Patient Presentation & History
We present the case of a 32-year-old professional ballet dancer, female, presenting with a 14-month history of insidious onset right posterior ankle pain. The patient reports a gradual increase in symptoms, initially presenting as a dull ache during pliés and relevés, progressing to sharp, debilitating pain with sustained pointe work and during the push-off phase of jumping. The pain is exacerbated by passive dorsiflexion of the ankle and hallux extension, as well as active hallux flexion against resistance. She describes occasional subjective "catching" or "snapping" sensation in the posterior ankle, particularly when initiating movement after a period of rest.
Her past medical history is unremarkable. She denies any specific acute traumatic event, attributing the onset to cumulative microtrauma inherent to her profession. She reports no systemic inflammatory conditions, diabetes mellitus, or other relevant comorbidities. Prior conservative management, supervised by her company's physical therapist, included activity modification, relative rest, non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroid injection into the posterior ankle joint (under ultrasound guidance, approximately six months prior), and a structured rehabilitation program focusing on ankle and foot intrinsic muscle strengthening, Achilles stretching, and proprioceptive exercises. Despite these interventions, her symptoms have remained refractory, significantly impacting her ability to perform and necessitating a full work stoppage for the past three months. She expresses a strong desire to return to her elite-level performance.
Clinical Examination
Inspection
On inspection, the patient presented with subtle, diffuse swelling localized to the posteromedial aspect of the right ankle, compared to the contralateral limb. There was no obvious erythema, warmth, or skin discoloration. Gait analysis demonstrated a cautious, shortened stance phase on the right foot, with reduced push-off and an antalgic component during ambulation. Active range of motion of the ankle revealed a painful arc during full plantarflexion and dorsiflexion, with an evident restriction in the terminal range of dorsiflexion. Active flexion of the great toe against resistance reproduced her pain and demonstrated a subtle weakness compared to the left. No specific deformities of the foot or ankle were noted, and arches were well-maintained.
Palpation
Palpation elicited exquisite tenderness along the course of the flexor hallucis longus (FHL) tendon, specifically posterior to the medial malleolus and within the fibro-osseous tunnel distal to the talar body. Pressure applied directly over the os trigonum region (if present) also reproduced her symptoms. A subtle crepitus was noted with passive motion of the great toe during palpation. The posterior aspect of the talus, in the interval between the Achilles tendon and the posterior tibial neurovascular bundle, was tender. The deltoid ligament complex and posterior tibial tendon were non-tender.
Range of Motion
-
Ankle:
- Dorsiflexion: 10 degrees (painful at end range, contralateral 20 degrees)
- Plantarflexion: 40 degrees (painful at end range, contralateral 50 degrees)
- Inversion: 25 degrees (contralateral 30 degrees)
- Eversion: 10 degrees (contralateral 15 degrees)
-
Hallux:
- Interphalangeal joint flexion: Full, but painful against resistance.
- Metatarsophalangeal joint flexion: Full, painful against resistance.
Specific provocative maneuvers for FHL tenosynovitis were performed:
*
FHL Palpation with Passive Hallux Motion:
Significant pain and crepitus noted when the great toe was passively moved from extension to flexion while palpating the FHL tendon posterior to the medial malleolus.
*
Resisted Hallux Flexion:
Pain sharply reproduced along the FHL tendon and posterior ankle.
*
Posterior Ankle Impingement Test (forced passive plantarflexion):
Reproduction of posterior ankle pain.
*
FHL "Flicker" Sign (Wedge Test):
This test involves passively extending the great toe and then rapidly flexing it while the ankle is in moderate plantarflexion. A palpable or audible "flick" or "snap" was noted along the FHL sheath, reproducing the patient's symptoms, indicative of stenosing tenosynovitis or impingement.
Neurological/Vascular Assessment
Sensory examination revealed intact sensation to light touch and pinprick in all dermatomes of the foot. Motor strength was graded 5/5 in all major muscle groups except for hallux flexion, which was subjectively 4/5 due to pain, with some objective weakness. Deep tendon reflexes (Achilles, patellar) were 2+ bilaterally.
Peripheral pulses (dorsalis pedis, posterior tibial) were strong and symmetric bilaterally. Capillary refill was brisk (<2 seconds) in all digits. No signs of neurovascular compromise were present.
Imaging & Diagnostics
Radiographs
Initial weight-bearing radiographs of the right foot and ankle (anteroposterior, lateral, oblique views) were obtained. These revealed:
* No acute fracture or dislocation.
* Slightly increased sclerosis of the posterior process of the talus, consistent with a moderately sized os trigonum, without clear signs of recent fracture.
* No significant osteophyte formation in the posterior ankle joint.
* No degenerative changes in the subtalar or ankle joints.
* Normal alignment of the hindfoot.
These findings suggested the presence of an anatomical variant (os trigonum) that could contribute to posterior ankle impingement and FHL pathology.
Magnetic Resonance Imaging (MRI)
Given the chronicity of symptoms and failure of conservative management, an MRI of the right ankle without contrast was performed. The MRI provided critical soft tissue detail:
- FHL Tendon: Diffuse tenosynovitis of the flexor hallucis longus tendon sheath was evident, characterized by significant fluid accumulation and synovial thickening extending from the posteromedial ankle distal to the subtalar joint. There was mild intrasubstance signal alteration within the FHL tendon consistent with tendinosis, but no overt tendon tear. The tendon showed mild hypertrophy.
- Fibro-osseous Tunnel: Significant narrowing of the FHL fibro-osseous tunnel was noted, with the FHL tendon appearing compressed and exhibiting an acute angle as it courses around the posterior talus and sustentaculum tali.
- Os Trigonum: A well-corticated, separate os trigonum was clearly visualized, approximately 8x6x5 mm in size, situated posterior to the talar body. It appeared to impinge upon the FHL tendon with ankle plantarflexion. Edema was noted within the soft tissues surrounding the os trigonum, suggesting an inflammatory response.
- Posterior Talus: There was no significant posteromedial osteophyte or other bony impingement from the talar body itself, beyond the presence of the os trigonum.
- Associated Findings: Mild synovitis within the posterior ankle joint recess was observed. The Achilles tendon and posterior tibial tendon were intact with normal signal characteristics. No significant pathology of the peroneal tendons or other ankle ligaments was noted.
- Neurovascular Bundle: The posterior tibial neurovascular bundle was noted in close proximity to the FHL tendon, immediately medial, emphasizing the need for careful dissection during any intervention.
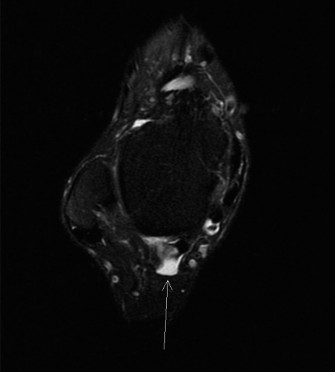
Figure 1: Representative MRI axial view of the FHL tendon within its fibro-osseous tunnel. Note the close proximity of the posterior tibial neurovascular bundle (medial to FHL). This image illustrates typical findings in FHL pathology, demonstrating the FHL tendon (often with increased signal or surrounding fluid) constrained by its anatomical tunnel.
Ultrasound
Dynamic ultrasound could have been considered for real-time visualization of the FHL tendon during movement and to guide injections, but was not primarily utilized in this case given the comprehensive MRI findings.
Templating
Pre-operative planning involved reviewing the MRI to delineate the exact anatomical course of the FHL tendon and its relationship to the os trigonum and posterior neurovascular bundle. This detailed understanding was crucial for selecting the appropriate surgical approach and ensuring comprehensive decompression while minimizing iatrogenic injury. The size and position of the os trigonum were templated for potential excision.
Differential Diagnosis
The chronicity of posterior ankle pain in a ballet dancer warrants a comprehensive differential diagnosis. Given the clinical findings and imaging, the primary diagnosis remained FHL tenosynovitis with associated os trigonum syndrome and posterior ankle impingement. However, several other conditions must be considered and distinguished.
| Condition | Key Clinical Features | Key Imaging Findings (MRI) | Distinguishing Factors |
|---|---|---|---|
| FHL Tenosynovitis (Primary) | Posterior ankle pain, pain with great toe flexion/extension, palpable crepitus, FHL flicker sign, weakness on resisted hallux flexion. | Tendon sheath effusion, synovial hypertrophy, intrasubstance tendinosis, narrowing of fibro-osseous tunnel. Often co-exists with os trigonum. | Our Case: Patient presented with classic symptoms, FHL flicker sign, and specific tenderness. MRI directly confirmed FHL tenosynovitis and tendinosis. This was the central pathology. |
| Os Trigonum Syndrome | Posterior ankle pain, worse with forced plantarflexion (impingement), tenderness over posterior talus. May present with snapping/catching. | Separate os trigonum posterior to talus, surrounded by edema/inflammation. Often associated with FHL tenosynovitis. | Our Case: Radiographs and MRI showed a definite os trigonum. While present and likely contributing to impingement, the MRI showed significant FHL tenosynovitis extending beyond just the os trigonum. The FHL flicker sign pointed to primary FHL involvement. |
| Posterior Ankle Impingement Syndrome (PAIS) | Posterior ankle pain, exacerbated by forced plantarflexion. May be osseous or soft tissue. | Osseous (osteophytes, os trigonum, Stieda's process) or soft tissue (synovitis, hypertrophic fat pad, thickened posterior capsule) lesions impinging on posterior talus/tibia. | Our Case: The os trigonum is an osseous impingement lesion, and the FHL tenosynovitis contributes to soft tissue impingement. PAIS is a broader syndrome, and in this case, FHL tenosynovitis and os trigonum syndrome are the specific etiologies contributing to PAIS. |
| Achilles Tendinopathy | Pain and tenderness over Achilles tendon (2-6 cm proximal to insertion), worse with activity, resisted plantarflexion. | Thickened Achilles tendon, signal changes (tendinosis), peritendinous edema, +/- tear. Often a fusiform swelling. | Our Case: Tenderness was specifically medial to the Achilles tendon. Achilles tendon was normal on palpation and MRI. Resisted plantarflexion was painful due to overall ankle strain, but less so than resisted great toe flexion. |
| Posterior Tibial Tendon Dysfunction (PTTD) | Medial ankle pain, flatfoot progression, inability to perform single-leg heel raise, tenderness along PTT course. | PTT signal change (tendinosis), thickening, longitudinal tears, peritendinous fluid. Often associated with hindfoot valgus. | Our Case: No evidence of flatfoot deformity or hindfoot valgus. PTT was non-tender and normal on MRI. Symptoms were clearly related to great toe mechanics and posterior talar region, not the entire medial longitudinal arch support. |
| Tarsal Tunnel Syndrome | Burning pain, numbness, tingling in foot (medial plantar, lateral plantar, calcaneal nerve distribution), exacerbated by activity. | Entrapment of posterior tibial nerve or its branches (e.g., by space-occupying lesion, edema). | Our Case: Predominantly mechanical pain, not neuropathic. No specific radiating pain or paresthesias in typical nerve distributions, though chronic inflammation could potentially cause secondary nerve irritation. MRI did not show overt nerve compression. |
Surgical Decision Making & Classification
The decision for surgical intervention was made after a prolonged course of non-operative management (14 months) had demonstrably failed. The patient’s symptoms were chronic, debilitating, and significantly impacted her professional livelihood. Key factors leading to surgery included:
- Refractory Symptoms: Persistent, severe pain despite a comprehensive and well-executed conservative treatment regimen, including physical therapy, activity modification, NSAIDs, and a corticosteroid injection.
- Mechanical Symptoms: The presence of a clear FHL "flicker" sign and subjective "catching" suggested a mechanical impediment within the tendon sheath, often not amenable to conservative treatment alone.
- Imaging Evidence of Structural Pathology: MRI confirmed significant FHL tenosynovitis, tendinosis, and the presence of a symptomatic os trigonum causing impingement. This objective evidence supported a structural cause for her chronic pain.
- Patient's Functional Demands: As an elite ballet dancer, the patient requires a full, pain-free range of motion and maximal strength from her ankle and hallux. Returning to this level of function typically necessitates addressing the underlying mechanical impingement.
Classification
While there isn't a universally accepted classification specific for FHL tenosynovitis severity, findings can be graded:
*
Grade I:
Peritendinous edema, minimal fluid.
*
Grade II:
Significant fluid, synovial thickening.
*
Grade III:
Tendon thickening, signal changes (tendinosis), potential for stenosis.
*
Grade IV:
Frank tendon rupture (rare, not present here).
Our patient presented with findings consistent with a Grade III FHL tenosynovitis due to the tendinosis and significant synovial thickening. The concomitant os trigonum syndrome further complicated the pathology, placing her condition within the broader category of posterior ankle impingement syndrome, specifically of combined osseous and soft tissue etiology.
The goals of surgery were to:
1. Decompress the FHL tendon sheath.
2. Perform a tenosynovectomy to remove inflamed and hypertrophic synovium.
3. Excise the symptomatic os trigonum and any other impinging osseous or soft tissue lesions.
4. Restore pain-free range of motion and function to facilitate return to high-level activity.
Surgical Technique / Intervention
The patient underwent a right posterior ankle arthroscopy with flexor hallucis longus tenosynovectomy and os trigonum excision.
Patient Positioning
The patient was positioned prone on the operating table. A pneumatic tourniquet was applied to the proximal thigh. The limb was prepped and draped in the usual sterile fashion. A bump was placed under the ipsilateral hip to facilitate access. A traction tower could be used, but for this specific procedure, it was not deemed necessary.
Anesthesia
General anesthesia was administered.
Approach
A standard posterior ankle arthroscopy approach was utilized, establishing two primary portals:
1.
Posterolateral Portal:
Located just lateral to the Achilles tendon, approximately 1 cm proximal to the calcaneal tuberosity. This portal is typically the viewing portal.
2.
Posteromedial Portal:
Located just medial to the Achilles tendon, approximately 1 cm proximal to the calcaneal tuberosity. This portal serves as the working portal.
Care was taken to identify and protect the sural nerve laterally and the posterior tibial neurovascular bundle medially.
Procedure
-
Portal Creation & Initial Assessment:
- A spinal needle was used to identify the safe zone for portal placement, ensuring avoidance of neurovascular structures.
- The posterolateral portal was established first. A small skin incision was made, followed by blunt dissection with a hemostat down to the capsule. The arthroscope (2.7 mm, 30-degree) was then inserted into the posterior compartment of the ankle.
- Distension of the posterior compartment with saline was crucial for visualization and to create space.
- The posteromedial portal was then established under direct arthroscopic visualization using the "outside-in" technique.
-
Assessment of Posterior Compartment:
- Initial visualization revealed significant synovitis within the posterior compartment of the ankle.
- The FHL tendon was identified, crossing the posterior aspect of the talus, medial to the subtalar joint. It appeared thickened, inflamed, and was tightly constrained within its fibro-osseous tunnel.
- The os trigonum was clearly visible, superior and medial to the FHL tendon, causing direct mechanical impingement during simulated ankle motion.
-
FHL Tenosynovectomy and Decompression:
- A shaver (3.5 mm, full-radius) was introduced through the posteromedial working portal.
- A meticulous tenosynovectomy of the FHL tendon sheath was performed, carefully debriding all hypertrophic and inflamed synovium surrounding the tendon. This step was critical for relieving the stenosing component of the tenosynovitis.
- The fibro-osseous tunnel was then identified, and the retinacular structures overlying the FHL tendon were released longitudinally to decompress the tendon. This widened the space for the FHL tendon, allowing it to glide freely without impingement. Care was taken to avoid over-release that might lead to tendon subluxation, though this is rare in the posterior ankle.
-
Os Trigonum Excision:
- Using the shaver and a specialized arthroscopic burr, the inflammatory tissue surrounding the os trigonum was debrided.
- The os trigonum, which was impinging on the FHL tendon and posterior talus, was carefully resected using the burr. Fragments were removed with a grasping forceps. The underlying talar bone was smoothed to prevent further impingement.
- Thorough irrigation and aspiration were performed to remove all loose bodies and debris.
-
Final Assessment:
- Dynamic assessment of the FHL tendon was performed under arthroscopic visualization, confirming smooth gliding of the tendon through the decompressed tunnel.
- Full passive range of motion of the ankle and great toe was confirmed without impingement or mechanical block.
- All bleeding was controlled, and the posterior compartment was irrigated thoroughly.
Closure
The portals were closed with a single non-absorbable suture (e.g., 3-0 Nylon). Sterile dressings were applied, and the ankle was placed in a non-weight-bearing posterior splint in a neutral position for comfort and initial protection.
Post-Operative Protocol & Rehabilitation
The post-operative protocol was designed to minimize initial pain and swelling, promote soft tissue healing, and gradually restore full, pain-free function.
Phase 1: Immediate Post-Operative (Weeks 0-2)
- Immobilization: Posterior splint for 3-5 days for pain control and initial swelling reduction, then transition to a walking boot (CAM walker) in neutral position.
- Weight-Bearing: Non-weight-bearing (NWB) with crutches for the first 1-2 weeks.
- Pain Management: Oral analgesics (NSAIDs, acetaminophen, short-course opioids as needed). Ice and elevation are crucial.
-
Rehabilitation:
- Gentle ankle plantarflexion/dorsiflexion within pain limits (in the boot when removed for exercises).
- Active great toe flexion/extension without resistance, emphasizing smooth gliding of the FHL tendon.
- Subtalar inversion/eversion, maintaining range of motion.
- Core stability exercises and upper extremity conditioning.
- Wound Care: Maintain clean, dry dressings. Suture removal around Day 10-14.
Phase 2: Early Mobilization & Strengthening (Weeks 2-6)
- Weight-Bearing: Gradual progression to partial weight-bearing (PWB) in the walking boot from week 2-3, advancing to full weight-bearing (FWB) as tolerated by week 4-6, still in the boot initially.
-
Rehabilitation:
- Continue active ROM exercises for ankle and great toe.
- Begin gentle passive range of motion for the ankle.
- Introduce light resistance for great toe flexion (e.g., therapeutic putty, theraband).
- Ankle isometric exercises (dorsiflexion, plantarflexion, inversion, eversion).
- Proprioceptive exercises: non-weight-bearing alphabet, seated balance board.
- Initiate soft tissue massage around the surgical site to prevent scar tissue formation.
- Discontinuation of Boot: Once FWB is comfortable and pain is minimal (around week 4-6), transition out of the walking boot and into supportive athletic footwear.
Phase 3: Advanced Strengthening & Proprioception (Weeks 6-12)
- Weight-Bearing: Full weight-bearing in supportive shoes.
-
Rehabilitation:
- Progressive strengthening exercises: calf raises (double and single leg), resisted ankle movements, single-leg balance activities (e.g., wobble board, Bosu ball).
- Advanced FHL strengthening: great toe curls with towel, marble pick-ups, sustained resisted great toe flexion.
- Plyometric preparation: light hopping, jumping, and agility drills, gradually increasing intensity.
- Sport-specific drills for ballet dancers, including gentle pliés and relevés without pointe work.
- Emphasis on kinetic chain integration, including hip and core strength.
Phase 4: Return to Activity (Weeks 12-24+)
-
Rehabilitation:
- Gradual reintroduction of advanced ballet-specific activities, initially flat, then progressing to demi-pointe and pointe work under strict supervision.
- Progressive increase in intensity, duration, and frequency of training.
- Emphasis on proper technique, biomechanics, and preventing recurrence.
- Continued strengthening and proprioceptive exercises.
- Return to Sport: Full return to high-level ballet performance is typically expected between 4-6 months, depending on individual progress and the demanding nature of the sport. Close communication between the surgeon, physical therapist, and ballet instructor is paramount.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Thorough History: Always inquire about the mechanism of injury (acute vs. chronic microtrauma), activity level (dancers, athletes, repetitive stress), specific movements that exacerbate pain (e.g., pointe work, push-off), and the presence of mechanical symptoms (snapping, catching).
- Comprehensive Physical Examination: Do not solely focus on the posterior ankle. Assess overall foot and ankle alignment, gait, full active and passive ROM. Critically evaluate the FHL tendon course: palpate from the muscle belly to the great toe. Perform specific FHL tests (resisted hallux flexion, FHL flicker sign) and posterior ankle impingement tests. Differentiate from Achilles, PTT, and peroneal pathologies.
-
High-Quality Imaging:
- X-rays: Essential to rule out bony pathologies like os trigonum, posterior talar process fractures, calcaneal stress fractures, and subtle osteophytes.
- MRI: The gold standard for soft tissue evaluation. Look for FHL tenosynovitis (fluid, synovial hypertrophy), tendinosis, compression within the fibro-osseous tunnel, and associated lesions (os trigonum, osteophytes, loose bodies, posterior ankle synovitis). This helps guide surgical planning.
- Anatomical Knowledge: A deep understanding of the posterior ankle anatomy, especially the relationship of the FHL tendon to the posterior tibial neurovascular bundle (medial) and the flexor digitorum longus (lateral), is paramount for safe surgical dissection.
- Arthroscopic Approach Advantages: Posterior ankle arthroscopy provides excellent visualization, minimizes soft tissue dissection, allows for comprehensive tenosynovectomy and os trigonum excision, and facilitates early rehabilitation. It offers a minimally invasive option for addressing both soft tissue and osseous impingement.
- Gradual Rehabilitation: Emphasize a structured, progressive rehabilitation program, particularly for high-demand athletes. Early gentle motion of the great toe is important to prevent adhesions, but protected weight-bearing is crucial initially. Close liaison with a sports-specialized physical therapist is invaluable.
Pitfalls
- Missed Associated Pathologies: FHL tenosynovitis frequently co-exists with os trigonum syndrome, posterior ankle impingement, or other foot/ankle pathologies. A narrow diagnostic focus can lead to incomplete treatment and persistent symptoms.
- Inadequate Decompression: Insufficient release of the fibro-osseous tunnel or incomplete tenosynovectomy can lead to recurrent stenosing symptoms. Ensure the FHL tendon glides freely at the end of the procedure.
- Iatrogenic Neurovascular Injury: The posterior tibial neurovascular bundle lies in close proximity (medial) to the FHL tendon. Careless portal placement or aggressive dissection, especially with the shaver, can lead to direct nerve injury, resulting in permanent paresthesias or weakness. Similarly, the sural nerve laterally must be protected.
- Failure to Address the Os Trigonum: If a symptomatic os trigonum is present and contributing to impingement, merely decompressing the FHL tendon will not resolve all symptoms. Comprehensive treatment requires excision of the os trigonum.
- Overly Aggressive Early Rehabilitation: While early mobilization is generally beneficial, pushing the patient too hard, especially with high-impact activities or pointe work too soon, can lead to inflammation, scar tissue formation, or even re-injury. Adherence to a structured, phased protocol is key.
- Misdiagnosis: Confusing FHL pathology with Achilles tendinopathy, PTTD, or other causes of posterior ankle pain can lead to inappropriate treatment. The specific clinical tests (FHL flicker, resisted hallux flexion) are crucial for differentiation.
- Recurrence: While rare, recurrence can happen if the underlying biomechanical issues (e.g., excessive repetitive plantarflexion) are not addressed in rehabilitation or if the decompression was suboptimal.
