Ballet Dancer's Ankle: Is Total Ankle Arthroplasty the Answer?
Introduction & Epidemiology
The "ballet dancer's ankle" represents a complex clinical entity characterized by chronic pain, functional limitations, and often, progressive degeneration stemming from the unique and extreme biomechanical demands placed upon the ankle joint. Unlike the general population, ballet dancers routinely expose their ankles to supraphysiologic ranges of motion, particularly forced plantarflexion (en pointe) and repetitive impact loading. This sustained microtrauma and macrotrauma predisposes them to a specific spectrum of pathologies, including anterior and posterior impingement syndromes, osteochondral lesions of the talus (OCLs), syndesmotic instability, tendinopathies (flexor hallucis longus, posterior tibial), and eventually, post-traumatic osteoarthritis.
The prevalence of ankle pathologies among professional and pre-professional ballet dancers is remarkably high, with studies reporting symptomatic ankle pain in 75-90% of dancers during their careers. While many conditions are amenable to non-operative management or arthroscopic intervention (e.g., debridement for impingement or OCLs), a subset of dancers will progress to symptomatic, end-stage ankle osteoarthritis despite exhaustive conservative and prior operative efforts. This progression is particularly challenging in a population where preserving motion and high functional output is paramount to their profession and quality of life.
Total Ankle Arthroplasty (TAA) has emerged as a viable treatment option for end-stage ankle osteoarthritis, offering the theoretical advantage of motion preservation compared to ankle arthrodesis. However, the application of TAA in the athletic population, and specifically in ballet dancers, remains a subject of considerable debate and careful patient selection. The concerns revolve around implant survivorship, polyethylene wear, and functional outcomes in the face of extreme joint loading and range of motion requirements. This review aims to provide a comprehensive, academic perspective on the role of TAA in the management of end-stage ankle osteoarthritis in the ballet dancer, focusing on critical surgical considerations, outcomes, and rehabilitation.
Surgical Anatomy & Biomechanics
A profound understanding of the ankle's intricate anatomy and unique biomechanics is fundamental to addressing pathologies in ballet dancers and for successful TAA.
Osseous Anatomy
The ankle joint is a hinge-type synovial joint primarily formed by the articulation of the distal tibia, distal fibula, and the talus.
*
Tibia:
The distal tibia forms the tibial plafond superiorly and the medial malleolus medially. The anterior and posterior margins of the plafond are critical for impingement syndromes.
*
Fibula:
The lateral malleolus of the fibula forms the lateral wall of the ankle mortise. Its precise length and rotational alignment are crucial for ankle stability.
*
Talus:
The talus is a unique bone, devoid of muscular attachments, relying entirely on ligaments and tendons for its blood supply and stability. Its dome-shaped trochlea articulates with the tibial plafond. The talar neck is particularly vulnerable to stress fractures in dancers. The anterior and posterior aspects of the talus, when hyperplantarflexed or hyperdorsiflexed, are primary sites for impingement. The specific shape of the talus (wider anteriorly than posteriorly) contributes to the inherent stability of the joint in dorsiflexion, becoming less congruent in plantarflexion.
Ligamentous Anatomy
The stability of the ankle joint is heavily reliant on its robust ligamentous structures:
*
Lateral Collateral Ligaments:
The anterior talofibular ligament (ATFL), calcaneofibular ligament (CFL), and posterior talofibular ligament (PTFL) resist inversion and provide anteroposterior stability. Chronic ankle sprains, common in dancers, can lead to insufficiency and instability.
*
Medial (Deltoid) Ligament:
A broad, strong ligament composed of superficial (tibiocalcaneal, tibionavicular, posterior tibiotalar) and deep (anterior tibiotalar, posterior tibiotalar) layers. It resists eversion and external rotation.
*
Syndesmotic Ligaments:
The anterior inferior tibiofibular ligament (AITFL), posterior inferior tibiofibular ligament (PITFL), and interosseous membrane maintain the integrity of the distal tibiofibular syndesmosis, forming the ankle mortise. Injuries to these ligaments, often seen with rotational trauma, can lead to chronic instability and subsequent post-traumatic arthritis.
Tendon Anatomy
Multiple tendons cross the ankle joint, contributing to motion and stability. Of particular relevance in ballet:
*
Flexor Hallucis Longus (FHL):
Passes through a fibro-osseous tunnel posterior to the talus. Hyperplantarflexion can lead to FHL tendinopathy or impingement (dancer's tendinitis).
*
Achilles Tendon:
The strongest tendon in the body, vital for plantarflexion. Chronic pain or pathology here can significantly impact a dancer's career.
*
Posterior Tibial Tendon:
Supports the medial arch and plantarflexion.
*
Peroneal Tendons (Longus and Brevis):
Essential for eversion and lateral stability.
Biomechanics of the Ballet Dancer's Ankle
The unique biomechanical demands of ballet include:
*
Hyperplantarflexion (Pointe):
In the
en pointe
position, the dancer's body weight is transmitted through the very distal aspects of the tibia and talus, placing immense pressure on the anterior ankle joint and stretching the posterior structures. The range of plantarflexion required often exceeds 90 degrees relative to the tibia. This extreme position frequently causes posterior impingement (os trigonum syndrome, posterior capsulitis, FHL tendinopathy) and can lead to OCLs of the posterior talus.
*
Dorsiflexion (Plié):
The
plié
(deep knee bend) requires significant dorsiflexion, which can lead to anterior impingement (osteophyte formation, synovitis).
*
Repetitive Microtrauma:
Jumps, landings, and turns subject the ankle cartilage to high-impact and torsional forces. This repetitive loading, compounded by any underlying malalignment or instability, accelerates cartilage wear and eventually leads to osteoarthritis.
*
Ligamentous Laxity:
While some dancers exhibit generalized hypermobility, chronic repetitive sprains can lead to specific ligamentous laxity, compromising joint stability and leading to abnormal kinematics, further contributing to degenerative changes.
*
Subtalar Joint:
Though separate, the subtalar joint (talocalcaneal) motion is critical for ankle function, particularly for uneven surfaces and shock absorption. Altered subtalar mechanics due to long-standing ankle pathology can influence TAA outcomes.
Understanding these specific anatomical and biomechanical stresses is paramount when considering TAA for a ballet dancer. The ideal TAA implant must accommodate and withstand these unique forces while preserving the necessary range of motion, particularly in plantarflexion, without causing impingement or accelerated wear.

Indications & Contraindications
The decision to proceed with Total Ankle Arthroplasty in any patient, particularly a high-demand individual like a ballet dancer, requires rigorous assessment of indications and contraindications. The goal is to alleviate pain, improve function, and maintain motion where possible.
Indications for Total Ankle Arthroplasty (TAA)
- End-Stage Ankle Osteoarthritis: This is the primary indication, typically identified by clinical symptoms (pain, swelling, stiffness, functional limitation) and radiographic evidence (joint space narrowing, osteophytes, subchondral sclerosis, cyst formation). In ballet dancers, this often stems from chronic impingement, osteochondral lesions, or recurrent instability leading to post-traumatic arthritis.
- Failed Comprehensive Non-Operative Management: A prerequisite for TAA, encompassing activity modification, physical therapy, bracing/orthoses, NSAIDs, and intra-articular injections (corticosteroid, hyaluronic acid, PRP).
- Preservation of Motion Desired: For ballet dancers, maintaining ankle motion is crucial for their profession. TAA offers this advantage over arthrodesis, which would invariably end a dancer's performing career.
- Age (Relative): While traditionally considered for older, low-demand patients, modern TAA implants and techniques have expanded indications to younger, active individuals. However, long-term survivorship data in very young, high-demand patients like professional dancers is still evolving, necessitating careful discussion about revision burden.
- Adequate Bone Stock: Sufficient bone quality in the distal tibia and talus to support implant fixation. Significant osteonecrosis or large cysts may require augmentation or preclude TAA.
- Acceptable Ankle Alignment: While some mild to moderate coronal plane deformity (varus/valgus <15-20 degrees) can be corrected with TAA, severe deformity may require concomitant osteotomies or render TAA unsuitable. Sagittal plane malalignment (e.g., severe pes planus or cavus) also needs consideration.
- Intact Soft Tissue Envelope: A healthy, pliable soft tissue envelope without significant scarring, chronic ulcers, or active infection is essential for wound healing and prosthesis protection.
- Patient Motivation and Realistic Expectations: The patient must be fully informed about the potential benefits, risks, and the rigorous rehabilitation protocol, understanding that full return to professional ballet at the previous level may not be achievable.
Contraindications for Total Ankle Arthroplasty (TAA)
- Active Infection: Absolute contraindication. Any active local or systemic infection must be eradicated prior to considering TAA.
- Severe Peripheral Vascular Disease: Compromised vascular supply can lead to poor wound healing and increase the risk of infection and limb loss.
- Charcot Arthropathy: Neuropathic destruction of the joint, leading to bone instability and poor implant fixation.
- Severe Osteonecrosis of the Talus: Extensive collapse or fragmentation of the talus may not provide adequate support for the talar component, leading to early failure.
- Significant Neurological Deficit: Uncontrolled spasticity or paralysis can lead to uncontrolled stresses on the implant and poor outcomes.
- Extensive Soft Tissue Defect/Compromise: Previous trauma, radiation, or chronic ulcers that compromise the soft tissue envelope over the ankle.
- Ligamentous Instability: Severe, uncorrected ankle instability (e.g., recurrent dislocations or subluxations) can lead to early polyethylene wear, implant loosening, and persistent pain. This often requires pre-emptive or concomitant ligament reconstruction.
- Skeletally Immature Patient: TAA is contraindicated in patients with open growth plates.
- Morbid Obesity: While not an absolute contraindication, significantly increased body mass index (BMI > 40 kg/m²) is associated with higher complication rates and potentially reduced implant survivorship.
- Unrealistic Patient Expectations: If a patient anticipates a complete return to professional ballet with unrestricted activity after TAA, they may be a poor candidate due to potential disappointment and non-adherence to activity restrictions.
Operative vs. Non-Operative Indications in End-Stage Ankle Osteoarthritis
The following table summarizes the general decision-making pathway for end-stage ankle osteoarthritis in a high-demand patient, such as a ballet dancer.
| Category | Non-Operative Management | Operative Management (TAA or Arthrodesis) |
|---|---|---|
| Pain | Mild to moderate, intermittent, manageable with conservative measures | Severe, chronic, debilitating, refractory to comprehensive non-operative treatment |
| Functional Status | Able to modify activities, maintain reasonable function | Significant limitation in activities of daily living, inability to perform work/dance |
| Radiographic OA | Early to moderate joint space narrowing, minimal osteophytes | End-stage joint space narrowing, subchondral sclerosis, cysts, osteophytes, significant deformity |
| Joint Motion | Reasonable motion, mild stiffness | Markedly decreased, painful range of motion |
| Patient Demands | Lower demand, willing to accept activity modifications | High demand (e.g., professional ballet dancer) desiring motion preservation; unwilling to accept fusion |
| Comorbidities | Uncontrolled systemic diseases, active infection, severe vascular disease | Optimized health status, controlled comorbidities |
| Bone Stock/Integrity | Good bone stock, no significant osteonecrosis | Adequate bone stock, minimal osteonecrosis |
| Soft Tissues | Healthy, pliable | Healthy, pliable (if compromised, may require soft tissue reconstruction prior to or with TAA) |
| Ligamentous Stability | Stable ankle joint | Stable ankle joint, or instability correctable with concomitant procedures |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for achieving optimal outcomes in TAA, particularly in a complex case involving a high-demand individual like a ballet dancer.
Pre-Operative Planning
-
Detailed History and Physical Examination:
- History: Focus on the onset, duration, character, and location of pain. Elicit specific aggravating and relieving factors. Quantify functional limitations, specifically regarding ballet-related activities (e.g., ability to perform plié , relevé , en pointe , jump). Document prior injuries, surgeries, and conservative treatments. Assess general health status and comorbidities.
- Physical Exam: Observe gait. Evaluate skin condition, neurovascular status, and identify any signs of infection. Assess ankle and subtalar joint range of motion (active and passive), noting pain at extremes. Evaluate stability (anterior drawer, talar tilt, stress radiography if indicated). Palpate for osteophytes, effusion, and tenderness. Assess muscle strength, particularly plantarflexors and dorsiflexors. Crucially, assess the hindfoot alignment in weight-bearing.
-
Radiographic Evaluation:
- Standard Weight-Bearing Radiographs: Anteroposterior (AP), lateral, and mortise views are essential. These allow assessment of joint space narrowing, osteophyte formation, subchondral sclerosis, cyst formation, and overall limb alignment (tibial-talar angle, tibiocalcaneal angle). Crucial for templating implant size.
- Long-Leg Standing Radiographs: Recommended to assess overall lower limb mechanical axis and identify any proximal deformities (e.g., genu varum/valgum) that may influence ankle alignment and TAA success. Corrective osteotomies may be required.
- CT Scan: Provides detailed information on bone morphology, osteophyte burden, cystic lesions, and bone stock. Critical for assessing axial rotation, articular surface integrity, and identifying any talar avascular necrosis. It aids in preoperative templating and identifying potential challenges for bone cuts.
- MRI Scan: Useful for assessing soft tissue pathology (tendinopathy, synovitis), ligamentous integrity, and cartilage quality in cases where there is doubt. It can also help evaluate the extent of osteochondral lesions or talar necrosis.
-
Implant Selection and Templating:
- Review various TAA systems available, considering their design principles (fixed vs. mobile bearing, cemented vs. cementless, specific instrumentation). Most modern TAA systems are three-component, mobile-bearing designs with cementless fixation.
- Utilize templating software or physical templates with radiographic images to estimate appropriate implant size for both tibial and talar components. Consider the anticipated resected bone stock and the need for coverage.
- Plan for any concomitant procedures, such as osteophyte resection (anterior or posterior), ligamentous reconstruction, gastrocnemius recession, or hindfoot osteotomies (e.g., calcaneal osteotomy) to optimize alignment and soft tissue balance.
-
Patient Counseling:
- Thorough discussion of the surgical procedure, potential benefits (pain relief, motion preservation), and risks (infection, loosening, fracture, nerve injury, continued pain).
- Emphasize the unique challenges in a ballet dancer and set realistic expectations regarding functional return, particularly professional dancing. It is crucial to manage expectations regarding the intensity and type of activities possible post-TAA. A full return to en pointe work at the pre-injury level is rarely guaranteed and often not advisable for long-term implant survivorship.
- Review the anticipated post-operative rehabilitation protocol, commitment required, and potential need for revision surgery in the future.
Patient Positioning
- Supine Position: The patient is typically positioned supine on a radiolucent operating table.
- Limb Preparation: A thigh tourniquet is applied for a bloodless field, typically inflated after exsanguination. The entire lower limb is prepped and draped from the mid-thigh to the toes, allowing for full range of motion of the ankle and foot during the procedure.
- Foot Placement: The ipsilateral hip is usually slightly flexed and externally rotated to allow the foot to rest in a neutral position, or a bolster may be placed under the ipsilateral hip to facilitate positioning. Some surgeons prefer to position the foot off the end of the table to allow for easier access and full ankle excursion, using an ankle distractor or assistant for distraction.
- Image Intensifier: The C-arm image intensifier is positioned to allow for clear intraoperative AP and lateral views of the ankle joint. This is indispensable for confirming guide wire placement, bone cuts, and implant alignment.
- Operating Surgeon and Assistant Positioning: The primary surgeon typically stands on the medial side of the limb, while the assistant is positioned laterally, or vice-versa depending on the chosen approach and surgeon preference.
Detailed Surgical Approach / Technique
The standard approach for most modern Total Ankle Arthroplasty systems is anterior. This approach provides excellent visualization of the ankle joint and allows for precise bone cuts and soft tissue balancing. The following outlines a generalized technique, recognizing that specific implant systems may have proprietary instrumentation and nuances.
General Principles
- Asepsis: Strict sterile technique is paramount to minimize the risk of periprosthetic infection.
- Tourniquet Control: A pneumatic thigh tourniquet is used throughout the critical phases of bone resection and implant insertion to maintain a bloodless field, ensuring precise cuts and optimal visualization.
- Soft Tissue Protection: Meticulous dissection and careful retraction are crucial to protect neurovascular structures and preserve the soft tissue envelope for wound healing.
- Alignment: Achieving optimal mechanical alignment in coronal, sagittal, and axial planes is critical for implant longevity and functional outcome.
- Soft Tissue Balancing: Balanced tension of collateral ligaments and capsule throughout the range of motion is essential for stability and proper kinematics.
Surgical Steps (Anterior Approach)
-
Incision:
- A longitudinal skin incision, approximately 12-15 cm in length, is made over the anterior aspect of the ankle. It typically runs from just distal to the anterior margin of the tibia proximally, across the ankle joint, and distally towards the navicular or medial cuneiform.
- The incision can be centered slightly medially (anteromedial approach) or centrally, depending on surgeon preference and the specific TAA system. An anteromedial approach typically minimizes potential injury to the superficial peroneal nerve branches laterally and the dorsalis pedis artery centrally.
-
Dissection and Internervous Plane:
- Skin and Subcutaneous Tissue: Incision through skin and subcutaneous fat. Meticulous hemostasis.
-
Neurovascular Protection:
Identify and protect the neurovascular structures.
- The superficial peroneal nerve typically runs laterally within the subcutaneous tissue and can be protected by careful blunt dissection and retraction.
- The saphenous nerve and vein lie more medially.
- The dorsalis pedis artery , often accompanied by the deep peroneal nerve, lies centrally between the extensor hallucis longus (EHL) and extensor digitorum longus (EDL) tendons, or between the EHL and tibialis anterior (TA) tendons.
-
Retraction of Tendons:
- The tibialis anterior (TA) tendon is typically retracted medially.
- The extensor hallucis longus (EHL) tendon and extensor digitorum longus (EDL) tendons are retracted laterally, along with the deep peroneal nerve and dorsalis pedis artery complex. This creates an internervous plane.
- Careful, gentle retraction is vital to avoid tendon injury or nerve neuropraxia.
-
Capsulotomy and Exposure:
- A longitudinal arthrotomy is performed through the anterior joint capsule, exposing the tibio-talar articulation.
- Synovectomy is performed as needed to remove inflamed tissue and improve visualization.
- Any significant anterior osteophytes (e.g., "dancer's osteophytes") are resected at this stage to improve exposure and post-operative dorsiflexion.
-
Tibial Resection:
- Guide Wire Placement: An intramedullary (IM) or extramedullary (EM) guide system is employed. IM guides are generally preferred for precise alignment in the coronal and sagittal planes. An IM rod is inserted into the distal tibia, typically aiming for the center of the medullary canal.
- Tibial Cutting Jig: The tibial cutting jig is attached to the guide rod, positioning the cutting block for the desired resection level. This block dictates the amount of bone to be resected from the distal tibia. The cut must be parallel to the ground in neutral ankle position (coronal plane), with appropriate posterior slope (typically 0-5 degrees) in the sagittal plane, and perpendicular to the mechanical axis of the tibia.
- Resection: An oscillating saw is used to make the initial distal tibial cut. The anterior and posterior osteophytes are removed, and the articular cartilage is cleared.
-
Talar Resection:
- Distraction: The ankle joint is distracted to facilitate access to the talus. This can be achieved with a specific ankle distractor or manually by an assistant.
- Guide Wire Placement: The talar cutting guide is positioned based on the desired talar component size and alignment. This often involves placing a guide pin into the neck of the talus, ensuring central placement and appropriate rotation.
- Talar Cuts: The talar cuts are made using an oscillating saw. These cuts usually involve a superior cut parallel to the tibial cut and additional cuts (e.g., medial/lateral chamfer cuts or sagittal cuts) to match the implant design. The goal is to recreate the normal talar anatomy and kinematics. Care is taken to avoid over-resection, particularly medially, which could compromise blood supply to the talus.
-
Soft Tissue Balancing:
- This is a critical step to ensure optimal implant function and longevity. Trial components are inserted.
- The ankle is taken through a full range of motion (dorsiflexion, plantarflexion, inversion, eversion) to assess mediolateral and anteroposterior stability.
- Tightness in Dorsiflexion: May indicate insufficient bone resection, anterior soft tissue impingement, or a tight posterior capsule/Achilles tendon.
- Tightness in Plantarflexion: Less common but could indicate posterior bony impingement (if osteophytes were not fully cleared) or a mismatch in component sizing.
- Mediomedial/Lateral Instability: If there is gapping on one side, a controlled release of the collateral ligament on the tighter side may be performed. For example, if there is varus instability, a medial release may be needed. If there is valgus instability, a lateral release may be necessary. This requires experience and precision. Occasionally, a gastrocnemius recession may be performed to address an equinus contracture.
-
Trial Implants and Final Checks:
- Trial tibial and talar components, along with various polyethylene inserts, are inserted.
- Assess alignment, stability, and range of motion. The polyethylene insert should sit congruently and not impinge on any surrounding structures.
- Confirm adequate joint space and soft tissue tension throughout the full range of motion. Use fluoroscopy to confirm proper alignment.
-
Definitive Implants:
- The trial components are removed.
- The bone surfaces are prepared (e.g., burr, brush) according to the implant system's specifications for cementless fixation.
- The definitive tibial component is impacted into place. Most modern systems utilize porous-coated titanium components for bone ingrowth.
- The talar component is then impacted into place.
- The chosen polyethylene insert is carefully seated between the two metal components.
- The range of motion, stability, and alignment are re-checked.

-
Closure:
- The tourniquet is deflated, and meticulous hemostasis is achieved.
- A drain may be placed, though this is surgeon-dependent.
- The anterior joint capsule is repaired.
- The subcutaneous tissues are closed in layers.
- The skin is closed using staples or sutures.
- A sterile dressing and a posterior splint (initially for immobilization in neutral position) are applied.
Special Considerations for Ballet Dancers
- Maximal Plantarflexion: The ability to achieve significant plantarflexion without impingement is crucial. This may necessitate aggressive posterior osteophyte debridement, careful talar component positioning, and ensuring adequate posterior soft tissue release. However, care must be taken not to destabilize the ankle.
- Subtalar Motion: While TAA replaces the tibiotalar joint, subtalar motion is vital for compensatory movements. The implant design and surgical technique should ideally preserve subtalar kinematics.
- Associated Pathology: Be prepared to address concomitant pathologies identified pre-operatively or intra-operatively, such as FHL tendinopathy (requiring release) or significant ligamentous laxity (requiring reconstruction).
- Realistic Expectations: Reiterate to the patient post-surgery that while motion will be preserved, the extreme demands of en pointe work may not be advisable for long-term implant survival, and a modified return to dance may be the most realistic goal.
Complications & Management
Despite advancements in implant design and surgical technique, Total Ankle Arthroplasty is a complex procedure with a potential for various complications. In a high-demand patient like a ballet dancer, these complications can be particularly challenging due to their functional expectations and the increased stress on the implant.
Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (%) | Salvage Strategy ## (continued)
Post-Operative Complications Specific to the Ballet Dancer
- Impingement: Despite extensive initial debridement, neo-osteophyte formation or capsular scarring can lead to recurrent anterior or posterior impingement, limiting the dancer's specific range of motion (e.g., en pointe or plié ).
- Polyethylene Wear/Loosening: The repetitive, high-impact forces and extreme range of motion (especially hyperplantarflexion) required for ballet could theoretically accelerate polyethylene wear or lead to earlier aseptic loosening compared to less active populations. The long-term survivorship data for TAAs in this specific demographic is limited.
- Subsidence/Periprosthetic Fracture: Increased stress across the bone-implant interface, particularly during dynamic and impact activities, might increase the risk of implant subsidence or periprosthetic fractures.
- Continued Pain/Functional Limitation: Even without gross complications, a dancer might experience persistent pain or an inability to return to their desired level of activity, leading to significant dissatisfaction. This may stem from subtle malalignment, soft tissue imbalance, or limitations inherent to the prosthesis itself.
Management of Complications:
Early identification and prompt management are crucial.
*
Infection:
Requires immediate debridement, extensive irrigation, and targeted intravenous antibiotics. Depending on the severity and chronicity, this may involve implant retention, a one-stage exchange, or a two-stage exchange with an antibiotic spacer, followed by reimplantation or definitive arthrodesis.
*
Aseptic Loosening:
Symptomatic aseptic loosening often necessitates revision arthroplasty, provided there is adequate bone stock. If not, or if repeated revisions fail, arthrodesis remains the gold standard salvage procedure.
*
Malalignment/Instability:
Minor malalignment might be managed with orthotics or bracing. Significant malalignment or instability typically requires revision surgery, potentially with realignment osteotomies or ligamentous reconstruction. If the implant is well-fixed but functionally failing, arthrodesis is a consideration.
*
Wound Complications:
Minor wound dehiscence may be managed with local wound care. More severe dehiscence or necrosis requires debridement, vacuum-assisted closure (VAC), and potentially flap coverage by a plastic surgeon.
*
Periprosthetic Fractures:
Stable, non-displaced fractures may be managed conservatively with immobilization. Displaced fractures typically require open reduction internal fixation (ORIF), potentially with revision of components if stability is compromised.
The decision for salvage in a ballet dancer must always weigh the potential for further complications against the patient's functional goals and quality of life. Ankle arthrodesis, while ending a dancer's career, can provide a reliable, pain-free platform for general mobility.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following Total Ankle Arthroplasty in a ballet dancer must be structured, progressive, and individualized, recognizing the unique functional demands while prioritizing implant integration and longevity. The protocol aims to restore motion, strength, proprioception, and ultimately, functional activity, with a cautious approach to high-impact and extreme range-of-motion activities.
Phase 1: Immediate Post-Operative Protection (Weeks 0-2)
- Goal: Protect surgical site, control pain and swelling, initiate early tissue healing.
-
Immobilization:
- Initially, a posterior splint or bulky dressing in neutral dorsiflexion/plantarflexion for 1-3 days.
- Transition to a removable controlled ankle motion (CAM) boot or similar rigid orthosis.
- Weight-Bearing: Strictly non-weight bearing (NWB) for the entire period to allow initial bone-implant integration.
-
Exercises:
- Pain & Swelling Management: Elevation, ice (cryotherapy), gentle compression.
-
Early Motion (Non-Weight Bearing):
- Gentle active and passive range of motion of the toes and midfoot to prevent stiffness.
- Isometric quadriceps and hamstring exercises.
- Upper extremity and core strengthening.
- Medications: Analgesics, anti-inflammatories, DVT prophylaxis.
- Wound Care: Daily wound checks, dressing changes as per surgeon's instructions.
Phase 2: Early Mobilization & Controlled Weight-Bearing (Weeks 2-6)
- Goal: Gradual increase in weight-bearing, controlled restoration of ankle range of motion, initiation of gentle strengthening.
-
Weight-Bearing:
- Progress from non-weight bearing to touch-down weight bearing (TDWB) to partial weight bearing (PWB) in the CAM boot, typically guided by radiographic evidence of implant stability and bone healing, and patient tolerance.
- Typically, PWB begins around 3-4 weeks, progressing to FWB by 6 weeks in the boot.
-
Exercises:
- Range of Motion: Gentle active and passive ankle dorsiflexion and plantarflexion, inversion, and eversion within pain-free limits. Focus on restoring a functional arc. Crucial for ballet dancers, but caution against aggressive end-range stretching initially.
-
Strengthening (Isometric/Low-Load Isotonic):
- Ankle isometrics (dorsiflexion, plantarflexion, inversion, eversion).
- Calf raises (seated, bilateral, limited range).
- Hip and knee strengthening.
- Gait Training: With crutches or walker, focusing on a heel-toe pattern as weight-bearing progresses.
Phase 3: Intermediate Strengthening & Proprioception (Weeks 6-12)
- Goal: Discontinue immobilization, progressive strengthening, restore proprioception, normalize gait.
-
Immobilization:
- Transition out of the CAM boot, often starting at 6-8 weeks, gradually increasing time out of the boot as tolerated. May use an ankle brace for support in the initial weeks out of the boot.
- Weight-Bearing: Full weight-bearing (FWB) out of the boot, progressing to normal gait.
-
Exercises:
-
Strengthening:
- Progressive resistance exercises for ankle musculature (TheraBand, light weights).
- Unilateral heel raises (controlled range).
- Stair climbing, step-ups.
-
Proprioception/Balance:
- Single-leg standing, balance board, wobble board (progressing from stable to unstable surfaces).
- Eyes open, then eyes closed.
- Functional Activities: Longer walks, gentle cycling (stationary bike).
-
Strengthening:
- Manual Therapy: Soft tissue mobilization to address any scar tissue, joint mobilizations to improve ankle and subtalar motion.
Phase 4: Advanced Functional & Sport-Specific Training (Months 3-6+)
- Goal: Refine strength, power, agility, and return to modified dance activities.
-
Exercises:
- Progressive Strengthening: Increase resistance and complexity of exercises. Introduce plyometrics (low-level hopping, jumping) if appropriate and with extreme caution, and only after significant strength and stability are achieved.
- Agility Drills: Ladder drills, cone drills, lateral shuffling.
-
Dance-Specific Conditioning:
- Gradual Introduction of Ballet Exercises: Begin with barre work, focusing on controlled pliés (half-bend), relevés (rise to balls of feet), and tendus (stretched movements).
- Emphasis on Core Stability and Proximal Control: Essential for proper biomechanics during dance.
- No En Pointe Work Initially: This extreme plantarflexion and weight-bearing on the forefoot places immense stress on the TAA components. A return to en pointe should be considered only after at least 6-12 months, with expert guidance, and only if deemed safe and sustainable for the implant, which is often not the case for professional en pointe performance. Many surgeons strongly advise against a return to full en pointe work.
- Modification of Jumps and Impact: High-impact jumps and landings should be severely limited or avoided.
- Monitoring: Continuous monitoring of pain, swelling, and functional progress. Radiographic follow-up to assess implant stability.
Phase 5: Return to Activity & Long-Term Management (Months 6+)
- Goal: Safe return to chosen activities, long-term implant maintenance.
- Return to Dance: A highly individualized decision made in conjunction with the surgeon, physical therapist, and dance instructor. For a professional ballet dancer, a complete return to pre-injury performance levels, especially en pointe , is highly improbable and often contraindicated for implant longevity. A modified role or a transition to teaching/choreography may be more realistic.
- Activity Restrictions: Permanent restrictions on high-impact activities (e.g., long-distance running, aggressive jumping) are generally advised to minimize polyethylene wear and reduce the risk of implant loosening or failure.
- Long-Term Follow-up: Regular clinical and radiographic follow-up is essential to monitor implant survivorship, detect early signs of wear or loosening, and address any late complications.
The rehabilitation process for a ballet dancer is often longer and more nuanced than for the general population. The goal is to maximize functional recovery while protecting the TAA from excessive forces. Clear communication about these limitations and expectations is paramount.
Summary of Key Literature / Guidelines
The landscape of Total Ankle Arthroplasty has evolved significantly over the past two decades, with modern implant designs and refined surgical techniques demonstrating improved outcomes compared to earlier generations. However, the specific application of TAA in high-demand, active individuals such as ballet dancers, where extreme ranges of motion and repetitive impact are inherent to their profession, remains a niche area with limited high-level evidence.
TAA vs. Arthrodesis
- Early Studies: Historically, ankle arthrodesis was considered the gold standard for end-stage ankle osteoarthritis, offering reliable pain relief and stability at the expense of motion. Early TAA designs had high failure rates.
- Modern Outcomes: Current literature, largely from registry data and multi-center studies, now demonstrates comparable pain relief and patient satisfaction for TAA when compared to arthrodesis. TAA's primary advantage is motion preservation, which can lead to more normalized gait patterns and potentially reduce adjacent joint degeneration (subtalar, midfoot), though this latter point is still debated.
- Long-Term Survivorship: Ten-year implant survivorship for modern TAA designs is reported to be in the range of 80-90%. However, these figures are predominantly derived from older, less active populations. Survivorship in younger, high-demand cohorts is less certain and likely lower.
TAA in Younger, Active Patients
- Evolving Indications: There is a growing trend to offer TAA to younger patients (<50-55 years old) who desire motion preservation and have adequate bone stock. The rationale is to improve quality of life and potentially defer arthrodesis.
- Challenges: The main concerns are increased polyethylene wear, higher rates of aseptic loosening, and greater revision burden in this active demographic. The longevity of current implants under continuous high-stress loading over decades is unknown.
- Patient Selection: Meticulous patient selection is paramount. Careful counseling about activity modifications and the potential for future revision surgery is essential. While TAA aims to restore function, it is generally not designed for unlimited high-impact athletic activity.
The Ballet Dancer Cohort
- Limited Data: Specific literature addressing TAA outcomes exclusively in professional ballet dancers is scarce. Most studies on TAA in athletes group various sports together, making it difficult to extrapolate specific outcomes for the unique demands of ballet.
- Anatomical Considerations: The extreme plantarflexion required for en pointe work poses a challenge for TAA design and function. Some studies suggest that TAA can achieve a functional range of motion for many daily activities, but rarely the full extent required for professional ballet.
- Functional Expectations: It is crucial for surgeons and patients to have realistic expectations. While TAA may allow a dancer to maintain a reasonable level of activity and general mobility, a full, unrestricted return to en pointe performance or high-impact choreography at pre-injury levels is typically not recommended due to the potential for accelerated implant wear, loosening, or other complications. The goal shifts from performance enhancement to pain reduction and functional maintenance within modified parameters.
- Clinical Consensus (Though not formal guidelines): Most expert consensus leans towards TAA being a viable option for a ballet dancer with end-stage arthritis who wishes to preserve motion, understanding that significant activity modification will be necessary. Arthrodesis remains a definitive option for pain relief if motion preservation is not the primary goal or if TAA fails.
Emerging Technologies & Future Directions
- Custom Implants: Patient-specific instrumentation and custom-made implants derived from 3D CT reconstructions are being developed to optimize fit and alignment, potentially improving outcomes.
- Robotic Assistance: Robotic platforms are gaining traction in TAA, offering enhanced precision for bone cuts and alignment, which may further improve implant longevity.
- Advanced Bearing Surfaces: Research continues into novel polyethylene formulations and alternative bearing surfaces to reduce wear rates.
- Biological Augmentation: The role of biologics (e.g., PRP, stem cells) in enhancing bone ingrowth and managing adjacent soft tissue pathology is being explored.
In conclusion, Total Ankle Arthroplasty offers a compelling solution for pain relief and motion preservation in select patients with end-stage ankle osteoarthritis. For the ballet dancer, the decision to undergo TAA is highly complex, weighing the desire for motion against the unique biomechanical stresses and the inherent limitations of current prosthetic technology. While TAA can effectively manage pain and provide a functional ankle for many activities, a complete return to the highest level of professional ballet, particularly en pointe , is often an unrealistic expectation. Patient selection, meticulous surgical technique, and realistic goal setting through comprehensive patient counseling remain paramount for successful outcomes in this challenging patient population.
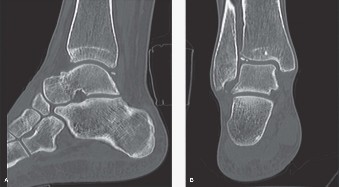
Clinical & Radiographic Imaging