Introduction & Epidemiology
Calcaneal fractures represent a challenging subset of orthopedic trauma, accounting for approximately 60% of tarsal bone fractures and 2% of all fractures. These injuries are predominantly high-energy, resulting from axial loading mechanisms such as falls from height, motor vehicle collisions, or industrial accidents. The profound impact on hindfoot mechanics and the high potential for long-term disability underscore the critical importance of meticulous diagnosis and management.
Epidemiologically, calcaneal fractures disproportionately affect younger, economically active males, often leading to significant socioeconomic consequences due to prolonged recovery and potential for permanent impairment. The incidence of associated injuries is considerable, with reports of concurrent spine fractures (thoracolumbar region) in 10-15% of cases, contralateral calcaneal fractures in 5-10%, and other lower extremity injuries (e.g., pilon, talus, pelvic fractures) also frequently observed. Understanding these associations is paramount for a comprehensive patient evaluation.
The intricate anatomy of the calcaneus, particularly its role in subtalar joint function and load transmission, means that even seemingly subtle articular displacement can lead to debilitating post-traumatic arthritis, chronic pain, and significant functional deficits, including gait disturbance and impaired activity participation. Mastery of calcaneal fracture diagnosis, especially concerning the posterior facet and its associated structural integrity, is fundamental to guiding optimal treatment strategies and prognosticating patient outcomes.
Surgical Anatomy & Biomechanics
The calcaneus, the largest tarsal bone, forms the heel of the foot and serves as the primary conduit for transmitting axial loads from the tibia to the ground. Its complex, irregular cuboidal shape and articulations with the talus superiorly and cuboid anteriorly are central to hindfoot function.
Key Anatomical Structures:
- Subtalar Joint: The calcaneus articulates with the talus via three facets: anterior, middle, and posterior. The posterior facet is the largest and most critical for subtalar motion and load bearing. The sustentaculum tali, a shelf-like projection on the medial aspect, supports the middle and anterior facets of the talus and serves as an important anchor for ligaments (e.g., spring ligament) and the flexor hallucis longus tendon.
- Calcaneocuboid Joint: The anterior articulation with the cuboid is a crucial component of the transverse tarsal joint (Chopart's joint), contributing to forefoot mobility.
- Calcaneal Tuberosity: The posterior prominence providing attachment for the Achilles tendon and the plantar aponeurosis. Fractures here often disrupt the lever arm for plantarflexion.
- Angles of Gissane (Critical Angle of Gissane): The angle formed by the intersection of two lines drawn on a lateral radiograph—one along the posterior facet and the other along the anterior process. Normal range is 120-145 degrees. A decrease indicates depression of the lateral portion of the posterior facet.
- Böhler's Angle (Tuber Joint Angle): Formed by the intersection of a line from the superior aspect of the posterior tuberosity to the superior aspect of the posterior facet, and a second line from the superior aspect of the posterior facet to the superior aspect of the anterior process. Normal range is 20-40 degrees. A decrease signifies loss of calcaneal height and subtalar joint depression.
- Peroneal Tubercle: A small lateral eminence separating the tendons of peroneus longus and brevis. Calcaneal widening can lead to impingement of these tendons.
- Neurovascular Structures: The sural nerve courses along the lateral aspect of the hindfoot and is particularly vulnerable during lateral surgical approaches. The posterior tibial neurovascular bundle (tarsal tunnel contents) lies on the medial aspect, susceptible to injury from medial wall blowout fractures or iatrogenic damage during medial approaches.
Biomechanics of Fracture:
High-energy axial loading, typically from a fall onto the heel, drives the talus inferiorly into the calcaneus. The talus acts as a wedge, splitting the calcaneus. The specific fracture pattern is influenced by the vector of force, foot position at impact, and bone quality.
*
Primary Fracture Line:
Often begins in the angle of Gissane, extending obliquely through the calcaneal body, often involving the posterior facet.
*
Secondary Fracture Lines:
Result in various fragment configurations:
*
Sustentacular Fragment:
Often remains attached to the talus via the strong interosseous ligament and usually maintains its position relative to the talus. This makes it a crucial reference point for anatomical reduction.
*
Tuberosity Fragment:
The posterior portion attached to the Achilles tendon. Can be displaced superiorly.
*
Thalamic Fragment:
The main weight-bearing portion of the posterior facet, often depressed and comminuted.
*
Lateral Wall Fragment:
Often comminuted and displaced laterally, contributing to calcaneal widening and peroneal impingement.
Loss of calcaneal height, widening of the body, and varus malalignment are common sequelae, profoundly altering foot biomechanics, leading to decreased subtalar motion, altered gait kinematics, and increased stress on adjacent joints.
Indications & Contraindications
Accurate diagnosis is paramount, integrating clinical examination, plain radiographs, and computed tomography (CT) scans. Initial assessment focuses on the severity of soft tissue injury, which dictates the timing of definitive management.
Imaging Modalities:
*
Plain Radiographs:
Anteroposterior, lateral, and axial (Harris) views are standard. The lateral view allows assessment of Böhler's and Gissane's angles. The axial view evaluates calcaneal widening and varus/valgus alignment. Broden's views (oblique views of the subtalar joint) are sometimes used to evaluate posterior facet congruity.
*
Computed Tomography (CT) Scan:
The gold standard for evaluating calcaneal fractures, especially intra-articular patterns. CT provides detailed information on articular involvement, comminution, fragment displacement, and subtalar joint congruity. 3D reconstructions are invaluable for pre-operative planning.
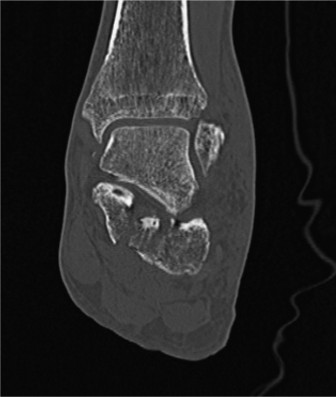
Figure 1: Axial CT scan demonstrating significant intra-articular calcaneal fracture with widening and displacement of the posterior facet.
Classification Systems:
*
Essex-Lopresti Classification:
Based on lateral radiographs, distinguishes between "tongue-type" and "joint depression" fractures, primarily based on the posterolateral fragment. Tongue-type involves a fracture line exiting the posterior tuberosity superiorly. Joint depression involves the posterior facet remaining separate from the tuberosity fragment, which is often depressed.
*
Sanders Classification:
The most widely accepted CT-based classification for intra-articular fractures. It categorizes fractures based on the number and location of primary fracture lines through the posterior facet.
*
Type I:
Non-displaced intra-articular fractures.
*
Type II:
Two-part fractures (IIA: lateral; IIB: central; IIC: medial).
*
Type III:
Three-part fractures (IIAB, IIAC, IIBC).
*
Type IV:
Highly comminuted fractures of the posterior facet.
This classification is highly prognostic and guides surgical approach and expected outcomes.
Indications for Operative vs. Non-Operative Management
The decision-making process for calcaneal fractures is complex, weighing fracture characteristics, patient factors, and surgeon experience.
| Operative Indications | Non-Operative Indications |
|---|---|
| Displaced intra-articular fractures (Sanders Type II, III, IV with >2mm displacement) | Non-displaced or minimally displaced intra-articular fractures (Sanders Type I) |
| Significant loss of Böhler's angle (<15-20°) | Extra-articular fractures without significant displacement or functional compromise |
| Calcaneal widening (>10-15mm) leading to peroneal impingement | Patients with severe comorbidities precluding surgical intervention |
| Varus malalignment leading to impingement | Severe soft tissue envelope compromise (e.g., extensive blistering, deep infection risk) |
| Open fractures (after appropriate debridement) | Advanced age with low functional demand (consider patient-specific factors) |
| Associated compartment syndrome or neurovascular compromise | Uncontrolled diabetes, peripheral vascular disease, heavy smoking (relative contraindications) |
| Talar impingement (often with severe decrease in Böhler's angle) | |
| Significantly displaced sustentaculum tali or anterior process fractures |
Contraindications:
- Absolute Contraindications: Severe, active infection; critically compromised soft tissue envelope (e.g., extensive blistering, skin necrosis, severe open fractures with gross contamination); severe medical comorbidities precluding anesthesia/surgery (ASA Class IV-V).
- Relative Contraindications: Uncontrolled diabetes mellitus; severe peripheral vascular disease; heavy smoking; advanced osteoporosis with severe comminution (Sanders Type IV) where stable fixation is unlikely; patient non-compliance; prolonged delay (>3 weeks) from injury with established malunion.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful surgical outcomes.
Timing of Surgery:
The definitive timing for open reduction internal fixation (ORIF) is critical. Early surgery (<72 hours) is associated with higher rates of wound complications due to acute swelling. Most surgeons advocate for a delayed approach, typically 7-14 days post-injury, allowing for soft tissue swelling to subside, evidenced by the "wrinkle test" (return of skin wrinkles around the ankle).
Advanced Imaging and Review:
Thorough review of plain radiographs, CT scans with multiplanar reconstructions (coronal, sagittal, axial), and 3D reconstructions is essential. The 3D models aid in visualizing the complex fracture pattern, identifying the sustentacular fragment, visualizing the depressed posterior facet, and planning the sequence of reduction maneuvers. This detailed understanding helps in predicting areas of comminution and selecting appropriate plate and screw constructs.
Approach Selection:
The choice of surgical approach depends on the fracture pattern and surgeon's preference:
*
Extensile Lateral Approach (ELA):
The workhorse for most displaced intra-articular fractures, particularly those involving the posterior facet and lateral wall comminution (Sanders Types II-IV). It offers broad exposure.
*
Sinus Tarsi Approach (STA):
A more limited, minimally invasive approach gaining popularity for specific patterns, such as tongue-type fractures or joint depression fractures without extensive lateral wall comminution. It is associated with potentially fewer wound complications.
*
Medial Approach:
Primarily for isolated, displaced sustentaculum tali fractures or severe medial wall blowout with tarsal tunnel impingement.
*
Posterior Approach:
For displaced calcaneal tuberosity avulsion fractures (e.g., "beak" fractures).
Implants:
Pre-contoured calcaneal locking plates are the standard for most intra-articular fractures, providing stable fixation in osteoporotic bone. Various lengths and configurations are available. Cannulated and non-cannulated screws, K-wires, and sometimes external fixators for distraction are also necessary.
Patient Positioning:
*
Prone Position:
Allows simultaneous evaluation of the contralateral lower extremity or spine and provides excellent access for a posterior approach if needed. However, lateral access for C-arm is less optimal.
*
Lateral Decubitus Position:
The most common position for the extensile lateral and sinus tarsi approaches. The affected extremity is positioned superiorly. A bump under the ipsilateral hip helps stabilize the pelvis. This provides optimal C-arm access (AP and lateral views) and surgeon ergonomics.
*
Tourniquet:
A pneumatic tourniquet on the proximal thigh is routinely used to maintain a bloodless field, crucial for visualization.
Pre-Operative Preparation:
Sterile preparation of the entire lower extremity, often extending to the knee, is performed. Prophylactic antibiotics are administered according to institutional protocols.
Detailed Surgical Approach / Technique
This section will primarily detail the Extensile Lateral Approach (ELA) due to its widespread applicability for complex intra-articular calcaneal fractures, with brief mention of the Sinus Tarsi Approach (STA).
Extensile Lateral Approach (ELA)
1. Incision and Flap Elevation:
*
Incision:
A standard L-shaped incision is made. It begins approximately 2 cm posterior and superior to the tip of the lateral malleolus, extends inferiorly over the lateral calcaneal wall, and then turns anteriorly towards the calcaneocuboid joint, roughly paralleling the sole of the foot. The anterior limb should extend far enough to allow access to the anterior process and calcaneocuboid joint.
*
Full-Thickness Flap Elevation:
The most critical step for minimizing wound complications. A full-thickness fasciocutaneous flap, including the sural nerve, peroneal tendons, and their vascular supply, is carefully elevated anteriorly and superiorly. This is performed using sharp dissection, starting at the posterior aspect and progressing anteriorly. The flap is retracted superiorly with stay sutures or small K-wires passed through the skin edge and secured to the tibia. Protection of the sural nerve, which lies subcutaneously, is paramount. The peroneal tendons are typically retracted superiorly with the flap.
2. Exposure and Visualization:
* After flap elevation, the lateral wall of the calcaneus, the peroneal tendons, and the posterolateral corner of the talus are exposed. The lateral wall of the calcaneus is often comminuted and may be removed temporarily (lateral wall osteotomy) to gain direct access to the depressed posterior facet.
* The primary fracture line, typically extending from Gissane's angle, is identified.
3. Reduction Sequence:
The reduction of an intra-articular calcaneal fracture is a systematic, often challenging, multi-step process aiming to restore articular congruity, calcaneal height, length, and width.
- Restoration of Calcaneal Length and Height: Initial maneuver often involves applying traction or distraction across the subtalar joint. This can be achieved with a distraction external fixator (e.g., Schanz pins in the talar neck and calcaneal tuberosity) or manually. This maneuver helps disimpact the fragments and restore the overall length of the calcaneus, correcting the varus deformity often seen.
- De-rotation and Reduction of Tuberosity Fragment: The tuberosity fragment, often rotated into varus, is de-rotated and brought into alignment with the sustentacular fragment. A large reduction clamp (e.g., Verbrugge clamp) or pointed reduction forceps can be used. Provisional fixation with a K-wire from the tuberosity into the sustentaculum tali.
- Lateral Wall Disimpaction and Removal: The comminuted lateral wall is often disimpacted from the underlying depressed posterior facet fragments. Temporarily removing the lateral wall fragments provides direct visualization of the depressed articular surface.
-
Posterior Facet Disimpaction and Reduction:
This is the most crucial step for restoring subtalar joint congruity. The depressed fragments of the posterior facet (thalamic fragments) are elevated from their subchondral depression. This is typically performed using specialized instruments such as lamina spreaders, osteotomes, or elevators (e.g., calcaneal elevators) inserted through the primary fracture line into the depressed fragments. These fragments are carefully elevated, working from posterior to anterior, until anatomical reduction of the posterior facet is achieved. K-wires can be used as joysticks to manipulate individual fragments.
- Crucial Reference Points: The sustentaculum tali fragment, which usually remains anatomically aligned with the talus, serves as the primary reference point for restoring the posterior facet. The reduction of the posterior facet must be precise against the undersurface of the talus.
- Intra-operative Imaging: Frequent fluoroscopic imaging (lateral, axial, Broden's views) is used to confirm articular reduction and restore Böhler's and Gissane's angles.
- Restoration of Böhler's and Gissane's Angles: As the posterior facet is elevated, Böhler's and Gissane's angles are concurrently restored. Aim for Böhler's angle ≥ 20 degrees and Gissane's angle ≥ 120 degrees.
- Provisional Fixation: Once anatomical reduction of the posterior facet is achieved, it is provisionally held with multiple K-wires directed into the sustentaculum tali or healthy calcaneal bone.
- Medial Wall Impingement: If a medial wall blowout fracture is present, resulting in impingement on the tarsal tunnel contents, it must be reduced. This can often be achieved indirectly by correcting the overall calcaneal width and length. Direct access via a separate medial incision may be required in severe cases.
- Lateral Wall Reconstruction: The lateral wall fragments are then reduced and placed back into position, recreating the normal calcaneal width. The lateral wall acts as a buttress to maintain the reduction of the posterior facet.
4. Definitive Fixation:

Figure 2: Intraoperative fluoroscopic image showing anatomical reduction of a calcaneal fracture with stable internal fixation using a pre-contoured locking plate.
- Plate Application: A pre-contoured calcaneal locking plate is selected and positioned on the lateral aspect of the calcaneus. The plate provides stable fixation by bridging the fracture lines and buttressing the lateral wall.
- Screw Placement: Screws are inserted through the plate. It is crucial to obtain good purchase in strong bone fragments, particularly the sustentaculum tali and the calcaneal tuberosity. Locking screws provide angular stability, which is beneficial in comminuted or osteoporotic bone. Careful attention must be paid to screw length and direction to avoid articular penetration (subtalar, calcaneocuboid, talonavicular joints) or impingement on neurovascular structures.
- Bone Grafting: In cases of significant comminution or metaphyseal bone void beneath the reduced posterior facet, cancellous bone graft (autograft or allograft) may be considered to support the reduction and promote healing.
5. Wound Closure:
* After ensuring stable fixation and adequate hemostasis, the wound is meticulously irrigated.
* A drain (e.g., suction drain) is often placed beneath the flap to prevent hematoma formation, which can compromise the flap viability.
* The full-thickness fasciocutaneous flap is carefully re-approximated to its original position. Meticulous layered closure, avoiding tension, is essential. Skin staples or sutures are used for the skin.
Sinus Tarsi Approach (STA)
- Indications: Often used for Sanders Type II/III fractures, especially tongue-type, with less lateral wall comminution.
- Incision: A small curvilinear incision (3-5 cm) is made in the sinus tarsi region, anterior to the lateral malleolus.
- Dissection: Careful dissection through the subcutaneous tissue to avoid the sural nerve. The extensor digitorum brevis muscle is elevated or split, and the sinus tarsi fat pad is removed. This exposes the lateral aspect of the posterior facet.
- Reduction: Indirect reduction maneuvers using K-wires as joysticks and elevators, often guided by distraction (e.g., using a small external fixator or a talar neck Schanz pin).
- Fixation: Typically involves smaller plates, cannulated screws, or a combination. The fixation is less robust than with an ELA, limiting its use to less comminuted patterns.
Complications & Management
Calcaneal fracture surgery is associated with a high rate of complications, highlighting the complexity of these injuries and the unforgiving nature of the soft tissue envelope in the hindfoot.
Early Complications (within 30 days post-op):
| Complication | Incidence | Management/Salvage Strategies |
|---|---|---|
| Wound Dehiscence/Necrosis | 5-25% | Local wound care, strict elevation, debridement of necrotic tissue, negative pressure wound therapy (NPWT), skin grafting/flaps, delayed primary closure. May require hardware removal. |
| Infection (Superficial/Deep) | 2-15% | Superficial: Oral/IV antibiotics, local wound care. Deep: Surgical debridement, IV antibiotics, hardware removal (if stable union), wound vac, possible flap coverage. |
| Sural Nerve Injury | 10-20% | (Neurapraxia to transection). Observation, symptomatic treatment for neuropathic pain. If painful neuroma, surgical excision or neurectomy may be considered. |
| Compartment Syndrome | <1% | Prompt diagnosis with intracompartmental pressure monitoring, urgent fasciotomy (usually 3 compartments: medial, lateral, superficial posterior). |
| Deep Vein Thrombosis (DVT)/PE | Variable | Prophylactic anticoagulation. Diagnosis with Doppler ultrasound/CT pulmonary angiogram. Therapeutic anticoagulation. |
| Hematoma | Common | Expect with thorough closure and drainage. If tense or expanding, evacuation may be required. |
Late Complications:
| Complication | Incidence | Management/Salvage Strategies |
|---|---|---|
| Post-traumatic Subtalar Arthritis | 30-70% | Most common long-term sequela, even with anatomical reduction. NSAIDs, injections, activity modification. Ultimately, subtalar arthrodesis (fusion) is often required. |
| Peroneal Tendon Impingement | 10-20% | Due to residual calcaneal widening. Custom orthotics, physical therapy. May require lateral wall exostectomy, calcaneal osteotomy, or subtalar fusion. |
| Tarsal Tunnel Syndrome | 5-10% | Due to medial wall impingement or fibrosis. NSAIDs, injections. Surgical release of the tarsal tunnel contents. |
| Malunion | Variable | Residual pain, stiffness, gait abnormalities, shoe wear difficulties. Corrective osteotomy (if deformity amenable), subtalar fusion, or triple arthrodesis. |
| Nonunion | Rare (1-2%) | Revision fixation with bone graft, possibly subtalar fusion if symptoms are severe. |
| Hardware Prominence/Irritation | 15-25% | Symptomatic hardware removal after fracture union (typically >12 months post-op). |
| Complex Regional Pain Syndrome (CRPS) | 2-5% | Multidisciplinary pain management, physical therapy, regional nerve blocks, psychological support. Early recognition is key. |
| Chronic Pain/Stiffness | High | Multifactorial. Persistent physical therapy, pain management, shoe modifications, bracing. |
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is essential for optimizing functional outcomes following calcaneal fracture fixation. The timeline and specific interventions are tailored to the individual patient, fracture stability, and surgical approach.
Phase 1: Immediate Post-Operative (0-2 weeks)
*
Goal:
Protect surgical repair, minimize swelling, pain control, initiate early wound healing.
*
Weight Bearing:
Strict
non-weight bearing (NWB)
on the operated extremity.
*
Immobilization:
Posterior splint or bulky soft dressing in slight dorsiflexion, neutral inversion/eversion.
*
Activity:
Strict elevation (above heart level), intermittent ice application.
*
Exercises:
Gentle, pain-free ankle dorsiflexion/plantarflexion (avoiding subtalar motion if fixation requires), toe flexion/extension, quadriceps/gluteal sets, upper extremity conditioning.
*
Wound Care:
Monitor for signs of infection, skin compromise. Dressing changes as per surgeon's protocol. Suture/staple removal typically at 2-3 weeks.
Phase 2: Early Mobilization (2-8 weeks)
*
Goal:
Improve range of motion (ROM), maintain muscle tone, continued protection of healing fracture.
*
Weight Bearing:
Continue
NWB
.
*
Immobilization:
Transition to a removable walking boot or controlled ankle motion (CAM) walker.
*
Activity:
Continue elevation and ice.
*
Exercises:
*
ROM:
Active and passive ankle dorsiflexion/plantarflexion, inversion/eversion (controlled, gentle, and within pain limits, gradually introducing subtalar motion as per surgeon's discretion, often post 6-8 weeks).
*
Strengthening:
Isometric ankle exercises (dorsiflexion, plantarflexion, inversion, eversion) against resistance within the boot, hip and knee strengthening.
*
Balance/Proprioception:
Single leg stance on unaffected leg, core stability exercises.
*
Therapy:
Formal physical therapy typically initiated around 4-6 weeks, focusing on ROM and strength.
Phase 3: Progressive Weight Bearing (8-12+ weeks)
*
Goal:
Gradually reintroduce weight bearing, improve gait, increase strength and endurance.
*
Weight Bearing:
Progression to
partial weight bearing (PWB)
begins, typically around 8-12 weeks, contingent on radiographic evidence of healing and pain tolerance. This is done in the CAM walker, gradually increasing load.
*
Activity:
Continue with home exercise program and formal physical therapy.
*
Exercises:
*
Weight Bearing:
PWB with crutches/walker, progressing to full weight bearing (FWB) as tolerated.
*
Strengthening:
Calf raises (bilateral progressing to unilateral), resistance band exercises for ankle, stair climbing.
*
Gait Training:
Focus on proper heel-toe gait pattern without limping.
*
Balance/Proprioception:
Increased challenge with single-leg stance, uneven surfaces.
*
Transition:
Gradually wean off CAM walker and transition to supportive, comfortable shoes. Custom orthotics may be considered for arch support and alignment.
Phase 4: Advanced Rehabilitation / Return to Activity (3-6+ months)
*
Goal:
Maximize strength, endurance, agility, and return to pre-injury activities.
*
Weight Bearing:
Full weight bearing in supportive shoes.
*
Activity:
Continue with aggressive strengthening and conditioning.
*
Exercises:
*
Functional:
Hopping, jumping, sport-specific drills (if applicable), plyometrics.
*
Endurance:
Treadmill walking, cycling, swimming.
*
Flexibility:
Continued stretching of the Achilles tendon and plantar fascia.
*
Return to Sport/High-Impact Activities:
Typically not before 6-12 months, and often longer, dependent on clinical progress, pain levels, and radiographic consolidation. High-impact activities may need to be permanently modified.
*
Long-Term Follow-up:
Regular clinical and radiographic assessment to monitor for complications such as post-traumatic arthritis or malunion.
Patient education regarding the potential for long-term residual stiffness, pain, and the possibility of future interventions (e.g., subtalar fusion for arthritis) is crucial throughout the rehabilitation process.
Summary of Key Literature / Guidelines
The management of calcaneal fractures, particularly displaced intra-articular types, has evolved significantly, guided by landmark studies and ongoing research.
- Essex-Lopresti (1951): His seminal work described the mechanism and characteristic fracture patterns (tongue-type vs. joint depression), laying the foundation for understanding these complex injuries.
- Sanders Classification (1993): Developed by Sanders et al., this CT-based classification system revolutionized the assessment of intra-articular calcaneal fractures. It provides a reliable and reproducible method for categorizing fracture severity and guiding treatment, becoming the most widely accepted system due to its prognostic value.
- Canadian Orthopaedic Trauma Society (COTS) Randomized Controlled Trial (2001): This large, multicenter study compared operative versus non-operative management for displaced intra-articular calcaneal fractures. It demonstrated that while ORIF improved functional outcomes for certain subgroups (e.g., younger, non-smoking females, patients not on Workers' Compensation), it did not show a universal benefit over non-operative care for all patients. The study highlighted the importance of patient selection, comorbidities, and the challenging nature of these injuries. This trial significantly influenced practice, leading to a more nuanced approach to surgical indications.
- Meta-analyses and Systematic Reviews: Numerous subsequent meta-analyses have largely supported the COTS findings, emphasizing that while ORIF can yield better anatomical and functional outcomes for appropriately selected patients (e.g., good soft tissue envelope, Sanders Type II/III, relatively younger age, good general health), the procedure is associated with high complication rates, particularly wound-related issues. The consensus reinforces individualized treatment based on fracture pattern, patient comorbidities, functional demands, and the surgeon's expertise.
- Minimally Invasive Approaches (Sinus Tarsi Approach): A growing body of literature supports the use of minimally invasive techniques, particularly the Sinus Tarsi Approach (STA), for specific fracture patterns (e.g., less comminuted Sanders Type II/III, tongue-type fractures). Studies suggest that STA may achieve comparable functional outcomes to the extensile lateral approach with a potentially lower incidence of wound complications, though often with less direct visualization of the entire posterior facet. This approach typically requires a steep learning curve and precise technique.
- Future Directions: Current research focuses on improving internal fixation constructs (e.g., patient-specific implants, novel materials), optimizing surgical techniques, enhancing soft tissue management strategies to reduce wound complications, and developing more sophisticated rehabilitation protocols. There is also increasing interest in advanced imaging techniques, biomechanical modeling, and personalized medicine approaches to predict outcomes and tailor interventions more effectively.
In summary, the contemporary management of calcaneal fractures demands a sophisticated understanding of their anatomy, biomechanics, and the various classification systems. The decision for operative versus non-operative treatment is complex and should be made collaboratively with the patient, considering all relevant factors. While surgical reduction and stable fixation aim to restore anatomical relationships and improve long-term function, the inherent challenges of soft tissue compromise and the potential for debilitating complications necessitate meticulous technique and a comprehensive post-operative rehabilitation strategy.
