INTRODUCTION TO PROXIMAL TIBIAL FRACTURE-DISLOCATIONS
Proximal tibial fracture-dislocations represent a highly complex subset of knee trauma that must be strictly differentiated from standard tibial plateau fractures (such as those described by the Schatzker classification). While standard plateau fractures primarily involve axial loading and articular depression, fracture-dislocations involve a combination of axial load, severe translational forces, and rotational shear. This biomechanical cascade results in profound instability, mirroring the pathology of a true knee dislocation.
The hallmark of these injuries is the catastrophic failure of both the osseous architecture and the soft-tissue envelope. The fracture-dislocation patterns classified by Hohl and Moore occur with a significantly higher incidence of associated ligamentous injuries, frequent meniscal injuries (which are often severely macerated and usually cannot be repaired), and a dramatically higher incidence of neurovascular compromise.
Clinical Pearl: The overall average incidence of neurovascular injury in Hohl and Moore fracture-dislocations is approximately 15%—a rate nearly identical to that of classic knee dislocations. This incidence scales with the severity of the fracture pattern, increasing from 2% in Type I injuries to a staggering 50% in Type V injuries. A high index of suspicion and mandatory vascular assessment (ABI, CT Angiography) are non-negotiable.
THE HOHL AND MOORE CLASSIFICATION SYSTEM
The Hohl and Moore classification system divides proximal tibial fracture-dislocations into five distinct morphological types. Understanding these patterns is critical for preoperative planning, anticipating soft-tissue injuries, and determining the optimal surgical approach.
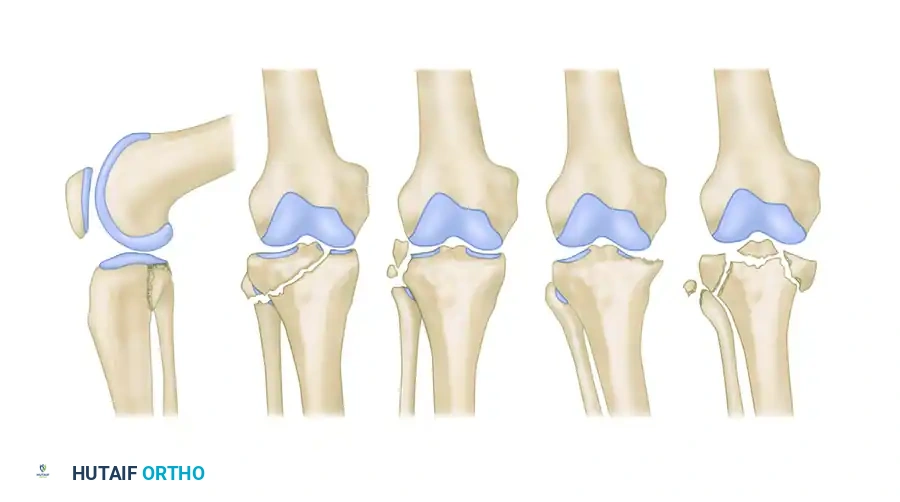
Type I: Coronal Split Fracture
Accounting for approximately 37% of all tibial plateau fracture-dislocations, the Type I pattern is characterized by a coronal split.
* Pathoanatomy: The fracture primarily involves the medial side and is most apparent on the lateral radiographic view. The fracture line runs at a 45-degree angle to the medial plateau in an oblique coronal-transverse plane.
* Associated Injuries: The fracture may extend to the lateral side. Avulsion fractures are highly common, frequently involving the fibular styloid, the insertion of the cruciate ligaments, and Gerdy’s tubercle.
* Stability & Management: Approximately half of these fracture-dislocations are stable on stress views. While they conceivably could be managed non-operatively in a cast in extension or via traction with a limited range of motion, modern orthopedic principles favor surgical intervention. Closed reduction and percutaneous screw fixation are frequently utilized to improve articular congruity, restore stability, and allow for early range of motion in a hinged cast brace. Protected weight-bearing is strictly continued for 8 to 10 weeks. If open reduction is required, the fragment usually reduces in extension and can be rigidly fixed with interfragmentary lag screws. Associated ligamentous injuries and invariable capsular disruptions should be repaired concurrently.
Type II: Entire Condyle Fracture
Constituting 25% of all fracture-dislocations, the Type II injury involves the shearing of an entire condyle.
* Pathoanatomy: This fracture may involve either the medial or lateral plateau. It is distinguished from standard plateau fractures and Type IV injuries by a fracture line that extends into the opposite compartment, passing directly beneath the intercondylar eminence.
* Associated Injuries: The opposite collateral ligament complex is involved in 50% of these fractures, frequently resulting in an associated fracture or dislocation of the proximal fibula. Neurovascular injuries occur in 12% of cases.
* Stability & Management: Stress testing under anesthesia is often necessary to determine the presence of occult ligamentous injury. Stable fractures can be managed by cast bracing, frequent radiographic follow-up, and delayed weight-bearing. However, unstable or poorly reduced fractures mandate surgical stabilization. Fixation is typically achieved with interfragmentary screws and buttress plating following closed or open reduction. Any associated ligamentous injury must be repaired.

Type III: Rim Avulsion Fracture
Type III injuries account for 16% of fracture-dislocations and are characterized by high-energy avulsions.
* Pathoanatomy: This type involves almost exclusively the lateral plateau. It presents as avulsion fragments of the capsular attachment, Gerdy’s tubercle, or the peripheral articular rim.
* Associated Injuries: Disruption of either or both cruciate ligaments is highly common. While meniscal injury is relatively rare in this specific subtype, neurovascular injuries occur in an alarming 30% of cases.
* Stability & Management: Nearly all Type III fractures are grossly unstable. Surgical intervention is required. A lateral surgical approach allows for direct visualization and screw fixation of the articular rim, alongside the repair of the avulsed iliotibial band and collateral ligaments. Cruciate ligament repair or augmentation is frequently necessary to restore knee kinematics.
Type IV: Rim Compression Fracture
Accounting for 12% of all fracture-dislocations, the Type IV pattern is driven by severe subluxation and impaction.
* Pathoanatomy: The tibia subluxates to such an extent that the femoral condyle violently compresses a portion of the anterior, posterior, or "middle" articular rim of the tibia.
* Associated Injuries: This injury is almost always unstable. The opposite collateral ligament complex is routinely torn, and the cruciate ligaments are avulsed or ruptured in 75% of patients.
* Stability & Management: While theoretically stable injuries can be treated by casting until the ligaments heal, this is exceedingly rare. Surgery is almost universally necessary. A parapatellar approach allows for meticulous débridement of small, non-viable osteochondral fragments, elevation and stabilization of larger articular fragments, and comprehensive repair of the cruciate and opposite collateral ligaments. Postoperative mobilization is largely dictated by the nature and security of the ligamentous repair.
Type V: Four-Part Fracture
The most devastating of the classifications, the Type V injury constitutes 10% of all fracture-dislocations.
* Pathoanatomy: This is a true bicondylar fracture-dislocation where both tibial plateaus are split off, and the intercondylar eminence is a separate, free-floating fragment. The distinguishing feature is the complete dissociation of the articular surface from the metaphysis and diaphysis.
* Associated Injuries: This injury is nearly always unstable. Neurovascular injury occurs in 50% of these fractures, with the popliteal artery and the peroneal nerve being injured in more than one-third of cases. Both collateral ligament complexes are disrupted, and the stabilization provided by the cruciates is entirely lost due to the eminence fracture.
* Stability & Management: Management of Type V injuries is fraught with complications. Historically, a bicondylar approach with dual plating was recommended; however, modern surgeons are far more cautious.
Surgical Warning: In a landmark review of tibial plateau fractures, Moore, Patzakis, and Harvey analyzed 296 bicondylar fractures. Of the 95 treated by Open Reduction and Internal Fixation (ORIF), 11 required medial and lateral plating. Shockingly, 9 of those 11 fractures (82%) treated with dual plating underwent wound dehiscence or became deeply infected. The overall infection rate for Type V bicondylar fractures was 23%.
Due to this unacceptably high complication rate, it is best to avoid stabilizing both condyles with large, bulky implants through extensile exposures. Contemporary management favors plating the more displaced and comminuted condyle with a buttress plate, while the less involved condyle is reduced via ligamentotaxis or percutaneous techniques and stabilized with large cancellous lag screws. Alternatively, limited open reduction and percutaneous fixation combined with a neutral external fixator (in a delta configuration) or an Ilizarov fine-wire frame is highly recommended to spare the compromised soft tissue envelope.
PREOPERATIVE EVALUATION AND DIAGNOSTICS
Advanced Trauma Life Support (ATLS)
Patients presenting with Hohl and Moore fracture-dislocations have often sustained high-energy trauma (e.g., motor vehicle collisions, falls from height). A full ATLS primary and secondary survey is mandatory to rule out life-threatening concomitant injuries.
Vascular Assessment
Given the 15% to 50% risk of neurovascular compromise, vascular assessment is the most critical step in the initial evaluation.
* Physical Examination: Assess palpable pulses (dorsalis pedis, posterior tibial). Note that the presence of pulses does not definitively rule out an intimal tear of the popliteal artery.
* Ankle-Brachial Index (ABI): An ABI of less than 0.9 is highly suspicious for arterial injury and warrants immediate advanced imaging.
* CT Angiography (CTA): CTA is the gold standard for evaluating the popliteal artery in the setting of a knee fracture-dislocation. If an arterial injury is identified, emergent vascular surgery consultation is required. Ischemia time exceeding 6-8 hours results in irreversible muscle necrosis and a high amputation rate.
Radiographic Imaging
- Plain Radiographs: AP, lateral, and oblique views of the knee. Stress views may be performed under anesthesia to unmask occult instability, particularly in Type I and Type II patterns.
- Computed Tomography (CT): A non-contrast CT scan with 2D and 3D reconstructions is mandatory for all complex plateau fractures. It defines the exact fracture morphology, the degree of articular depression, and the location of the primary fracture lines, which dictates the surgical approach.
- Magnetic Resonance Imaging (MRI): While not always feasible in the acute trauma setting, MRI is invaluable for assessing the integrity of the cruciate ligaments, collateral ligaments, and menisci once the bone has been stabilized.
SURGICAL APPROACHES AND TECHNIQUES
Damage Control Orthopedics (DCO)
In the presence of severe soft tissue swelling, fracture blisters, or polytrauma, definitive ORIF must be delayed. The application of a spanning knee external fixator (placing pins in the anterior femur and the tibial shaft) restores length, alignment, and rotation while allowing the soft tissue envelope to recover. Definitive fixation is typically delayed for 10 to 21 days until the "wrinkle sign" appears.
Patient Positioning
For definitive fixation, the patient is placed supine on a radiolucent Jackson or OSI table. A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position. A sterile tourniquet is applied to the proximal thigh. The limb must be draped free to allow for full flexion and extension, which aids in reduction and fluoroscopic imaging.
The Anterolateral Approach
Used primarily for Type III (Rim Avulsion) and the lateral components of Type II and Type V fractures.
1. Incision: A curvilinear incision is made centered over Gerdy's tubercle, extending proximally toward the lateral epicondyle and distally along the anterior tibial crest.
2. Deep Dissection: The iliotibial (IT) band is incised in line with its fibers. The origin of the extensor digitorum longus and the tibialis anterior is elevated off the lateral tibial metaphysis.
3. Arthrotomy: A submeniscal arthrotomy is performed. The lateral meniscus is elevated superiorly with stay sutures to directly visualize the articular surface.
4. Reduction: Depressed articular fragments are elevated "en masse" using a bone tamp from a cortical window created distally in the metaphysis. The resulting metaphyseal void is filled with autograft, allograft, or bone substitute.
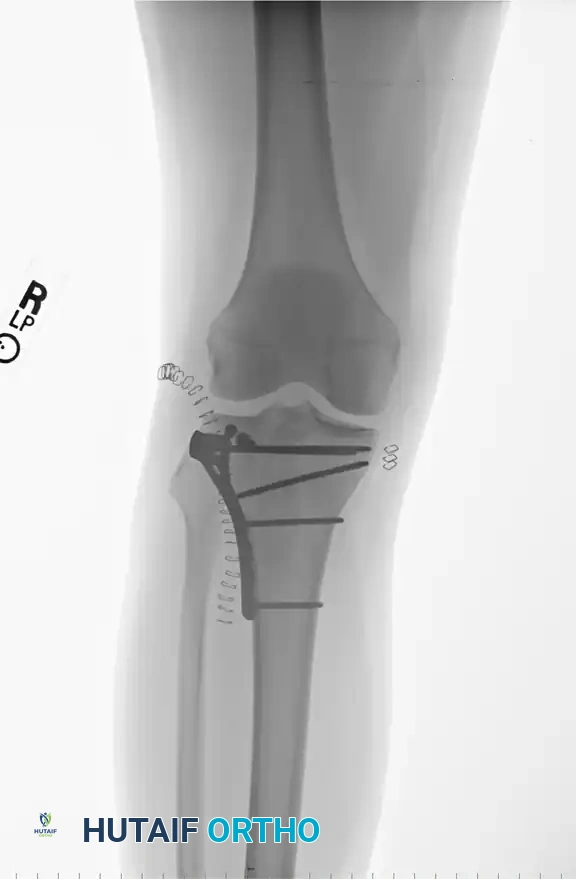
5. Fixation: The lateral cortex is supported with a pre-contoured lateral periarticular locking plate acting as a buttress.
The Posteromedial Approach
Utilized for medial coronal splits (Type I) and the medial component of bicondylar injuries.
1. Incision: A longitudinal incision is made along the posteromedial border of the tibia.
2. Deep Dissection: The saphenous nerve and vein are protected. The pes anserinus tendons are retracted anteriorly, and the medial head of the gastrocnemius is retracted posteriorly.
3. Fixation: This approach allows direct access to the posteromedial apex of the fracture. An anti-glide or buttress plate is applied to resist the sheer forces of the medial femoral condyle.
Management of the Soft Tissue Envelope in Type V Fractures
As highlighted by the Moore, Patzakis, and Harvey data, the soft tissue envelope in Type V four-part fractures is profoundly compromised.
* Avoid Dual Incisions: Simultaneous anterolateral and posteromedial incisions require massive soft tissue stripping, leading to the 82% complication rate noted historically.
* Hybrid Fixation: The modern gold standard for these severe injuries is a hybrid approach. A method of lateral plateau plating combined with temporary medial external fixation (as described by Mast) is highly effective. Alternatively, limited open reduction of the articular surface with percutaneous screw fixation, followed by the application of an Ilizarov fine-wire circular frame, provides excellent biomechanical stability while completely respecting the biology of the traumatized soft tissues.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Postoperative mobilization is a delicate balance between preventing joint stiffness and protecting the fracture fixation and ligamentous repairs.
- Phase I (0-6 Weeks):
- Motion is strictly prohibited until the surgical incisions have completely healed to prevent wound dehiscence.
- Once the soft tissue allows, passive and active-assisted range of motion (ROM) is initiated in a hinged knee brace.
- Weight-bearing is strictly non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) for plate and screw constructs.
- Exception: If an Ilizarov external fixator is utilized, early weight-bearing to tolerance is encouraged, as the frame relies on axial loading for micromotion and secondary bone healing.
- Phase II (6-12 Weeks):
- Progressive weight-bearing is initiated based on radiographic evidence of callus formation.
- The hinged brace is gradually opened to allow full ROM.
- Physical therapy focuses on quadriceps activation and hamstring strengthening.
- Phase III (3-6 Months):
- Full weight-bearing is achieved.
- Focus shifts to proprioception, functional rehabilitation, and eventual return to baseline activities.
- Ligamentous stability is reassessed; delayed reconstruction of the cruciate ligaments may be considered if symptomatic instability persists after fracture union.
By adhering to the biomechanical principles outlined by Hohl and Moore, respecting the fragile soft tissue envelope, and maintaining a high index of suspicion for neurovascular compromise, orthopedic surgeons can navigate these devastating fracture-dislocations and optimize patient outcomes.
