Displaced Talar Neck Fracture: Optimal Treatment Revealed
Introduction & Epidemiology
Displaced talar neck fractures represent a formidable challenge in orthopedic trauma, often resulting from high-energy mechanisms such as motor vehicle accidents or falls from height. Given the talus's critical role as the keystone of the ankle and subtalar joints, connecting the leg to the foot, optimal management is paramount to preserving foot and ankle function. These fractures are characterized by a significant risk of severe complications, predominantly avascular necrosis (AVN) of the talar body and post-traumatic arthritis (PTA), largely due to the talus's unique, precarious blood supply and extensive articular cartilage coverage.
The incidence of talar fractures is relatively low, accounting for approximately 3-6% of all foot fractures and less than 1% of all body fractures. However, talar neck fractures constitute 50% of all talar fractures. They are frequently associated with other injuries, including ankle and subtalar dislocations (up to 40-50%), calcaneal fractures, pilon fractures, and ipsilateral foot or knee injuries. Open fractures are also common, particularly with higher-grade displacements.
The widely adopted Hawkins classification system, based on the degree of talar neck displacement and associated subtalar/ankle dislocations, remains a critical prognostic tool, especially regarding the risk of AVN:
*
Type I:
Nondisplaced vertical fracture of the talar neck. Low risk of AVN.
*
Type II:
Displaced fracture of the talar neck with subtalar subluxation or dislocation. Moderate (20-50%) risk of AVN.
*
Type III:
Displaced fracture of the talar neck with subtalar and ankle joint dislocation. High (70-100%) risk of AVN.
*
Type IV (Canale & Kelly modification):
Type III injury with associated talonavicular joint dislocation. Highest risk of AVN.
The goal of treatment is anatomic reduction and stable internal fixation, restoring articular congruity, and minimizing the risk of devastating long-term sequelae.
Surgical Anatomy & Biomechanics
A thorough understanding of talar anatomy, vascularity, and biomechanics is fundamental to successful management. The talus is unique among tarsal bones, having no muscular attachments, and is almost entirely covered by articular cartilage (approximately 60% of its surface). This extensive cartilage, combined with its limited intrinsic vascularity, makes it highly susceptible to chondral damage and AVN following trauma.
Key Anatomical Features:
*
Head:
Articulates with the navicular bone, forming the talonavicular joint.
*
Neck:
Connects the head to the body. This is the most common site of fracture. Its length and angulation vary, influencing screw trajectory.
*
Body:
Articulates superiorly with the tibia and fibula (ankle joint), and inferiorly with the calcaneus (subtalar joint).
*
Posterior Process:
Contains the groove for the flexor hallucis longus (FHL) tendon and medial/lateral tubercles.
*
Sinus Tarsi & Tarsal Canal:
Critical spaces containing fat, blood vessels, and ligaments, notably the cervical and interosseous talocalcaneal ligaments.
Vascular Supply:
The talus has a precarious blood supply, primarily derived from extraosseous anastomotic networks. Disruption of these vessels is directly correlated with fracture displacement and AVN risk.
*
Artery of the Tarsal Canal:
A branch of the posterior tibial artery, typically entering the tarsal canal. This is a crucial supply to the talar body.
*
Deltoid Branch:
Arises from the posterior tibial artery, supplies the medial aspect of the talar body. Often spared in non-displaced fractures, offering a potential vascular tether.
*
Dorsalis Pedis Artery branches:
Supply the superior aspect of the talar neck and head.
*
Perforating Peroneal Artery:
Contributes to the lateral aspect of the talar body.
*
Anastomotic Network:
These arteries form a retinacular plexus over the talar neck and body. High-energy injuries and significant displacement invariably disrupt these delicate networks.
Biomechanics:
The talus acts as a fulcrum, transmitting axial loads from the tibia to the foot.
*
Ankle Joint:
A hinge joint primarily allowing dorsiflexion and plantarflexion.
*
Subtalar Joint:
A complex joint allowing inversion and eversion, critical for foot adaptation to uneven surfaces.
*
Talonavicular Joint:
Part of the transverse tarsal joint (Chopart's joint), contributing to pronation/supination.
Displaced talar neck fractures disrupt the intricate alignment of these joints, altering load distribution and leading to abnormal kinematics, which predisposes to PTA. Fracture displacement is typically superiorly and medially, resulting from a combination of dorsiflexion and inversion forces, often with the foot in dorsiflexion against a fixed object.
Indications & Contraindications
Operative vs. Non-Operative Indications
The vast majority of displaced talar neck fractures (Hawkins II, III, IV) require surgical intervention to achieve anatomic reduction and stable fixation, thereby minimizing the risk of AVN, malunion, and post-traumatic arthritis.
| Indication Type | Specific Condition | Rationale / Comments |
|---|---|---|
| Operative | Hawkins Type I (rarely) | While typically non-operative, consider ORIF if a persistent gap or significant comminution is present, or if there's early collapse. |
| Hawkins Type II, III, IV | All displaced fractures, with or without associated dislocations (subtalar, ankle, talonavicular). Anatomic reduction is crucial to prevent malunion, reduce AVN risk, and minimize PTA. | |
| Open Fracture | Requires urgent irrigation and debridement, typically within 6 hours, followed by stabilization. High infection risk. | |
| Neurovascular Compromise | Immediate reduction (closed or open) is indicated to restore circulation/nerve function. | |
| Irreducible Closed Dislocation/Fracture | If closed reduction fails to achieve satisfactory alignment (often due to soft tissue interposition, e.g., tibialis posterior tendon or capsule), emergent open reduction is necessary. | |
| Significant Articular Step-off/Gap (>1-2 mm) | Even with "acceptable" overall alignment, intra-articular incongruity significantly increases the risk of PTA. | |
| Polytrauma Patient (once stabilized) | Following initial damage control and resuscitation, definitive fixation of the talar neck fracture is usually prioritized to prevent further soft tissue compromise and facilitate early mobilization. | |
| Non-Operative | Hawkins Type I (Non-displaced) | Immobilization in a short leg cast or CAM boot for 6-8 weeks, non-weight bearing, with close radiographic follow-up for displacement. |
| Medically Unstable Patient | If the patient's comorbidities or overall condition preclude safe anesthesia and surgery, temporary external fixation may be considered, followed by delayed definitive treatment once medically optimized. | |
| Severe Local Soft Tissue Compromise | Blistering, severe swelling, or impending skin necrosis may necessitate a delay in definitive ORIF, possibly with initial external fixation to allow the soft tissue envelope to recover ("wrinkle sign"). However, displaced fractures are still ultimately operative . | |
| Non-ambulatory Patient / Limited Life Expectancy | In specific circumstances where the functional demands are very low, or life expectancy is short, non-operative management might be considered to avoid surgical risks, but this is rare for displaced fractures. |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is critical to anticipating potential challenges and optimizing surgical outcomes.
Imaging:
1.
Standard Radiographs:
AP, lateral, and oblique views of the ankle and foot are essential for initial assessment. The
Canale view
(AP with foot in 15° pronation and 75° plantarflexion) is crucial for visualizing the talar neck and assessing comminution and displacement. The
Broden's view
(oblique ankle with 10-40° cephalic tilt) helps visualize the posterior subtalar facet.
2.
Computed Tomography (CT) Scan:
Mandatory for all displaced talar neck fractures. CT provides detailed information regarding:
* Fracture pattern, comminution, and articular involvement (ankle, subtalar, talonavicular joints).
* Degree and direction of displacement, impaction, and rotation.
* Presence of incarcerated fragments within joint spaces.
* Associated subtle fractures or dislocations not evident on plain radiographs.
* Planning screw trajectories and identifying potential fixation points.
3.
Magnetic Resonance Imaging (MRI):
Not typically part of acute evaluation but may be useful in later stages to assess for early AVN or significant chondral injury if symptoms persist despite good reduction.
Timing of Surgery:
The timing of surgery is controversial for closed displaced fractures but often dictated by the soft tissue envelope.
*
Urgent:
Open fractures require immediate irrigation and debridement within 6 hours to minimize infection risk. Neurovascular compromise also warrants emergent intervention.
*
Delayed:
For closed fractures with significant swelling or blistering, waiting for the "wrinkle sign" (resolution of soft tissue edema) is prudent to reduce wound complications. However, prolonged delay (>7-10 days) may lead to fracture impaction, early fibrous union, and make reduction more difficult. External fixation can be used as a temporizing measure for severely compromised soft tissues.
Patient Positioning:
*
Supine Position:
The patient is placed supine on a radiolucent operating table.
*
C-arm Access:
Essential for intraoperative fluoroscopy in multiple planes (AP, lateral, Broden's, Canale views). The C-arm should be draped and positioned to allow unobstructed views of the foot and ankle without contaminating the field.
*
Limb Preparation:
A high thigh tourniquet is applied. The limb is prepped and draped from below the knee to the toes, ensuring adequate exposure for both anteromedial and anterolateral approaches.
*
Hip Bump (Optional):
Some surgeons place a small bump under the ipsilateral hip to internally rotate the leg slightly, facilitating medial exposure.
*
Associated Injuries:
If a pilon or calcaneal fracture is present, the operating room setup needs to accommodate these as well, potentially requiring changes in C-arm angles or positioning.
Detailed Surgical Approach / Technique
Achieving anatomic reduction and stable internal fixation of a displaced talar neck fracture requires meticulous technique, often utilizing a combination of approaches.
Approaches:
-
Anteromedial Approach (Primary):
- Incision: Typically made curvilinearly, 6-8 cm long, medial to the tibialis anterior tendon, extending from the distal tibia to the talonavicular joint.
- Interval: Between the tibialis anterior tendon medially and the neurovascular bundle (dorsalis pedis artery, deep peroneal nerve) laterally.
- Structures at Risk: Saphenous nerve and vein (medially). The deltoid ligament should be preserved if possible, as it may contain a viable vascular supply to the talar body.
- Advantages: Excellent visualization of the talar neck, good access for reduction and screw placement from medial to lateral. Allows direct assessment of the talonavicular joint.
-
Anterolateral Approach (Adjunct/Secondary):
- Incision: A curvilinear incision, 6-8 cm long, centered over the talar neck, lateral to the extensor digitorum longus tendons.
- Interval: Between the extensor digitorum longus tendons medially and the peroneus tertius tendon laterally.
- Structures at Risk: Superficial peroneal nerve branches. Careful dissection is required.
- Advantages: Provides a direct view of the lateral talar neck, useful for addressing comminution or placing additional screws, particularly for a lateral-to-medial trajectory. May be needed for access to the lateral subtalar joint.
-
Posteromedial Approach (Less Common, Specific Indications):
- Incision: Posterior to the medial malleolus, along the course of the posterior tibial artery.
- Advantages: Allows access to the posterior process of the talus, useful for addressing incarcerated fragments from the posterior subtalar joint or comminution of the posterior aspect of the talar body/neck. Can also be used to address sustained comminution.
- Structures at Risk: Posterior tibial neurovascular bundle (tibial nerve, posterior tibial artery/vein, FHL tendon). Requires careful retraction.
Step-by-Step Surgical Technique:
-
Initial Reduction Maneuver:
- Often, initial closed reduction attempts can be performed under fluoroscopy to restore gross alignment and reduce soft tissue tension. This involves traction with the foot in plantarflexion and inversion.
- Once the foot is delivered into plantarflexion, the talar body is often reduced relative to the ankle mortise. The challenge then shifts to reducing the talar head/neck to the body.
- A Steinmann pin or large Schanz pin can be placed into the calcaneus for axial traction and manipulation.
- A joystick technique using a K-wire or small Schanz pin inserted into the talar head/neck fragment can aid in rotational and translational reduction.
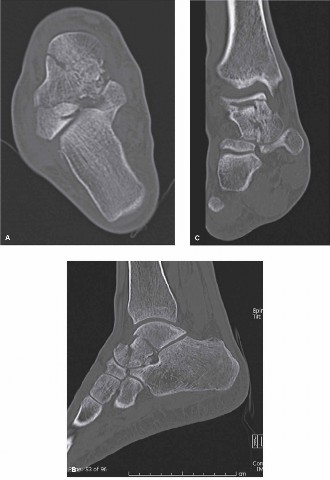
Depicts a potential complex fracture pattern that would benefit from joystick maneuvers. -
Open Reduction via Anteromedial Approach:
- Carefully dissect through subcutaneous tissue. Identify and protect the saphenous nerve and vein.
- Incision of the deep fascia exposes the tibialis anterior tendon. Retract the tendon medially.
- Capsule and periosteum are incised longitudinally over the fracture site.
- Clear the fracture hematoma and any interposed soft tissues (e.g., periosteum, capsule).
- Inspect the articular surfaces for comminution or chondral injury. Address impaction by elevating depressed fragments.
-
Fragment Reduction and Temporary Fixation:
- Restoring Length and Rotation: The primary goals are to restore the length, rotation, and alignment of the talar neck to the body.
- Direct Manipulation: Use bone hooks, periosteal elevators, or dental picks to manipulate the talar head/neck fragment into anatomic alignment with the talar body.
- Addressing Impaction: If there is impaction, a small osteotome or elevator can be used to disimpact and elevate depressed fragments, often from the plantar aspect of the neck. Bone graft (autograft or allograft) may be considered to fill metaphyseal defects, though its role in talar neck fractures is less established than in tibial plateau fractures.
- Provisional Fixation: Once anatomic reduction is achieved, maintain it with multiple small K-wires (e.g., 1.5-2.0 mm). These K-wires should be strategically placed to provide provisional stability without interfering with planned definitive screw placement. Ensure K-wires do not enter articular surfaces.
- Fluoroscopic guidance (AP, lateral, Broden's, Canale views) is used to confirm anatomic reduction in all planes. Pay close attention to the restoration of the medial and lateral columns, and the subtalar and ankle joint congruity.
-
Definitive Internal Fixation:
- Screw Selection: Typically, two to three low-profile, partially threaded (or headless compression) screws are used. Screws should be cannulated to facilitate accurate placement over K-wires.
-
Screw Trajectory:
- The most common and mechanically stable configuration involves two screws: one inserted from the anteromedial aspect of the talar neck directed posterolaterally into the talar body, and a second from the anterolateral aspect directed posteromedially. This creates a convergent, crossed-screw construct.
- Lag screw technique is preferred to maximize compression across the fracture site. This requires overdrilling the near cortex and underdrilling the far cortex. For headless compression screws, the design inherently provides compression.
- Screws should ideally be placed in the sagittal plane, parallel to the axis of motion, to avoid conflict with the ankle or subtalar joint during motion. Avoid placing screws through articular cartilage.
- Consider the unique vascular anatomy. Some surgeons advocate for screws originating from the talar body into the head/neck (retrograde) when possible, or at least avoiding excessive soft tissue stripping medially to preserve potential deltoid arterial supply.

Illustrates optimal screw placement for stable fixation.- Plate Fixation (for comminution): In cases of significant comminution, particularly in Hawkins Type III/IV fractures, a small fragment plate (e.g., 2.0 or 2.4 mm locking plate) may be considered as an adjunct to screws to provide additional stability and neutralization, especially if the bone quality is poor or screw purchase is inadequate. Plates are typically applied on the dorsal or medial aspect of the talar neck.
-
Associated Dislocations:
- Subtalar Dislocation: Often reduces with neck reduction. If persistent, direct manipulation or temporary K-wire fixation may be needed.
- Ankle Dislocation: Typically reduces as the talar body is aligned with the tibia.
- Talonavicular Dislocation: Address directly after talar neck fixation. This usually involves reducing the navicular onto the talar head and temporary K-wire fixation.
-
Final Fluoroscopic Assessment:
- Verify anatomic reduction of the talar neck and all associated joints (ankle, subtalar, talonavicular) in all views.
- Confirm adequate screw length, position, and absence of intra-articular penetration.
- Assess ankle and subtalar range of motion to ensure no mechanical block from hardware.
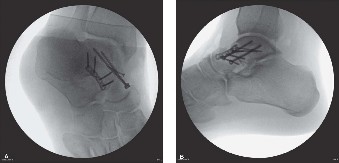
A post-operative radiograph demonstrating successful fixation of a talar neck fracture. -
Wound Closure:
- Thorough irrigation of the surgical site.
- Close the capsule/periosteum if possible, without tension.
- Layered closure of subcutaneous tissues and skin.
- Apply a sterile dressing and a well-padded splint (e.g., posterior slab with sugar tong) in a neutral position.
Complications & Management
Displaced talar neck fractures are associated with a high rate of severe complications, regardless of the quality of surgical intervention. Anticipation and prompt management are crucial.
| Complication | Incidence / Risk Factors | Clinical Presentation | Management / Salvage Strategies |
|---|---|---|---|
| Avascular Necrosis (AVN) | Hawkins II: 20-50% ; Hawkins III: 70-100% ; Hawkins IV: >90% . Higher displacement, more severe comminution, prolonged time to reduction. | Persistent pain, especially with activity, decreased ankle/subtalar motion. Radiographs show increased sclerosis (Hawkins sign - subchondral lucency 6-8 weeks post-op is a good sign, indicating revascularization). Late collapse of talar dome. |
Early (pre-collapse):
Protected weight-bearing, core decompression, vascularized bone graft (e.g., medial femoral condyle flap) - controversial efficacy.
Late (post-collapse): Ankle/subtalar arthrodesis (talectomy with tibiocalcaneal fusion if severe), total ankle arthroplasty (rare, highly selected cases). |
| Nonunion / Malunion | Variable (up to 30%). Inadequate fixation, persistent distraction, infection, severe comminution, premature weight-bearing, AVN. | Persistent pain, deformity, limping, limited range of motion. Radiographs show lack of bridging callus, hardware failure. |
Nonunion:
Revision ORIF with bone grafting (autograft from iliac crest or calcaneus), potentially more rigid fixation.
Malunion: Corrective osteotomy (challenging), subtalar fusion for severe deformity and arthritis. |
| Post-Traumatic Arthritis (PTA) | High incidence (50-90%), often affecting subtalar joint first, then ankle. Incongruent reduction, cartilage damage at time of injury, AVN, malunion. | Chronic pain, stiffness, swelling, crepitus, loss of function, impaired gait. Radiographs show joint space narrowing, osteophytes, subchondral sclerosis. |
Early/Mild:
Conservative (NSAIDs, injections, physical therapy), arthroscopic debridement/synovectomy.
Severe: Subtalar arthrodesis, ankle arthrodesis, or combined tibiocalcaneal fusion depending on joint involvement. Total ankle arthroplasty (less common due to bone loss). |
| Infection | 10-20% for open fractures; <5% for closed. Open fracture, extensive soft tissue damage, prolonged surgery, patient comorbidities. | Redness, warmth, swelling, purulent drainage, fever, pain. Elevated inflammatory markers. |
Superficial:
Oral antibiotics, local wound care.
Deep: Urgent surgical debridement, tissue sampling for culture, prolonged IV antibiotics, hardware retention vs. removal depending on stability and organism. Serial debridements. |
| Hardware Complications | Up to 15%. Screw prominence (often requiring removal), screw breakage, loss of fixation. | Localized pain, impingement, skin irritation. Radiographic evidence of hardware issues. | Symptomatic hardware removal (typically >1 year post-op). Revision fixation for loss of reduction or hardware failure. |
| Nerve Injury | Rare. Superficial peroneal nerve, saphenous nerve. Direct trauma, traction, iatrogenic during surgical approach. | Numbness, tingling, dysesthesia, weakness in nerve distribution. | Conservative management for neurapraxia (observation, gabapentin). Surgical exploration and neurolysis for persistent symptoms or clear iatrogenic injury. |
| Wound Complications | Variable. Blistering, skin necrosis, dehiscence. Due to high-energy trauma, significant swelling, soft tissue stripping. | Skin changes, seroma, wound breakdown. | Local wound care, delayed primary closure, negative pressure wound therapy, debridement and flap coverage for severe cases. |
Post-Operative Rehabilitation Protocols
A structured and carefully phased rehabilitation protocol is essential for optimizing functional outcomes while protecting the fragile talar vascularity and fracture fixation. Weight-bearing restrictions are critical, especially given the high risk of AVN.
Phase 1: Immediate Post-Operative (Weeks 0-6/8)
*
Goal:
Protect fixation, control pain and swelling, maintain soft tissue integrity.
*
Immobilization:
* Initial non-removable cast or well-padded posterior splint with sugar tong in a neutral ankle position.
* Transition to a short leg non-weight-bearing cast or CAM walker boot (locked in neutral) once swelling subsides and sutures are removed (around 2 weeks).
*
Weight Bearing:
Strict
Non-Weight Bearing (NWB)
on the operative limb, typically for a minimum of 6-8 weeks, sometimes longer (up to 12-16 weeks) for higher Hawkins types or significant comminution/AVN risk. Use crutches or a knee scooter.
*
Elevation:
Keep the limb elevated above heart level as much as possible to reduce swelling.
*
Range of Motion (ROM):
* Encourage active and passive range of motion of toes and knee.
* Avoid direct ankle/subtalar ROM exercises during this initial phase to protect the fracture site.
*
Pain Management:
As prescribed.
*
Wound Care:
Monitor incision for signs of infection or dehiscence.
Phase 2: Early Mobilization & Controlled Weight Bearing (Weeks 8-12/16)
*
Goal:
Initiate gentle joint mobility, begin controlled weight bearing, maintain muscle strength.
*
Weight Bearing:
* Gradual progression to
Partial Weight Bearing (PWB)
in a CAM walker boot, starting with 25% body weight, advancing as tolerated based on radiographic healing and clinical assessment. This typically begins around 8-12 weeks post-op, but can be delayed further in high-risk cases.
* Radiographic evidence of early union is often required before initiating PWB.
*
Mobilization:
* Begin gentle, non-painful active and passive ankle and subtalar ROM exercises
out of the boot
. Focus on dorsiflexion, plantarflexion, inversion, and eversion.
* Initiate isometric strengthening exercises for the ankle musculature.
*
Manual Therapy:
Soft tissue massage for scar management, gentle joint mobilizations as tolerated.
*
Proprioception:
Begin with non-weight-bearing proprioceptive exercises (e.g., foot circles, alphabet).
Phase 3: Progressive Strengthening & Full Weight Bearing (Weeks 12-24)
*
Goal:
Restore full weight bearing, improve strength, endurance, and proprioception.
*
Weight Bearing:
* Progress to
Full Weight Bearing (FWB)
in the CAM walker boot, then transition to supportive shoes. The timing is individualized but often around 12-16 weeks.
* Gradually wean off the CAM boot as strength and confidence improve.
*
Strengthening:
* Progressive resistive exercises for ankle dorsiflexors, plantarflexors, invertors, and evertors (e.g., theraband exercises).
* Calf raises, heel walks, toe walks.
*
Balance & Proprioception:
* Single-leg stance, balance board exercises.
*
Gait Training:
Focus on normalized gait pattern.
*
Cardiovascular:
Non-impact activities (e.g., swimming, cycling).
Phase 4: Return to Activity / Advanced Rehabilitation (>24 Weeks)
*
Goal:
Achieve maximum functional recovery, return to recreational or sporting activities.
*
Advanced Strengthening:
Progress to higher-level functional exercises.
*
Plyometrics & Agility:
For athletes or individuals with high functional demands, introduce sport-specific drills, cutting, and jumping, ensuring adequate strength and joint stability.
*
Impact Activities:
Gradual introduction, carefully monitoring for pain or swelling.
*
Long-term Monitoring:
Regular follow-up for several years is crucial to monitor for signs of AVN, malunion, or progression of post-traumatic arthritis. Patients should be educated on the potential for these long-term complications.
Summary of Key Literature / Guidelines
The management of displaced talar neck fractures has evolved, but several fundamental principles and landmark studies continue to guide contemporary practice.
Classification Systems:
*
Hawkins Classification (1970):
Remains the cornerstone for grading talar neck fractures and predicting the risk of AVN. This system, originally focusing on subtalar dislocation, was later expanded by Canale and Kelly to include talonavicular dislocation (Type IV), further emphasizing the severity and higher AVN risk with greater displacement.
*
Marti-Weber Classification:
While less common for talar neck injuries specifically, it provides a broader classification for talar body and neck fractures.
Surgical Principles:
*
Anatomic Reduction and Rigid Internal Fixation:
The primary goal articulated by
Canale and Kelly (1978)
in their seminal paper, which demonstrated better outcomes with anatomic reduction and stable fixation. This has been consistently reaffirmed as crucial for minimizing malunion and post-traumatic arthritis.
*
Timing of Surgery:
The "wrinkle sign" as an indicator for optimal soft tissue conditions for closed fractures is widely accepted, though there is debate on the acceptable delay for definitive fixation (generally within 7-10 days to avoid difficult late reductions). For open fractures, the "six-hour rule" for debridement is paramount to prevent infection.
*
Approaches:
Dual medial and lateral approaches are often preferred for direct visualization and reduction in complex cases, enabling a convergent screw construct. However, minimal soft tissue stripping is emphasized to preserve vascularity.
*
Fixation:
Lag screw technique is preferred for compression. Two or three screws are generally adequate. Headless compression screws or partially threaded screws are common. The role of plates is growing for comminuted fractures, but they must be applied carefully to avoid soft tissue impingement.
Complications and Their Management:
*
Avascular Necrosis (AVN):
The most devastating complication, directly correlated with Hawkins type.
Hawkins (1970)
first described the subchondral lucency (Hawkins sign) on plain radiographs 6-8 weeks post-injury as a reliable indicator of intact vascularity and absence of AVN. Absence of this sign raises suspicion. Management ranges from conservative to complex salvage procedures (e.g., core decompression, vascularized bone grafts, arthrodesis). The decision to proceed with early arthrodesis versus waiting for collapse in high-risk AVN cases remains a subject of ongoing debate and depends on patient factors and joint involvement.
*
Post-Traumatic Arthritis (PTA):
Almost inevitable to some degree, particularly in the subtalar joint. It is a leading cause of long-term disability. While anatomic reduction mitigates severity, it does not eliminate the risk. Surgical options include arthroscopic debridement, osteotomies, or arthrodesis of the affected joints (subtalar, ankle, talonavicular).
*
Malunion:
Often leads to altered biomechanics and accelerated arthritis. Corrective osteotomies of the talus are technically demanding and carry high risks. Subtalar fusion is a more predictable salvage option for symptomatic malunion.
Current Trends & Future Directions:
*
Minimally Invasive Techniques:
While challenging for displaced fractures, some techniques are being explored for less displaced patterns.
*
Biological Augmentation:
The role of bone marrow aspirate concentrate (BMAC) or platelet-rich plasma (PRP) in fracture healing and preventing AVN is an active area of research, though robust evidence for routine use in talar neck fractures is still limited.
*
Advanced Imaging:
Wider use of 3D CT reconstructions for pre-operative planning.
*
Patient-Specific Outcomes:
Greater focus on patient-reported outcome measures (PROMs) to evaluate the true impact of different treatment strategies.
In conclusion, optimal treatment for displaced talar neck fractures demands meticulous surgical technique for anatomic reduction and stable fixation, tempered by an acute awareness of the precarious vascularity and high potential for debilitating long-term complications. A comprehensive understanding of the complex anatomy, systematic pre-operative planning, and a phased rehabilitation protocol are cornerstones of successful management. Continuous long-term follow-up is essential to address the often-delayed sequelae of these challenging injuries.
Clinical & Radiographic Imaging

