Introduction & Epidemiology
Achilles tendinopathy (AT) represents a prevalent and often debilitating overuse injury affecting the triceps surae complex, primarily involving the Achilles tendon. This degenerative condition is characterized by pain, stiffness, and impaired function, significantly impacting an individual's quality of life and athletic participation. From an epidemiological perspective, AT is ubiquitous, observed in both athletic and sedentary populations, though incidence rates are notably higher among runners, jumpers, and individuals engaged in sports requiring repetitive ankle dorsiflexion and plantarflexion. Estimates suggest an incidence of up to 50% in elite long-distance runners over a lifetime, and it accounts for 6-17% of all running injuries.
The pathophysiology of AT is now largely understood as a failed healing response rather than a purely inflammatory process (tendinitis). Histopathological examination typically reveals collagen disorganization, tenocyte hyperplasia, neovascularization, and an increase in ground substance, with minimal inflammatory cell infiltrate. This distinction underscores the shift in treatment paradigms from anti-inflammatory approaches to regenerative and mechanobiological strategies.
Clinically, AT is categorized into two main types:
*
Non-insertional Achilles Tendinopathy (NIAT):
Affecting the mid-portion of the tendon, typically 2-6 cm proximal to its calcaneal insertion. This region is considered a "watershed area" with relatively poorer vascularity, making it susceptible to degenerative changes.
*
Insertional Achilles Tendinopathy (IAT):
Occurring at the tendon-bone interface, often associated with a Haglund's deformity (posterolateral calcaneal prominence) and retrocalcaneal bursitis.
Both forms are characterized by activity-related pain, localized tenderness, and morning stiffness. Despite differing anatomical locations, the underlying etiology often involves repetitive microtrauma exceeding the tendon's adaptive capacity, leading to a breakdown in the collagen matrix and subsequent structural disorganization. Non-operative management, particularly focused on eccentric loading exercises, remains the cornerstone of treatment for the vast majority of cases, aiming to stimulate tendon remodeling and improve load tolerance.
Surgical Anatomy & Biomechanics
A thorough understanding of the Achilles tendon's anatomy and biomechanics is fundamental for effective diagnosis and management of its pathologies. The Achilles tendon (tendo calcaneus) is the largest and strongest tendon in the human body, formed by the conjoined aponeuroses of the gastrocnemius (medial and lateral heads), soleus, and often the plantaris muscles.
Anatomical Considerations
-
Triceps Surae:
- Gastrocnemius: A biarticular muscle originating from the femoral condyles, primarily responsible for powerful plantarflexion and knee flexion. Its fast-twitch fibers contribute to explosive movements.
- Soleus: A uniarticular muscle originating from the tibia and fibula, primarily responsible for sustained plantarflexion, especially important during standing and walking. Its slow-twitch fibers provide endurance.
- Plantaris: A small, rudimentary muscle with a long, thin tendon that typically inserts medial to the Achilles tendon on the calcaneus. Its function is minor, but its tendon can be confused with the Achilles or involved in specific pathologies.
- Tendon Insertion: The Achilles tendon inserts onto the posterior aspect of the calcaneus, encompassing the middle third of the tuberosity. The fibers splay out at their insertion, forming a broad footprint. Superficial fibers insert more proximally than deep fibers, providing a strong anchoring point.
- Blood Supply: The Achilles tendon receives its blood supply from multiple sources, including the posterior tibial artery (via the peritendinous plexus), peroneal artery, and calcaneal branches. A relatively hypovascular region (the "watershed area") exists approximately 2-6 cm proximal to the calcaneal insertion, which correlates with the common site of non-insertional tendinopathy and acute ruptures.
- Innervation: Primarily from the tibial nerve (S1, S2) to the triceps surae muscles. The sensory innervation of the tendon and paratenon is less clearly defined but involves branches from the sural nerve laterally and the tibial nerve medially. The sural nerve, formed by contributions from the tibial and common peroneal nerves, runs subcutaneously along the lateral aspect of the Achilles tendon, making it vulnerable during surgical approaches.
- Paratenon: A highly vascularized fascial sheath surrounding the Achilles tendon, providing nourishment and facilitating smooth gliding. In tendinopathy, thickening and adhesions of the paratenon can contribute to pain and dysfunction.
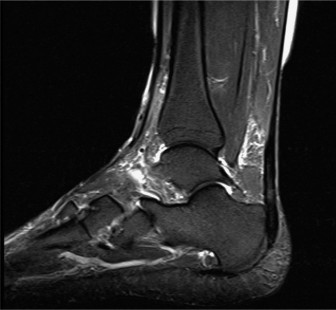
Figure 1: Illustration of the Achilles tendon and its anatomical relationships, including the triceps surae muscles and the retrocalcaneal bursa.
Biomechanics of the Achilles Tendon
The Achilles tendon acts as a critical link in the kinetic chain of the lower extremity, transmitting forces from the triceps surae to the foot. Its primary biomechanical functions include:
*
Plantarflexion:
Essential for propulsion during gait, running, and jumping.
*
Energy Storage and Release:
During the stance phase of gait, the tendon is elongated and stores elastic energy, which is then released during push-off, contributing to efficient locomotion.
*
Shock Absorption:
Eccentric contraction of the triceps surae and controlled lengthening of the Achilles tendon help absorb ground reaction forces upon landing.
Mechanobiology of Tendinopathy
The development of AT is intimately linked to the tendon's response to mechanical loading. Healthy tendons adapt to load through collagen synthesis and remodeling. However, excessive or unaccustomed repetitive loading, insufficient recovery periods, or impaired cellular responses can lead to a breakdown in this adaptive process.
*
Repetitive Microtrauma:
Leads to accumulation of micro-damage.
*
Impaired Healing:
Instead of normal repair, the tendon undergoes a degenerative process involving altered tenocyte morphology, increased production of proteoglycans (leading to increased water content), disoriented collagen fibers, and neovascularization (often associated with pain nerves).
*
Eccentric Loading:
The therapeutic effect of eccentric calf stretching in AT is believed to stem from its ability to:
1.
Promote Tendon Remodeling:
Eccentric contractions place tensile stress on the tendon during lengthening, which is thought to stimulate collagen synthesis, alignment of collagen fibers, and improve load tolerance.
2.
Reduce Neovascularization and Neoinnervation:
Some theories suggest that eccentric exercises may mechanically compress or reduce activity in the pathological neovessels and associated pain nerves, though this mechanism is still debated.
3.
Strengthen the Muscle-Tendon Unit:
Improves the capacity of the triceps surae to absorb and generate force, reducing stress on the tendon itself.
The precise mechanisms are complex, but the overwhelming clinical evidence supports the efficacy of eccentric loading as a primary non-operative intervention.
Indications & Contraindications
The management of Achilles tendinopathy typically follows a stepwise approach, prioritizing conservative measures before considering surgical intervention. The decision-making process hinges on the duration of symptoms, severity of pain and dysfunction, response to non-operative treatment, and specific anatomical pathologies.
Non-Operative Indications
Non-operative management is the first-line treatment for the vast majority of Achilles tendinopathy cases, regardless of insertional or non-insertional type.
*
Acute/Subacute Presentation:
Patients presenting with symptoms for less than 3-6 months.
*
Mild to Moderate Pain and Dysfunction:
Cases where pain is manageable, and functional limitations are not severe enough to warrant immediate surgical consideration.
*
No Significant Structural Pathology:
Absence of large tendon nodules, substantial Haglund's deformity, or calcific deposits that may mechanically impede function or response to conservative care.
*
Patient Compliance:
Willingness and ability to adhere to a structured rehabilitation program, including eccentric loading exercises, activity modification, and other supportive measures.
*
Pre-operative Optimization:
Even in cases eventually requiring surgery, a trial of comprehensive non-operative treatment is standard to optimize tendon health and patient conditioning.
Operative Indications
Surgical intervention for Achilles tendinopathy is generally reserved for cases refractory to a prolonged and comprehensive course of non-operative treatment.
*
Chronic, Debilitating Tendinopathy:
Persistent pain and functional impairment despite at least 6-12 months of well-supervised non-operative management, including eccentric loading protocols, physical therapy, activity modification, and appropriate orthotics.
*
Large Tendon Nodules/Degenerative Lesions:
Palpable, painful tendon thickening or visible lesions on imaging (MRI) that fail to respond to conservative care and may be a source of mechanical impingement or structural weakness.
*
Insertional Tendinopathy with Significant Haglund's Deformity:
Chronic posterior heel pain associated with a prominent posterosuperior calcaneal tuberosity (Haglund's deformity), often accompanied by calcaneal spurring, retrocalcaneal bursitis, and symptomatic insertional tendinopathy.
*
Partial Achilles Ruptures:
While many partial ruptures can be managed non-operatively, surgical repair may be indicated for larger tears (>25-50% cross-sectional area), persistent pain, functional instability, or in active individuals with high functional demands who fail conservative management.
*
Achilles Xanthomas:
Though rare, these cholesterol deposits within the tendon can cause pain, rupture, and functional impairment, often requiring surgical excision, particularly in cases of familial hypercholesterolemia.
*
Recalcitrant Peritendinitis:
Persistent inflammation and thickening of the paratenon causing pain and restricted tendon gliding despite conservative management.
Contraindications
General contraindications for Achilles tendon surgery include:
*
Active Local or Systemic Infection:
Increases the risk of surgical site infection and potential complications.
*
Uncontrolled Systemic Comorbidities:
Such as diabetes mellitus, peripheral vascular disease, or immunosuppression, which can impair wound healing and increase surgical risks.
*
Poor Skin Quality:
Compromised skin integrity in the surgical area, which may increase the risk of wound complications.
*
Unrealistic Patient Expectations:
Crucial to manage patient expectations regarding recovery time, potential for residual symptoms, and return to prior activity levels.
*
Lack of Patient Compliance:
Post-operative rehabilitation is rigorous and prolonged; non-compliance can jeopardize surgical outcomes.
The decision to proceed with surgery requires careful patient selection, thorough counseling, and consideration of individual risk factors and functional goals.
| Indication Type | Non-Operative Management | Operative Management |
|---|---|---|
| Primary AT (NIAT/IAT) | Initial presentation, mild-moderate pain, < 6-12 months duration, no significant structural abnormalities. Eccentric loading is paramount. | Failed structured conservative management (> 6-12 months), severe and persistent pain, significant functional impairment. |
| Insertional AT | Initial presentation, mild pain, no significant Haglund's deformity or large calcaneal spurs. Focus on activity modification, heel lifts, and gentle eccentric loading. | Chronic pain with significant Haglund's deformity, large calcaneal spurring, retrocalcaneal bursitis, and tendinosis refractory to conservative care. |
| Non-Insertional AT | Initial presentation, diffuse tendinosis, palpable but small nodule, pain localized to mid-portion. Core treatment is Alfredson-type eccentric heel drop protocol. | Large painful nodule or segment of tendinosis affecting >50% of tendon cross-section, persistent symptoms despite comprehensive non-op therapy. |
| Partial Rupture | Small tear (< 25-30% of cross-section), stable, low functional demand, compliant patient willing to undergo prolonged immobilization/rehab. | Larger tears (>30-50%), persistent pain/dysfunction despite non-op, active individuals with high functional demands, or failed conservative management. |
| Other Pathologies | - | Achilles xanthomas, recalcitrant peritendinitis with adhesions, chronic painful plantaris tendon impingement. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to optimize outcomes and minimize complications in Achilles tendon surgery. This involves a comprehensive patient assessment and detailed surgical strategy.
Pre-Operative Planning
-
Patient History and Physical Examination:
- Thorough review of the patient's symptoms, duration, prior treatments, and functional limitations.
- Assessment of pain location, palpation of the Achilles tendon for nodules, thickening, or defects.
- Evaluation of ankle range of motion, strength of plantarflexion, and integrity of the Achilles tendon (Thompson test if partial rupture is suspected).
- Assessment for Haglund's deformity or other bony prominences in cases of insertional tendinopathy.
- Neurovascular examination, paying particular attention to the sural nerve distribution.
-
Imaging Studies:
- Plain Radiographs: Lateral weight-bearing views of the ankle and foot are crucial to assess for Haglund's deformity, calcaneal spurs, enthesophytes, or calcification within the Achilles tendon.
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating tendon integrity, extent of degenerative changes, presence of nodules, retrocalcaneal bursitis, and occult partial ruptures. It provides detailed information on tendon architecture and soft tissue involvement.
- Ultrasound: A dynamic, cost-effective tool to assess tendon morphology, neovascularization (Power Doppler), and guide percutaneous interventions, though it is operator-dependent.
-
Medical Optimization:
- Evaluate and optimize any underlying medical conditions (e.g., diabetes, cardiovascular disease) that could impact surgical risk or wound healing.
- Discuss smoking cessation, as nicotine significantly impairs tissue healing.
- Review all medications, especially anticoagulants, which may need to be bridged or discontinued perioperatively.
- Informed Consent: Detailed discussion with the patient regarding the proposed procedure, potential benefits, risks (e.g., infection, wound dehiscence, sural nerve injury, re-rupture, persistent pain), alternative treatments, and expected post-operative course and rehabilitation.
- DVT Prophylaxis: Develop a plan for deep vein thrombosis (DVT) prophylaxis, which may include chemical (e.g., low-molecular-weight heparin) and/or mechanical (e.g., pneumatic compression devices) measures, especially given the prone position and likely prolonged immobilization.
Patient Positioning
The most common and preferred position for Achilles tendon surgery is
prone
.
1.
Preparation:
The patient is carefully turned prone onto the operating table. Care must be taken to pad all pressure points (e.g., knees, shins, forehead, chest, iliac crests) to prevent nerve compression or skin breakdown.
2.
Lower Extremity Access:
The affected lower extremity is prepped and draped to allow full access to the posterior ankle and distal calf.
3.
Ankle Positioning:
A soft bolster or specialized ankle support is placed under the distal tibia/proximal foot to maintain the ankle in approximately 10-20 degrees of plantarflexion. This relaxes the gastrocnemius-soleus complex, facilitating tendon exposure and reducing tension during repair. It also helps to prevent excessive pressure on the anterior ankle.
4.
Tourniquet Placement:
A pneumatic tourniquet is typically applied high on the ipsilateral thigh to achieve a bloodless field, crucial for precise dissection and identification of pathology.
5.
Surgical Prep and Drape:
Standard sterile prep extends from the mid-calf down to the toes. Draping ensures a wide sterile field, allowing for potential extension of the incision or harvesting of grafts if necessary.
Detailed Surgical Approach / Technique
Surgical intervention for Achilles tendinopathy varies based on the specific pathology (non-insertional vs. insertional) and the extent of tendon involvement. The goal is consistent: debridement of degenerative tissue and restoration of healthy tendon structure and function, either directly or through augmentation.
Non-Insertional Achilles Tendinopathy (Mid-portion)
For chronic, symptomatic NIAT refractory to conservative care, the primary surgical approach involves open debridement of the degenerative tissue.
- Incision: A longitudinal incision is typically made along the medial or lateral border of the Achilles tendon, centered over the palpable nodule or area of maximal tenderness. A lateral incision is often preferred to minimize the risk of sural nerve injury (which runs posterolaterally), although a medial incision avoids the sural nerve entirely. Some surgeons advocate a central incision directly over the tendon. The length of the incision is dictated by the extent of the pathology, usually 5-10 cm.
-
Dissection:
- Skin and Subcutaneous Tissue: Careful dissection is performed through the skin and subcutaneous layers. Identify and protect the sural nerve if using a lateral incision. The nerve typically crosses the lateral aspect of the tendon approximately 10-15 cm proximal to the calcaneal insertion.
- Paratenon: The paratenon is identified. It may be thickened and adherent in chronic cases. A longitudinal incision is made through the paratenon, preserving as much as possible, as it contributes to tendon vascularity.
-
Tendon Exploration and Debridement:
- The Achilles tendon is exposed. Degenerative areas appear yellowish, soft, swollen, and disorganized, contrasting with the glistening white appearance of healthy tendon.
- A longitudinal incision may be made into the affected tendon substance to fully expose the pathology.
- Core Debridement: The diseased, mucoid, and disorganized tendon tissue is meticulously excised using a scalpel. The extent of debridement is crucial: sufficient removal of pathological tissue while preserving as much healthy tendon as possible. Longitudinal tenotomies may be performed to release tension and allow for remodeling.
- Curettage: The central core of the tendon may be curetted.
- Neovascularization: Any visible neovessels, particularly those with associated nerve fibers, are cauterized or ligated.
-
Augmentation (if needed):
- If a significant portion (>50%) of the tendon is debrided, or if there is concern for tendon integrity post-debridement, augmentation may be necessary.
- Flexor Hallucis Longus (FHL) Tendon Transfer: This is the most common technique. The FHL tendon is harvested through a separate small incision on the medial aspect of the foot, released from its muscle belly, and then passed proximally into the Achilles tendon. It is then woven into the Achilles tendon (using a Pulvertaft weave or similar technique) to reinforce the weakened segment. The FHL is an ideal donor due to its similar biomechanical properties, synergistic function, and minimal donor site morbidity.
-
Closure:
- The paratenon is carefully closed with fine absorbable sutures, aiming to create a smooth gliding surface.
- Subcutaneous tissues are approximated.
- Skin is closed with non-absorbable sutures or staples.
- The ankle is typically immobilized in slight plantarflexion with a splint or cast.

Figure 2: Intraoperative view during an Achilles tendon debridement and repair, demonstrating the tendon exposure and potential areas of pathological tissue.
Insertional Achilles Tendinopathy with Haglund's Deformity
Surgical treatment for chronic IAT often involves excision of the bony prominence, debridement of the diseased tendon, and reattachment of the tendon if necessary.
-
Incision:
- Posterior Midline Incision: A common approach, but carries a higher risk of wound healing complications due to tension and potentially poor vascularity.
- Lateral Longitudinal Incision: Preferred by many surgeons to minimize wound complications and allow better access to the Haglund's deformity. It requires careful protection of the sural nerve.
- Medial Incision: Can also be used, potentially minimizing sural nerve risk but may offer less direct access to a prominent Haglund's deformity.
-
Dissection:
- Skin and Subcutaneous Tissue: Carefully incised. Sural nerve identified and protected with the lateral approach.
- Retrocalcaneal Bursa: The inflamed retrocalcaneal bursa (if present) is identified and excised.
- Tendon Release: The Achilles tendon insertion is carefully released from the calcaneus. This can be a partial release (splitting the tendon to access the underlying bone) or a complete detachment of the central and/or lateral portions of the tendon. The extent depends on the pathology and size of the Haglund's deformity. The plantaris tendon, if present and symptomatic, may also be resected.
-
Bone Resection (Haglund's Excision):
- Using an osteotome, saw, or high-speed burr, the prominent posterosuperior portion of the calcaneus (Haglund's deformity) and any associated calcaneal spurs are resected. The goal is to create a flat, smooth posterior calcaneal surface and ensure adequate clearance (at least 2-3 mm) between the tendon and bone to prevent impingement.
- The bony bed is smoothed to prevent abrasion of the reattached tendon.
-
Tendon Debridement and Reattachment:
- Any degenerative tendon tissue at the insertion is debrided.
- If the tendon was completely detached, it is reattached to the calcaneus using suture anchors. Typically, 2-4 anchors are placed into the posterior calcaneus. Strong non-absorbable sutures are passed through the tendon and securely tied down, reapproximating the tendon to its anatomical insertion site. The ankle is held in approximately 10-20 degrees of plantarflexion during reattachment to minimize tension.
- If a partial split was used, the tendon is repaired primarily.
-
Closure:
- The deep fascia, subcutaneous tissue, and skin are closed in layers.
- The ankle is immobilized in an equinus position with a splint or cast to protect the repair and minimize tension on the reattached tendon.
General Principles for Both Approaches
- Hemostasis: Maintain a bloodless field using a tourniquet.
- Aseptic Technique: Strict adherence to sterile principles.
- Gentle Tissue Handling: Minimize trauma to skin flaps and tendon substance.
- Irrigation: Copious irrigation of the wound to remove debris.
- Tourniquet Release: Release the tourniquet, achieve meticulous hemostasis.
- Post-operative Dressing: Apply a sterile dressing and appropriate immobilization.
Complications & Management
Achilles tendon surgery, while effective for recalcitrant tendinopathy, is associated with a specific set of potential complications that require vigilant post-operative monitoring and prompt management. The relatively poor vascularity of the posterior heel region, combined with the high mechanical stresses on the Achilles tendon, contributes to the incidence of these issues.
| Complication | Incidence (Approx.) | Management Strategy |
|---|---|---|
| Wound Dehiscence/Necrosis | 5-15% | Strict wound care, negative pressure wound therapy (NPWT). If full dehiscence, surgical debridement and delayed primary closure, skin grafting, or rotational flap coverage (e.g., local fasciocutaneous flaps, free flap). Aggressive infection control if present. |
| Infection (Superficial/Deep) | 1-5% | Superficial: Oral antibiotics, local wound care. Deep: Surgical irrigation and debridement, IV antibiotics based on culture sensitivities. May require hardware removal if anchors are involved. |
| Sural Nerve Injury | 2-10% (more common with lateral approach) | Neuropraxia: Observation, expectant management, gabapentin/pregabalin for neuropathic pain. Axonotmesis/Neurotmesis: Surgical exploration, neurolysis or primary repair, nerve grafting if a significant gap. |
| Tendon Re-rupture | 0-5% (higher with extensive debridement or early mobilization) | Surgical revision: direct repair if possible, augmentation with FHL or plantaris transfer, synthetic graft, or allograft for larger defects. Requires prolonged immobilization and slow rehabilitation. |
| Residual Pain/Stiffness | Common (10-30%) | Intensive physical therapy (including eccentric loading), NSAIDs, modalities. Address underlying issues like adhesions, inadequate debridement, or persistent impingement. Steroid injections are generally avoided due to rupture risk. |
| DVT/Pulmonary Embolism | <1% (with prophylaxis) | Anticoagulation (LMWH, oral agents). IVC filter for recurrent PE or contraindication to anticoagulation. Aggressive DVT prophylaxis is crucial. |
| Adhesions/Peritendinous Scarring | Variable | Aggressive, early range-of-motion exercises, physical therapy to promote tendon gliding. Surgical tenolysis may be considered for severe cases refractory to conservative management. |
| Hardware Irritation | 1-2% | Removal of suture anchors or prominent screws after adequate healing, usually 6-12 months post-operatively. |
| Complex Regional Pain Syndrome (CRPS) | Rare (<1%) | Multidisciplinary approach: physical therapy, pain management (nerve blocks, neuromodulators), psychological support, medications (NSAIDs, gabapentinoids, calcitonin). |
Management Principles
- Prevention: Meticulous surgical technique, careful soft tissue handling, adequate debridement, appropriate reattachment, and strict post-operative protocols are crucial for minimizing complications. Prophylactic antibiotics and DVT prophylaxis are standard.
- Early Recognition: High index of suspicion for developing complications based on clinical signs (e.g., fever, increasing pain, wound erythema, swelling, numbness).
- Aggressive Management: Prompt and decisive intervention is essential. This may involve further surgical procedures (e.g., debridement, re-repair, flap coverage), targeted medical therapies, and intensive rehabilitation.
- Patient Education: Comprehensive education pre- and post-operatively regarding potential complications and the importance of adhering to rehabilitation protocols.
Wound complications remain a significant challenge due to the tenuous vascularity of the posterior heel and the high-tension environment. Patients with risk factors such as diabetes, obesity, smoking, and previous corticosteroid use require particular caution and often benefit from specific wound care strategies.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following Achilles tendon surgery is a critical determinant of functional outcome and requires a structured, progressive approach. Protocols vary slightly depending on the extent of surgical intervention (e.g., debridement only vs. FHL transfer vs. reattachment for IAT) and surgeon preference, but generally follow phases of protection, controlled motion, progressive strengthening, and return to activity. The goal is to gradually restore tendon integrity, strength, and elasticity while minimizing the risk of re-injury.
General Principles
- Gradual Progression: Avoid aggressive advancements, respecting tissue healing timelines.
- Pain-Guided: Progression should be pain-free or with minimal discomfort.
- Individualized: Adjust protocol based on patient's response, co-morbidities, and functional goals.
- Multidisciplinary: Involve physical therapists, orthotists, and possibly athletic trainers.
Phases of Rehabilitation
Phase 1: Immobilization and Early Protection (0-2/4 weeks post-op)
- Goal: Protect surgical repair, minimize swelling and pain, allow initial tissue healing.
-
Immobilization:
- Immediately post-op: Posterior splint or short leg cast with the ankle in 10-20 degrees of plantarflexion.
- For IAT with reattachment or FHL transfer, immobilization is typically longer (3-4 weeks). For debridement-only procedures, it might be shorter (1-2 weeks).
- Weight-Bearing: Non-weight-bearing (NWB) with crutches for the entire immobilization period.
-
Exercises:
- Toe wiggles, quadriceps, gluteal, and core strengthening.
- Upper body conditioning.
- Ipsilateral hip strengthening (abduction, extension).
- Wound Care: Monitor incision, manage dressings.
- DVT Prophylaxis: Continue as prescribed.
Phase 2: Controlled Motion and Gradual Weight-Bearing (2/4 - 6/8 weeks post-op)
- Goal: Restore controlled ankle range of motion, initiate partial weight-bearing.
- Immobilization: Transition from cast/splint to a controlled ankle motion (CAM) boot or removable walker boot.
-
Weight-Bearing:
- Progress from NWB to partial weight-bearing (PWB) in the CAM boot, gradually increasing load over several weeks.
- Progress to full weight-bearing (FWB) in the boot as tolerated, typically by 6-8 weeks for most procedures.
-
Range of Motion (ROM):
- Begin gentle active and passive ankle dorsiflexion within pain-free limits. Avoid forced or aggressive dorsiflexion, especially if the tendon was reattached or augmented.
- Progressive decrease in plantarflexion angle of the CAM boot (e.g., by 10-degree increments weekly).
-
Exercises:
- Non-weight-bearing ankle ROM (plantarflexion, inversion, eversion).
- Isometric plantarflexion in the boot.
- Stationary cycling with minimal resistance (boot on).
- Aquatic therapy (when wounds are fully healed).
Phase 3: Progressive Strengthening and Proprioception (6/8 - 12/16 weeks post-op)
- Goal: Restore strength, balance, and proprioception.
- Immobilization: Discontinue CAM boot, transition to supportive shoes with heel lift (initially) as needed.
- Weight-Bearing: FWB without restrictions (except high-impact activities).
-
Strengthening:
- Eccentric Calf Strengthening: This is the cornerstone. Start with bilateral heel raises, progress to unilateral heel raises, then unilateral heel drops (eccentric phase emphasis) from a step. Gradual increase in repetitions, sets, and eventually resistance (e.g., backpack weight). Adhere to a prescribed protocol (e.g., Alfredson protocol principles).
- Concentric calf strengthening.
- Theraband resistance exercises for ankle dorsiflexion, inversion, eversion.
- Progressive resistance exercises for the entire lower extremity.
-
Proprioception/Balance:
- Single-leg standing, balance board, unstable surfaces.
- Walking forwards, backwards, sideways.
- Cardiovascular: Continue low-impact activities (cycling, swimming, elliptical).
Phase 4: Return to Activity / Sport-Specific Training (12/16 weeks - 6+ months post-op)
- Goal: Achieve full functional return, safe return to sport/work.
- Criteria for Advancement: Full pain-free ROM, symmetrical strength (>80-90% of contralateral limb), good balance, successful completion of prior phase activities.
-
Progressive Loading:
- Plyometric exercises (low-level jumping, hopping).
- Agility drills (shuttle runs, figure-eights).
- Sport-specific drills, gradually increasing intensity and duration.
- Return to running program: gradual progression from walking to jogging to running, with close monitoring of symptoms.
- Emphasis on Eccentrics: Continue regular eccentric calf strengthening exercises for long-term tendon health and injury prevention.
- Full Return to Sport: Typically 6-12 months post-op, or even longer for complex reconstructions (e.g., FHL transfer). This decision is based on clinical criteria, functional testing, and patient confidence, not solely on time.
Throughout all phases, vigilant monitoring for pain, swelling, and signs of re-injury is paramount. Patient education on activity modification and avoidance of sudden, high-impact activities is crucial to prevent recurrence.
Summary of Key Literature / Guidelines
The management of Achilles tendinopathy has evolved considerably, with a robust body of literature guiding current practice. A consensus has largely formed around conservative management as the initial approach, with eccentric loading protocols consistently demonstrating superior efficacy.
Conservative Management: The Role of Eccentric Loading
- Alfredson Protocol: The seminal work by Alfredson et al. (1998, 2000) established the efficacy of heavy-load, slow eccentric calf muscle training for chronic non-insertional Achilles tendinopathy. Their protocol involves 3 sets of 15 repetitions, twice daily, 7 days a week for 12 weeks, performed with both a straight knee (gastrocnemius) and a bent knee (soleus) on a step to allow for pain-free dorsiflexion. This protocol has been widely adopted and validated.
- Mechanism of Action: While the precise biological mechanism remains debated, theories include promotion of collagen cross-linkage and alignment, reduction of neovascularization and associated neoinnervation, and adaptation of the muscle-tendon unit to tensile load. Histological studies suggest a reduction in collagen disorganization.
- Efficacy: Multiple systematic reviews and meta-analyses (e.g., by Stevens and Tan, 2014; Malliaropoulos et al., 2013) have consistently demonstrated that eccentric exercise programs are effective in reducing pain and improving function in both insertional and non-insertional AT.
- Variations: While Alfredson's protocol is well-known, variations exist regarding load, speed, and frequency. Some research suggests high-load, slow-speed training may be particularly beneficial.
-
Other Conservative Modalities:
- NSAIDs: May provide short-term pain relief but do not address underlying pathology.
- Physical Therapy: Beyond eccentrics, includes manual therapy, stretching (though caution with aggressive stretching for IAT), and strengthening of proximal kinetic chain.
- Orthotics/Heel Lifts: Can reduce tension on the Achilles tendon, particularly beneficial for IAT.
- Topical Nitroglycerin Patches: Some evidence for pain reduction, thought to stimulate collagen synthesis and nitric oxide-mediated vasodilation.
-
Injections:
- Corticosteroid Injections: Generally contraindicated directly into the Achilles tendon due to a significant risk of tendon rupture and limited long-term efficacy. May be considered for retrocalcaneal bursitis external to the tendon.
- Platelet-Rich Plasma (PRP): Evidence for PRP in AT is mixed and generally not superior to eccentric exercise alone, with some studies showing no benefit or only short-term modest improvements. Not currently considered a first-line treatment.
- Dry Needling/Prolotherapy: Limited, inconclusive evidence.
Surgical Management: Outcomes and Indications
- Indications: As discussed, surgery is reserved for chronic, debilitating AT refractory to a minimum of 6-12 months of high-quality conservative management.
-
Surgical Outcomes:
- Non-Insertional AT Debridement: Studies generally report good to excellent outcomes in 70-90% of patients, with significant pain relief and functional improvement. FHL transfer for extensive debridement yields similar success rates, with minimal donor site morbidity.
- Insertional AT with Haglund's Resection and Tendon Reattachment: Success rates are comparable, ranging from 75-90%. However, wound healing complications, re-rupture, and prolonged recovery are more common with insertional procedures, especially those requiring significant tendon detachment and reattachment.
- Current Guidelines: Major orthopedic societies (e.g., AAOS) generally endorse a conservative-first approach, emphasizing eccentric loading. Surgical intervention algorithms prioritize debridement for localized pathology and consider augmentation for significant tendon defects. The choice of surgical approach (open vs. minimally invasive) continues to be debated, with open techniques remaining the gold standard for extensive pathology.
Persistent Challenges and Future Directions
Despite advances, chronic Achilles tendinopathy remains a challenging condition. Key areas of ongoing research and clinical focus include:
*
Optimizing Eccentric Protocols:
Refining parameters (load, speed, frequency, duration) for individualized patient care.
*
Biological Augmentation:
Further investigation into the efficacy and appropriate use of biologics (e.g., advanced PRP formulations, stem cells) with more rigorous study designs.
*
Minimally Invasive Techniques:
Development and evaluation of less invasive surgical approaches to reduce morbidity, particularly for NIAT (e.g., percutaneous tenotomy, TOPAZ radiofrequency microtenotomy), though long-term data and comparative studies are still maturing.
*
Preventative Strategies:
Identifying individuals at high risk and implementing targeted prevention programs.
In conclusion, eccentric calf stretching is undeniably the bedrock of non-operative management for Achilles pain due to tendinopathy, proven by extensive literature to facilitate tendon remodeling and provide lasting relief. Surgical intervention, while effective, is a secondary option, judiciously applied to specific pathologies after exhaustive conservative efforts, demanding meticulous technique and stringent post-operative rehabilitation for optimal patient outcomes.
Clinical & Radiographic Imaging

