Principles of Hand Fracture and Dislocation Management
Key Takeaway
The management of hand fractures and dislocations requires a delicate balance between anatomical reduction and functional preservation. While radiographic perfection is desirable, it must not supersede the ultimate goal of restoring hand mechanics. This guide details the foundational principles of treating hand injuries, emphasizing the critical evaluation of malrotation, appropriate radiographic imaging, and the judicious application of closed versus operative interventions to optimize patient outcomes.
Introduction to Hand Trauma and Functional Preservation
Although the general principles of orthopedic trauma management remain consistent across all regions of the musculoskeletal system, the hand represents a highly specialized, prehensile structure that interacts intimately with the environment. Consequently, it is exquisitely sensitive to functional impairment. The intricate balance of the intrinsic and extrinsic musculature, combined with the tight tolerances of the flexor and extensor gliding mechanisms, dictates that even minor architectural disruptions can lead to profound disability.
In the treatment of hand fractures and dislocations, a critical paradigm must be understood by all orthopedic surgeons: anatomical and radiographic perfection does not always equate to normal function. The pursuit of a pristine radiographic appearance through extensive surgical dissection often results in severe soft tissue scarring, tendon adhesions, and irreversible joint contractures. Often, it is far superior to accept a less-than-anatomical position of a fracture—provided it falls within acceptable biomechanical tolerances—and strive for excellent functional recovery through proper splinting and early, aggressive mobilization.
Clinical Pearl: The ultimate goal of hand fracture management is the restoration of the hand as a functional unit. When operative intervention is required, the surgeon must select the least complicated procedure that provides sufficient stability to allow for early active motion.
With very few exceptions, prolonged immobilization (greater than 3 weeks) is strictly contraindicated in the management of hand injuries. Prolonged casting leads to collateral ligament contracture, particularly at the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints, resulting in debilitating stiffness. Because clinical union of hand fractures frequently precedes radiographic evidence of consolidation by many weeks, early motion protocols should be initiated as soon as clinical stability is ensured.
The Pathoanatomy and Clinical Evaluation of Malrotation
When evaluating a reduced hand fracture, angulation and lack of apposition are readily apparent on standard orthogonal radiographs. However, rotational deformities are notoriously elusive on two-dimensional imaging due to the cylindrical nature of the phalangeal and metacarpal shafts. An error in rotation may only become devastatingly obvious after the fracture has clinically healed and the patient attempts to form a composite fist.
A rotational deformity of merely 5 degrees at the metacarpal base can translate to a 1.5 cm overlap at the fingertip, severely impairing grip strength and fine motor dexterity.
The Composite Fist Assessment
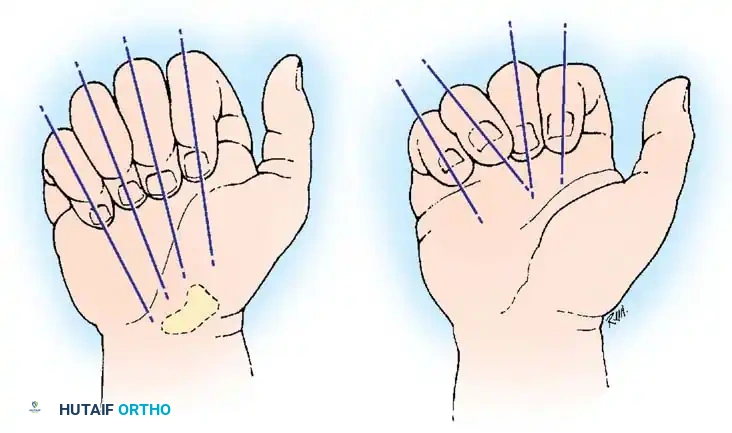
To accurately assess rotation, the surgeon must observe the kinematic alignment of the digits during active or passive flexion. Normally, when a composite fist is made, the longitudinal axes of all four fingers converge and point toward a single anatomical landmark: the scaphoid tubercle.
During the clinical evaluation of a fracture reduction, passively flexing all fingers fully at the MCP, PIP, and distal interphalangeal (DIP) joints simultaneously helps verify appropriate fracture rotation. If a fracture is malrotated, the affected finger will deviate from this convergence pathway, overriding or scissoring across an adjacent digit.
The Fingernail Plane Technique
Another highly reliable method for detecting subtle malrotation is the observation of the fingernail planes. With the fingers in partial flexion, the planes of the fingernails should align harmoniously, creating a smooth, uninterrupted arc.
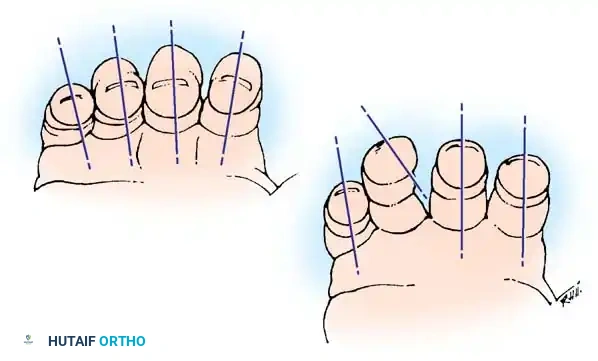
Comparing the injured hand to the contralateral, uninjured hand is essential. Any deviation in the plane of the nail bed relative to the adjacent digits strongly suggests a rotational malalignment at the fracture site that must be corrected prior to definitive fixation or casting.
Kinematics of the Fifth Ray
A common clinical pitfall involves the assessment of the little finger. The fifth digit possesses a natural tendency to overlap the ring finger during partial flexion. This phenomenon is permitted by the unique, highly mobile articulation of the fifth carpometacarpal (CMC) joint, which allows for 20 to 30 degrees of flexion and a significant degree of internal rotation (opposition) to facilitate cupping of the palm.
When a fracture limits the full flexion of the little finger, this partial-flexion overlap can be highly concerning to both the patient and the inexperienced physician. However, it must be understood that once full flexion of the little finger is achieved, it will align normally with the ring finger.
Surgical Warning: When full flexion of the little finger is accomplished, external rotation becomes biomechanically impossible due to the tightening of the collateral ligaments, whereas further internal rotation remains possible. Therefore, apparent internal malrotation at the fracture site during partial flexion may be a physiological illusion rather than a true deformity.
Radiographic Evaluation Protocols
Exact anteroposterior (AP) and lateral radiographs are the cornerstone of determining fragment position before and after reduction. However, standard views are often insufficient for complex hand trauma.
Optimizing the Lateral View
Obtaining a true lateral view of individual digits without superimposition is challenging.
* Splay Lateral (Fan Lateral): Views of the digits in varying degrees of flexion can help prevent phalangeal override, though they may only provide a true lateral projection for a single digit.
* Ring and Small Metacarpals: True lateral views of the 4th and 5th metacarpals can be reliably obtained by positioning the hand in 10 degrees of supination, while the index and middle fingers are held in 10 degrees of pronation.
Advanced Imaging Techniques
- Oblique Views: Essential for assessing the reduction of intra-articular fractures, particularly at the metacarpal heads and the bases of the phalanges.
- Fluoroscopy: Even when a fracture is being reduced under direct surgical vision, intraoperative fluoroscopy is mandatory. It prevents subtle errors in alignment and reveals small, interposed osteochondral fragments that may block anatomical reduction.
- Computed Tomography (CT): Sagittal and coronal CT reconstructions are increasingly necessary to evaluate articular step-offs, comminution patterns, and displacement, especially when a splint or cast obscures plain radiographic detail.
Indications for Operative Intervention
While a closed approach is generally preferred, specific indications necessitate operative osteosynthesis to restore the structural integrity of the hand:
- Open Fractures: Requiring immediate irrigation, debridement, and stabilization.
- Irreducible Fractures or Dislocations: Often due to soft tissue interposition (e.g., volar plate interposition in complex MCP dislocations).
- Unstable Fracture Patterns: Spiral or long oblique fractures of the metacarpals or phalanges that inherently shorten and malrotate under the pull of the intrinsic muscles.
- Intra-articular Fractures: Any articular step-off greater than 1 to 2 mm, or fractures involving more than 25% of the articular surface, generally require open reduction and internal fixation (ORIF) to prevent post-traumatic osteoarthritis.
- Multiple Ray Involvement: "Crushed hand" injuries require rigid fixation of the skeletal architecture to allow for the management of complex soft tissue, vascular, and nerve injuries.
Closed Management and Splinting Techniques
When closed reduction is deemed appropriate, the method of immobilization must prioritize the prevention of malrotation and the preservation of joint mobility.
Buddy Taping (Dynamic Syndactyly)
For rotationally unstable fractures managed closed, taping the injured finger to an adjacent, uninjured finger (buddy taping) is a highly effective technique. The uninjured digit acts as a dynamic splint, guiding the injured finger through a normal kinematic arc and preventing rotational deviation.
Clinical Pearl: When utilizing buddy tape as a derotation device, it is often preferable not to place gauze or cast padding between the fingers. Direct skin-to-skin contact, secured firmly with tape, provides superior rotational control. However, the skin must be monitored closely for maceration.
The Intrinsic Plus Position
When static splinting is required, the hand must be immobilized in the "safe position" (James position or intrinsic-plus position) to prevent collateral ligament contracture:
* Wrist: 20 to 30 degrees of extension.
* MCP Joints: 70 to 90 degrees of flexion (places the cam-shaped MCP collateral ligaments under maximal tension, preventing shortening).
* PIP and DIP Joints: Full extension (places the volar plate under tension, preventing flexion contractures).
Surgical Approaches and Biomechanics
When operative intervention is indicated, the surgical approach must respect the delicate soft tissue envelope of the hand.
Metacarpal Fractures
The biomechanics of metacarpal shaft fractures are dictated by the volar interossei, which pull the distal fragment proximally and volarly, resulting in apex-dorsal angulation.
* Approach: A dorsal longitudinal incision is typically utilized. For adjacent metacarpal fractures (e.g., 3rd and 4th), a single incision placed between the metacarpals can access both rays.
* Technique: The extensor tendon is retracted (usually ulnarly). The dorsal periosteum is incised and elevated minimally to preserve blood supply. Fixation can be achieved via lag screws (for long oblique fractures), dorsal plating, or intramedullary Kirschner wires.
Phalangeal Fractures
Proximal phalanx fractures typically present with apex-volar angulation due to the pull of the central slip on the distal fragment and the interossei on the proximal fragment.
* Approach: A mid-axial approach or a dorsal approach (splitting or retracting the extensor mechanism) can be used. The mid-axial approach is often preferred for shaft fractures as it avoids scarring the extensor tendon directly to the bone.
* Technique: Care must be taken not to strip the flexor sheath volarly. Low-profile plates or crossed K-wires are utilized. The hardware must be meticulously placed to avoid impinging on the lateral bands or the central slip.
Postoperative Protocols and Rehabilitation
The success of hand fracture management is ultimately determined in the postoperative rehabilitation phase.
The Concept of Clinical Union
Surgeons must differentiate between clinical union and radiographic union. Clinical union is defined as the absence of pain at the fracture site upon palpation and the absence of motion at the fracture site under gentle stress. In the hand, clinical union typically occurs at 3 to 4 weeks, whereas radiographic consolidation (bridging callus) may not be visible for 6 to 8 weeks.
Early Active Motion
Prolonged immobilization is the enemy of hand function. Once rigid internal fixation is achieved, or once a closed fracture demonstrates clinical stability, early active range of motion (AROM) must be initiated.
* Phase 1 (0-3 weeks): Edema control, wound care, and protected active motion in a custom thermoplastic splint.
* Phase 2 (3-6 weeks): Weaning of the splint, initiation of passive range of motion (PROM), and gentle strengthening.
* Phase 3 (>6 weeks): Aggressive strengthening and return to full functional activities.
By adhering to these strict biomechanical principles, respecting the soft tissue envelope, and prioritizing functional movement over radiographic perfection, the orthopedic surgeon can consistently achieve excellent outcomes in the management of complex hand fractures and dislocations.
You Might Also Like

