 20 patients), ulnar lengthening carries a higher risk of nonunion and requires structural bone grafting.
Radial Shortening Osteotomy (RSO):
To minimize the chance of nonunion and avoid iliac crest harvest, radial shortening is currently the preferred joint leveling procedure for most hand surgeons.
* Surgical Technique:
1. A volar Henry approach is utilized to expose the distal radius.
2. The pronator quadratus is elevated from its radial border.
3. A transverse or oblique osteotomy is performed approximately 3 inches (7.6 cm) proximal to the distal articular surface.
4. Exactly 2 mm of bone is resected using parallel saw blades.
5. The osteotomy is reduced and rigidly fixed with a volar compression plate (typically a 3.5 mm dynamic compression plate).
* Biomechanics: Shortening the radius by just 2 mm significantly unloads the radiolunate fossa and shifts the load to the ulnocarpal articulation.
Surgical Warning: Over-shortening the radius (>2.5 mm) can lead to severe ulnocarpal impaction syndrome and distal radioulnar joint (DRUJ) incongruity. Precise preoperative templating is mandatory.
2. Osteotomies of the Distal Radius
For patients with Stage II or III Kienböck disease who possess an ulnar-neutral wrist, joint leveling is contraindicated. Instead, a radial closing wedge osteotomy is proposed.
* Rationale: By decreasing the radial inclination, pressure is shifted away from the lunate.
* Biomechanical Evidence: Biomechanical analyses demonstrate that a radial closing wedge osteotomy decreases force on the lunocapitate joint by 23%, the radiolunate joint by 10%, and the ulnolunate joint by 36%. However, debate exists, as other studies suggest lateral opening wedge osteotomies may be superior for unloading the lunate fossa.
3. Metaphyseal Core Decompression
Introduced by Illarramendi et al. in 2001, metaphyseal core decompression of the radius and ulna is a less invasive alternative that avoids altering carpal mechanics.
- Rationale: The procedure was developed after observing spontaneous resolution of Kienböck disease following a nondisplaced distal radius fracture. The mechanism is believed to be a regional acceleratory phenomenon (RAP)—the surgical trauma stimulates a robust local vascular healing response that revascularizes the lunate.
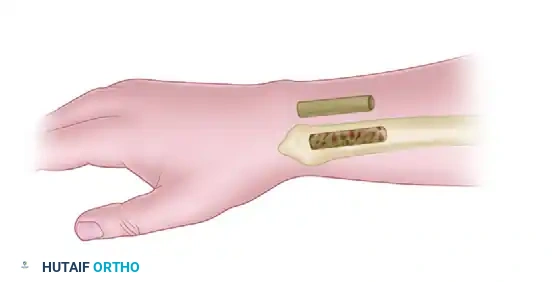
- Surgical Technique:
- A small incision is made over the distal radial metaphysis.
- A cortical window is created.
- Extensive curettage of the cancellous bone in the distal radius is performed.
- The cortical window is replaced, and the wound is closed without internal fixation.

- Outcomes: Illarramendi reported satisfactory results in 90% of patients. Later studies by Mehrpour et al. applied core decompression directly to the lunate to decrease intraosseous pressure (similar to femoral head decompression), yielding good results in 18 of 20 patients. Bain et al. have also described arthroscopic-assisted lunate core decompression.
4. Revascularization Procedures
For early-stage disease without collapse, vascularized bone grafting (VBG) can restore blood supply.
* Techniques: The 4+5 Extensor Compartmental Artery (ECA) pedicled graft from the distal radius, or a free vascularized medial femoral condyle graft.
* Adjuncts: Revascularization must be protected from compressive forces. This is achieved by temporary pinning of the scaphocapitate joint or application of a spanning external fixator for 8 to 12 weeks.
5. Salvage Procedures (Stage IIIB and IV)
When the lunate has collapsed, the scaphoid has rotated (DISI), or secondary arthritis has set in, joint leveling and revascularization are no longer viable.
- Proximal Row Carpectomy (PRC): Excision of the scaphoid, lunate, and triquetrum. Converts the wrist to a simple hinge joint between the capitate and the lunate fossa of the radius. Requires a pristine capitate head.
- Scaphoid-Trapezium-Trapezoid (STT) Fusion: Halts the DISI collapse pattern and unloads the lunate by transferring forces through the scaphoid.
- Total Wrist Arthrodesis: The ultimate salvage for Stage IV pancarpal arthritis. Provides reliable pain relief at the expense of all radiocarpal and midcarpal motion.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative regimen is dictated by the specific surgical intervention performed:
- Joint Leveling (Radial Shortening): Patients are placed in a short-arm cast or rigid splint for 2 to 4 weeks. Once radiographic evidence of osteotomy consolidation is noted, active and active-assisted range of motion (ROM) exercises commence. Heavy lifting is restricted until complete union (typically 8-12 weeks).
- Core Decompression: Because no structural alteration or fixation is performed, patients can begin early gentle ROM within 1 to 2 weeks postoperatively, progressing to strengthening as pain allows.
- Salvage Procedures (PRC / Fusions): Immobilization in a cast for 4 to 6 weeks is standard. For fusions, CT confirmation of bridging trabecular bone is recommended before initiating aggressive strengthening.
By meticulously matching the surgical intervention to the patient's anatomic variance and Lichtman stage, the orthopedic surgeon can effectively halt the progression of Kienböck disease, relieve debilitating pain, and preserve functional wrist kinematics.
You Might Also Like