Introduction & Epidemiology
Masses and nodules along the medial cord of the foot and ankle represent a diverse spectrum of pathologies, ranging from benign soft tissue lesions to complex osteochondral anomalies impacting intricate biomechanical functions. The "medial cord" typically refers to the structures supporting the medial longitudinal arch, encompassing the posterior tibial tendon (PTT) and its insertions, the navicular bone, the spring ligament complex, and the associated neurovascular bundle. Pain and palpable masses in this region warrant thorough investigation due to the critical role these structures play in foot stability and ambulation.
Epidemiologically, the most common etiologies include:
*
Accessory Navicular Syndrome:
Present in 2-14% of the population, often bilateral (50-90%). Type II, with a synchondrosis between the accessory ossicle and the main navicular body, is most frequently symptomatic, typically presenting in adolescence due to increased activity or trauma.
*
Posterior Tibial Tendon Dysfunction (PTTD):
A progressive disorder leading to adult-acquired flatfoot deformity (AAFD). While not primarily a "mass," chronic tenosynovitis or hypertrophic changes can present as a palpable thickening or nodule, especially in earlier stages (Johnson and Strom Stage I/II). The prevalence increases with age, obesity, and in females.
*
Ganglion Cysts:
Represent the most common soft tissue tumors of the foot and ankle, arising from synovial sheaths or joint capsules. While often dorsal or lateral, they can occur medially, particularly around the talonavicular joint or PTT sheath.
*
Lipomas:
Benign fatty tumors, less common but can present as soft, mobile masses.
*
Nerve Sheath Tumors:
Schwannomas and neurofibromas involving the tibial nerve or its branches (medial plantar, lateral plantar, calcaneal nerves) are rare but critical to identify given their neural origin and potential for neurological symptoms.
*
Bursitis:
Adventitial bursae can form over bony prominences, such as an accessory navicular, leading to inflammation and a palpable mass.
*
Rare Lesions:
Synovial sarcoma, other benign or malignant soft tissue tumors, osteochondromas, or other less common conditions must always be considered in the differential diagnosis, especially with atypical presentations or concerning features.
Accurate diagnosis is paramount, guiding appropriate conservative or operative management strategies. The objective of surgical intervention is to alleviate pain, restore function, prevent disease progression, and, in some cases, exclude malignancy.
Surgical Anatomy & Biomechanics
A profound understanding of the medial ankle and foot anatomy is indispensable for surgical planning and execution, particularly when addressing masses along the medial cord.
Bony Structures
- Navicular Bone: A crucial component of the medial longitudinal arch, articulating with the talus proximally and the cuneiforms distally. The tuberosity of the navicular is the primary insertion site for the posterior tibial tendon.
-
Accessory Navicular (Os Tibiale Externum):
An extra ossification center located posteromedially to the main navicular body.
- Type I: A sesamoid bone within the PTT, usually asymptomatic.
- Type II: A triangular or heart-shaped ossicle connected to the navicular by a synchondrosis (fibrocartilaginous or cartilaginous), often symptomatic due to irritation from footwear or PTT traction.
- Type III (Cornuate Navicular): A fused accessory navicular with an enlarged, prominent navicular tuberosity, essentially a hypertrophied navicular.
- Talus & Calcaneus: Form the subtalar joint, critical for pronation/supination. The talar head articulates with the navicular, forming part of the talonavicular joint.
- Medial Cuneiform & First Metatarsal: Distal to the navicular, contributing to the medial column.
Ligamentous Structures
- Spring Ligament Complex (Plantar Calcaneonavicular Ligament): Comprising superomedial, medioplantar, and inferoplantar bands. This complex is vital for supporting the talar head and the medial longitudinal arch, working synergistically with the PTT. Dysfunction is a hallmark of AAFD.
- Deltoid Ligament Complex: The primary medial ankle stabilizer, originating from the medial malleolus. Its components (tibionavicular, tibiocalcaneal, anterior/posterior tibiotalar) provide robust stability.
Tendinous Structures
-
Posterior Tibial Tendon (PTT):
Originates from the posterior tibia and fibula, courses posterior to the medial malleolus, and inserts primarily onto the navicular tuberosity, with additional slips to the cuneiforms, cuboid, and bases of the 2nd-4th metatarsals.
- Function: The primary dynamic stabilizer of the medial longitudinal arch, responsible for hindfoot inversion and forefoot adduction. It acts as a supinator of the subtalar joint and a plantarflexor of the ankle.
- Pathology: In accessory navicular syndrome, the PTT often inserts into the accessory ossicle, altering its pull and potentially causing a traction apophysitis or tendinopathy at the synchondrosis. In PTTD, the tendon undergoes progressive degeneration, lengthening, and eventual rupture, leading to AAFD.
- Flexor Digitorum Longus (FDL) & Flexor Hallucis Longus (FHL): These tendons also run posterior to the medial malleolus and are important surgical landmarks. The FDL lies immediately deep (anterior) to the PTT.
Neurovascular Structures
- Tibial Nerve: Courses posterior to the medial malleolus, accompanied by the posterior tibial artery and veins (forming the neurovascular bundle). It typically bifurcates into the medial and lateral plantar nerves proximal or distal to the sustentaculum tali.
- Medial Calcaneal Nerve: Branches off the tibial nerve, providing sensation to the heel.
- Saphenous Nerve: A superficial sensory nerve, accompanying the great saphenous vein, traversing along the anteromedial aspect of the leg and ankle.
- Posterior Tibial Artery and Veins: Crucial for blood supply to the foot.
Biomechanics
The PTT, spring ligament, and navicular bone form a critical functional unit for maintaining the medial longitudinal arch.
*
Accessory Navicular:
Can impede the smooth gliding of the PTT, lead to tendinosis, or cause a lever arm dysfunction due to its abnormal insertion, contributing to medial arch pain and sometimes a subtle valgus deformity.
*
PTTD:
Leads to a progressive collapse of the medial longitudinal arch, hindfoot valgus, and forefoot abduction (the "too many toes" sign), evolving from tenosynovitis to tendon rupture and eventual rigid deformity.
Indications & Contraindications
Careful patient selection is paramount for successful outcomes when considering interventions for medial foot masses.
Operative Indications
-
Failure of Non-Operative Management:
Persistent, disabling pain and functional impairment despite an adequate trial (typically 3-6 months) of conservative measures.
- For Accessory Navicular Syndrome: This includes activity modification, orthotics (arch support, medial heel wedge), NSAIDs, physical therapy, and corticosteroid injections (though injections into the PTT sheath are controversial due to rupture risk).
- For PTTD with a Mass/Prominence: Similar conservative measures, often including bracing (AFO, UCBL orthosis) to support the arch.
- For Ganglion Cysts/Benign Masses: Observation if asymptomatic; aspiration if symptomatic (with high recurrence rates); excision if painful, enlarging, compressive, or cosmetic.
- Neurological Compromise: Mass-effect causing definitive compression or entrapment of the tibial nerve or its branches (e.g., tarsal tunnel syndrome), leading to intractable pain, paresthesia, or motor weakness.
- Progressive Deformity: In the context of PTTD, progression of hindfoot valgus or forefoot abduction that cannot be controlled non-operatively.
- Suspicion of Malignancy: Any mass with rapidly changing characteristics, atypical imaging features, or deep location warrants urgent biopsy or wide local excision with appropriate oncologic margins.
- Functional Limitation: Masses causing significant mechanical irritation, difficulty with shoe wear, or impediment to activities of daily living or athletic performance.
Contraindications
- Active Local or Systemic Infection: Surgical intervention should be deferred until infection is resolved.
- Uncontrolled Systemic Comorbidities: Severe peripheral vascular disease, uncontrolled diabetes, significant cardiac or pulmonary compromise that significantly increases surgical risks.
- Poor Skin Quality: Active ulceration, severe skin atrophy, or history of radiation in the surgical field.
- Unrealistic Patient Expectations: Inadequate understanding of potential outcomes, complications, or rehabilitation commitment.
- Lack of Adherence to Post-Operative Protocols: Patients unable or unwilling to comply with immobilization, non-weight-bearing, or rehabilitation regimens.
Table: Operative vs. Non-Operative Indications for Medial Foot Nodule Pain
| Feature / Condition | Non-Operative Management (Initial Trial 3-6 Months) | Operative Management (Indicated After Failed Conservative) |
|---|---|---|
| Accessory Navicular Syndrome | Activity modification, supportive footwear, orthotics (arch support, medial heel wedge), NSAIDs, physical therapy, corticosteroid injections (cautious). | Persistent pain, PTT dysfunction, bursa formation, significant functional limitation. Excision (Kidner procedure if PTT is involved). |
| PTTD (Early Stages I/II) | RICE, NSAIDs, custom orthotics (UCBL), bracing (AFO), physical therapy (PTT strengthening), weight loss. | Persistent pain, progressive deformity (hindfoot valgus, forefoot abduction), PTT tendinosis/tears despite bracing, functional decline. Tenosynovectomy, debridement, repair, +/- FDL transfer, +/- medializing calcaneal osteotomy/lateral column lengthening (depending on stage). |
| Ganglion Cysts | Observation if asymptomatic, aspiration (high recurrence). | Persistent pain, nerve compression, recurrent after aspiration, rapidly enlarging, cosmetic concern, functional impairment, or diagnostic uncertainty. Complete excision. |
| Lipomas | Observation if asymptomatic and small. | Symptomatic (pain, compression), rapidly enlarging, cosmetic concern, functional impairment, or diagnostic uncertainty (rule out malignancy). Excision. |
| Nerve Sheath Tumors | Observation if small, asymptomatic, and stable on imaging. | Symptomatic (pain, paresthesia, motor weakness), enlarging, diagnostic uncertainty (malignancy concern). Excision with careful attention to nerve preservation (enucleation for schwannomas, resection for neurofibromas +/- grafting). |
| Suspected Malignancy | None, unless for symptom control pending definitive diagnosis. | Biopsy (incisional or excisional) followed by appropriate oncologic resection based on pathology (e.g., wide local excision with clear margins). |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to ensure a successful outcome and minimize complications.
Clinical Assessment
- Comprehensive History: Detailed pain characteristics (location, quality, exacerbating/alleviating factors), duration of symptoms, previous treatments and their efficacy, impact on activities, neurological symptoms (numbness, tingling, weakness).
-
Thorough Physical Examination:
- Inspection: Observe for skin changes, swelling, erythema, callosities, deformity (e.g., medial arch collapse, hindfoot valgus, "too many toes" sign for PTTD). Palpate the mass, noting its size, consistency, mobility, tenderness, and relationship to underlying structures.
- Palpation: Precisely locate the maximal tenderness. Assess the PTT for thickening, tenderness, or crepitus. Palpate the accessory navicular or other bony prominences. Evaluate for tarsal tunnel tenderness.
- Range of Motion (ROM): Ankle and subtalar joint ROM. Assess for pain with PTT loading (resisted inversion and plantarflexion).
- Muscle Strength: Evaluate PTT strength (single heel raise test for PTTD).
- Neurological Exam: Assess sensation (light touch, pinprick) in the distribution of the tibial nerve branches and saphenous nerve. Motor strength of intrinsic foot muscles.
- Vascular Exam: Palpate posterior tibial and dorsalis pedis pulses. Capillary refill.
Imaging
-
Weight-Bearing Radiographs (AP, Lateral, Oblique Foot/Ankle):
Crucial for bony assessment.
- Identify accessory navicular (Type II often seen as a separate ossicle).
- Assess for other bony abnormalities (osteophytes, tarsal coalition, stress fractures).
- Evaluate the medial longitudinal arch height and alignment (Meary's angle, Talo-first metatarsal angle on lateral view; Talo-navicular coverage angle on AP view) for PTTD assessment.
-
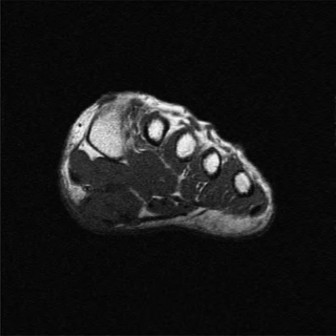
Magnetic Resonance Imaging (MRI):
The gold standard for soft tissue evaluation.
- Precisely characterizes masses (cystic vs. solid, vascularity).
- Assesses PTT integrity (tendinosis, partial tears, full ruptures).
- Evaluates inflammatory changes (bone marrow edema, tenosynovitis).
- Defines relationship of mass to neurovascular structures.
-
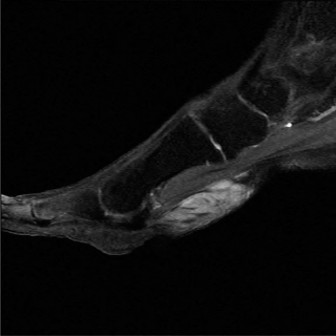 (This image, potentially an MRI, could illustrate PTT pathology or an accessory navicular.)
(This image, potentially an MRI, could illustrate PTT pathology or an accessory navicular.)
-
Ultrasound:
Operator-dependent but offers dynamic evaluation.
- Differentiates cystic from solid lesions.
- Assesses PTT pathology (tendinosis, tears, tenosynovitis).
- Evaluates vascularity.
- Can guide aspiration or injection.
- Computed Tomography (CT): Less frequently used for soft tissue masses, but invaluable for complex bony anatomy (e.g., tarsal coalition, osteochondromas, evaluating a Type III cornuate navicular).
Pre-Operative Consultation
- Anesthesiology: For general or regional anesthesia planning.
- Internal Medicine/Specialists: If significant comorbidities require optimization.
- Oncology: If malignancy is suspected, for multidisciplinary planning.
Patient Positioning
- Supine Position: Standard for medial foot and ankle surgery.
- Hip Bump: A bolster or towel roll placed under the ipsilateral hip facilitates internal rotation of the limb, allowing easier access to the medial aspect of the foot.
- Tourniquet: A thigh tourniquet is typically applied to minimize blood loss and improve visualization. Alternatively, an ankle tourniquet can be used for shorter procedures in compliant patients.
- Image Intensifier (Fluoroscopy): Positioned to allow intraoperative AP and lateral views, particularly important for bony resections or hardware placement.
- Pre-operative Marking: Mark the incision site, palpable mass, and key anatomical landmarks (medial malleolus, navicular tuberosity, course of saphenous vein/nerve).
Detailed Surgical Approach / Technique
The surgical approach to masses along the medial cord requires meticulous technique, precise anatomical identification, and careful preservation of vital neurovascular structures. The specific steps vary depending on the underlying pathology, but general principles apply. Here we describe common techniques for accessory navicular excision and general soft tissue mass removal.
General Principles
- Aseptic Technique: Strict sterile field maintenance.
- Incision Planning: Longitudinal incision, typically parallel to the course of the PTT, curvilinear if necessary to follow skin creases or improve exposure. Avoid crossing flexion creases perpendicularly.
- Hemostasis: Use of tourniquet and judicious electrocautery.
- Neurovascular Protection: Identify and protect the saphenous nerve and great saphenous vein superficially, and the tibial neurovascular bundle deeper.
Approach to Medial Ankle/Foot
- Incision: A curvilinear or longitudinal incision, approximately 6-8 cm, centered over the palpable mass or the accessory navicular/navicular tuberosity. The incision starts proximal to the medial malleolus and extends distally towards the navicular tuberosity.
- Subcutaneous Dissection: Carefully incise the skin and subcutaneous tissue. Identify and protect the great saphenous vein and the saphenous nerve branches (anterior and posterior branches) which run superficially. These should be gently retracted.
- Deep Fascia: Incise the deep fascia over the PTT sheath.
Accessory Navicular Excision (Modified Kidner Procedure Principles)
The goal is to remove the symptomatic accessory ossicle and reposition the PTT to its correct anatomical insertion on the main navicular body.
- Expose PTT and Accessory Navicular: Identify the posterior tibial tendon as it courses posterior to the medial malleolus and inserts onto the accessory navicular. The accessory navicular will be visible as a distinct bony prominence or a separate ossicle anterior to the medial malleolus.
- Assess PTT Involvement: Carefully evaluate the insertion of the PTT. In symptomatic Type II accessory navicular, the PTT often inserts predominantly or entirely into the accessory ossicle, or the ossicle itself irritates the tendon.
- Release PTT (if necessary): If the PTT inserts into the accessory navicular, a portion of the tendinous attachment to the ossicle may need to be carefully released. Preserve as much of the plantar-most fibers inserting onto the main navicular as possible.
-
Excision of Accessory Navicular:
- Make a longitudinal incision through the periosteum over the accessory navicular.
- Using an osteotome or small rongeur, carefully dissect and remove the accessory ossicle. Ensure complete removal of any cartilaginous or fibrous synchondrosis, as residual tissue can be a source of continued pain.
- Contour the remaining navicular tuberosity to remove any sharp edges or prominences.
-
 (This image could depict the accessory navicular being excised or a view of the post-excision navicular tuberosity.)
(This image could depict the accessory navicular being excised or a view of the post-excision navicular tuberosity.)
-
Re-routing and Re-attachment of PTT:
- Mobilize the posterior tibial tendon, ensuring it is free from any impinging structures. The goal is to shift its insertion more medially and inferiorly.
- Prepare the main navicular body: If a large defect or insufficient attachment site remains, a trough can be created or drill holes can be made in the main navicular tuberosity.
- Pass the PTT (or its released portion) into the prepared navicular bed.
- Secure the PTT using non-absorbable sutures via transosseous tunnels or suture anchors. Ensure adequate tension without overtensioning. The re-attached tendon should lie flat against the navicular.
-
(This image likely illustrates the re-attachment of the PTT to the navicular, possibly with suture anchors.)
- Inspection and Closure: Irrigates the wound. Ensure full range of motion. Close the deep fascia, subcutaneous layers, and skin.
Soft Tissue Mass Excision (e.g., Ganglion, Lipoma, Nerve Sheath Tumor)
- Exposure: The incision should be directly over the palpable mass, ensuring adequate exposure. Deepen the incision through subcutaneous tissue and fascia.
- Neurovascular Identification: This is critical. Identify the great saphenous vein and saphenous nerve branches superficially. Deeper, carefully identify the tibial neurovascular bundle (tibial nerve, posterior tibial artery and veins) and its branches. These structures should be meticulously dissected free and retracted.
-
Mass Dissection:
- Ganglion Cyst: Identify the cyst capsule and trace its stalk to its origin (usually a joint capsule or tendon sheath). Excise the entire cyst, including its pedicle, to minimize recurrence. Avoid rupturing the cyst if possible, to aid in complete removal of the lining.
- Lipoma: These are typically encapsulated. Dissect circumferentially around the pseudocapsule. Usually, they can be easily "shelled out."
-
Nerve Sheath Tumor (Schwannoma, Neurofibroma):
Requires the utmost care. The mass will be intimately associated with the nerve.
- Schwannomas: Often eccentric to the nerve fascicles and can sometimes be "shelled out" or enucleated from the nerve, preserving the main nerve trunk. Intraoperative nerve stimulation can help identify functional fascicles.
- Neurofibromas: Involve the nerve more diffusely, often requiring partial or complete resection of the nerve segment, potentially necessitating nerve grafting if motor function is critical. Biopsy (frozen section) may be performed to confirm benignity before definitive excision.
-
 (This image could show the careful dissection of a soft tissue mass, possibly a ganglion or lipoma, with surrounding structures.)
(This image could show the careful dissection of a soft tissue mass, possibly a ganglion or lipoma, with surrounding structures.)
-
 (This image might illustrate another soft tissue mass, perhaps a more encapsulated one, being removed.)
(This image might illustrate another soft tissue mass, perhaps a more encapsulated one, being removed.)
- Hemostasis: Achieved with electrocautery or ligatures.
- Specimen Handling: Send all excised tissue for histopathological examination.
- Closure: Irrigates the wound. Close the deep fascia (if opened) to avoid muscle herniation. Close subcutaneous tissue and skin layers meticulously.
Post-Excision Considerations
- PTTD Concurrent Pathology: If significant PTTD is noted during accessory navicular excision, concurrent tenosynovectomy, debridement of degenerated tendon, or even FDL transfer may be indicated. However, this expands the scope of the procedure significantly.
- Adhesiolysis: Release any adhesions found involving the PTT or neurovascular structures.
-
Wound Dressings:
Apply sterile dressings. A splint or cast may be applied depending on the extent of the procedure and need for immobilization.
-
 (This image could show the completed incision closure or a specific dressing application.)
(This image could show the completed incision closure or a specific dressing application.)
-
Complications & Management
Surgical intervention for medial foot masses, while often successful, carries inherent risks. A comprehensive understanding of potential complications and their management is crucial for all orthopedic surgeons.
General Surgical Complications
-
Infection:
Superficial (cellulitis) or deep (surgical site infection, osteomyelitis). Incidence varies, generally low (1-5%).
- Management: Prompt IV antibiotics, wound debridement, washout, possibly hardware removal in severe cases.
-
Wound Healing Issues:
Dehiscence, hematoma, seroma, skin necrosis. Factors include poor circulation, tension, diabetes, smoking.
- Management: Local wound care, débridement, negative pressure wound therapy, or surgical revision. Hematomas/seromas may require aspiration or drainage.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
Risk varies based on procedure length, patient comorbidities, and immobilization.
- Management: Prophylaxis (chemical and mechanical), early mobilization. Treatment involves anticoagulation.
-
Complex Regional Pain Syndrome (CRPS):
A rare but debilitating neuropathic pain condition.
- Management: Early recognition, multimodal pain management, physical therapy, sympathetic blocks.
Specific Complications Related to Medial Foot Mass Excision
-
Recurrence of Mass:
-
Ganglion Cysts:
High recurrence rate (up to 30%) even with complete excision of the stalk.
- Management: Re-excision, sometimes with a broader capsular resection.
-
Accessory Navicular:
Incomplete removal of the ossicle or synchondrosis, or residual prominent navicular tuberosity.
- Management: Revision surgery to remove residual bone and re-contour.
-
Ganglion Cysts:
High recurrence rate (up to 30%) even with complete excision of the stalk.
-
Continued Pain:
-
Inadequate PTT Reattachment/Function:
If PTT reattachment is compromised or the tendon remains dysfunctional, pain and arch collapse may persist.
- Management: Re-evaluation of tendon integrity (MRI), revision surgery (reattachment, augmentation with FDL transfer).
-
Residual Pathology:
Unrecognized tarsal coalition, subtalar pathology, or concurrent nerve entrapment.
- Management: Further imaging, diagnostic injections, specific addressing of the unrecognized pathology.
-
Neuroma:
Injury to saphenous nerve branches or formation of painful scar neuromas.
- Management: Neuropathic pain medications, corticosteroid injections, surgical excision of neuroma with burying in muscle or bone.
-
Inadequate PTT Reattachment/Function:
If PTT reattachment is compromised or the tendon remains dysfunctional, pain and arch collapse may persist.
-
Nerve Injury:
-
Saphenous Nerve:
Paresthesia, numbness, or dysesthesia along the medial ankle and arch. Relatively common.
- Management: Observation (often resolves), neuropathic pain medications, surgical neurolysis or neurectomy for persistent, severe symptoms.
-
Tibial Nerve/Branches:
Rare but severe, leading to motor weakness or profound sensory loss (e.g., tarsal tunnel syndrome post-op).
- Management: Urgent re-exploration if acute compression suspected. Nerve repair/grafting if transection occurs. Long-term management of neuropathic pain and functional deficits.
-
Saphenous Nerve:
Paresthesia, numbness, or dysesthesia along the medial ankle and arch. Relatively common.
-
PTT Weakness/Failure:
Can occur due to aggressive debridement, over-resection, or compromised reattachment, leading to arch collapse.
- Management: Intensive physical therapy, orthotics, or revision surgery including PTT reconstruction/augmentation.
-
Stiffness/Adhesions:
Scar tissue can restrict ankle/foot motion or tether tendons.
- Management: Early range of motion exercises, physical therapy.
-
Osseous Nonunion/Malunion:
If osteotomies or fusions are performed (less common for simple mass excision but relevant for complex PTTD reconstruction).
- Management: Immobilization, bone stimulators, revision surgery with bone grafting and stable fixation.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Recurrence of Ganglion Cyst | 10-30% | Re-excision, ensuring complete removal of the stalk/origin, possibly broader capsular resection. |
| Residual Accessory Navicular Pain | 5-15% | Revision surgery to ensure complete removal of ossicle/synchondrosis, re-contour navicular tuberosity, verify PTT reattachment. |
| Infection | 1-5% | Systemic antibiotics (IV for deep), surgical debridement, washout, possibly implant removal (if applicable). |
| Wound Dehiscence | 2-8% | Local wound care, offloading, débridement, secondary closure, skin grafting, or flap reconstruction for extensive defects. |
| Saphenous Nerve Dysesthesia/Neuroma | 5-20% (transient) | Observation (often self-resolving), neuropathic pain medication, local injections. Surgical neurolysis or neurectomy with proximal stump burial for intractable cases. |
| PTT Dysfunction/Weakness | 5-10% (post-Kidner) | Aggressive rehabilitation, orthotic support. Revision surgery: PTT advancement, FDL transfer to augment PTT, medializing calcaneal osteotomy for persistent deformity. |
| CRPS | <1% | Multidisciplinary approach: pain management (medications, blocks), physical therapy, psychological support. Early recognition is key. |
| Deep Vein Thrombosis (DVT) | <1% (with prophylaxis) | Anticoagulation (LMWH, oral anticoagulants), pulmonary embolism management as needed. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing outcomes, restoring function, and preventing recurrence or secondary complications. Protocols must be tailored to the specific procedure performed, patient factors, and intraoperative findings.
Phase I: Protection and Immobilization (Weeks 0-6)
- Goal: Protect surgical repair/site, minimize pain and swelling, prevent wound complications.
-
Immobilization:
- Accessory Navicular Excision with PTT Reattachment (Kidner): Non-weight bearing (NWB) in a short leg cast or removable boot (locked in neutral) for 4-6 weeks.
- Simple Soft Tissue Mass Excision (without tendon/bone repair): Immediate protected weight-bearing in a surgical shoe or cam walker, transitioning out of immobilizer as pain allows (often 1-2 weeks NWB, then progressive PWB).
- Pain & Swelling Management: Elevation, ice, oral analgesics.
- Early Motion: Active range of motion (AROM) of toes. Gentle, pain-free ankle dorsiflexion/plantarflexion (within cast if windowed, or during non-weight-bearing periods if in removable boot). Avoid active PTT loading/inversion initially with Kidner.
- Wound Care: Monitor incision for signs of infection.
Phase II: Controlled Mobilization & Early Strengthening (Weeks 6-12)
- Goal: Gradually restore ankle/foot ROM, initiate muscle strengthening, progress weight-bearing.
-
Weight-Bearing Progression:
- Accessory Navicular/PTT Reattachment: Transition to cam walker boot. Begin partial weight-bearing (PWB) at 6 weeks, progressing to full weight-bearing (FWB) over 2-4 weeks.
- Soft Tissue Mass Excision: If not already, transition to FWB in supportive shoe.
-
Physical Therapy (PT) Focus:
- ROM: Active and passive ankle/subtalar ROM exercises. Emphasis on achieving full dorsiflexion and subtalar inversion/eversion.
-
Strengthening:
- PTT Reattachment: Initiate gentle isometric PTT contractions (inversion). Progress to resistive exercises with therabands.
- General: Isometric and concentric/eccentric exercises for all ankle musculature (dorsiflexors, plantarflexors, evertors).
- Balance & Proprioception: Single leg stance, wobble board exercises (initiated once FWB is achieved and pain allows).
- Support: Consider custom or off-the-shelf orthotics, especially for patients with pre-existing flatfoot tendency or those who underwent PTT procedures.
Phase III: Advanced Strengthening & Return to Activity (Weeks 12+)
- Goal: Maximize strength, endurance, power, and return to full activities.
- Wean from Boot: Transition from cam walker to supportive athletic shoes, often with custom orthotics.
-
Progressive Strengthening:
- Eccentric PTT strengthening.
- Calf raises (bilateral to unilateral).
- Plyometric exercises (hopping, jumping) for athletes.
- Agility & Sport-Specific Training: Cutting maneuvers, sport-specific drills.
- Endurance Training: Walking, cycling, swimming, elliptical.
- Return to Activity: Gradual return to demanding activities and sports. Full return may take 4-6 months, or up to 9-12 months for more complex PTT reconstructions. Avoid high-impact activities initially.
- Patient Education: Continue home exercise program, proper footwear, and awareness of any warning signs.
Note: For complex PTTD reconstructions involving osteotomies or fusions, rehabilitation protocols are significantly longer and more protective in the early phases, with prolonged NWB periods. The described protocol primarily targets isolated mass excision or accessory navicular removal with PTT reattachment.
Summary of Key Literature / Guidelines
The management of medial foot masses, particularly accessory navicular syndrome and PTTD, is well-documented in orthopedic literature, though some areas remain subject to ongoing research and debate.
Accessory Navicular Syndrome
-
Kidner Procedure:
Historically described by Kidner in 1929, the procedure involves excision of the accessory navicular and re-routing/reattachment of the PTT to the main navicular tuberosity. Studies consistently show high success rates (80-90% good to excellent results) in relieving pain and improving function, particularly for symptomatic Type II lesions refractory to conservative treatment.
- Literature Insight: Sammarco et al. (2001) highlighted the importance of complete excision of the ossicle and meticulous PTT reattachment. Shantharam and colleagues (2012) reported on long-term outcomes of modified Kidner procedure with favorable results and low recurrence.
- Debate: The extent of PTT detachment and re-routing remains debated. Some advocate for minimal release if the PTT largely inserts onto the main navicular, while others emphasize full release and re-anchoring to correct biomechanics.
Posterior Tibial Tendon Dysfunction (PTTD)
-
Johnson and Strom Classification (1989):
This staging system remains the cornerstone for guiding PTTD management:
- Stage I: Tenosynovitis, mild weakness, no deformity. Managed conservatively.
- Stage II: Flexible flatfoot deformity, tendon lengthening/degeneration, painful. Often requires tendon transfer (e.g., FDL) with concomitant bony procedures (e.g., medializing calcaneal osteotomy, lateral column lengthening).
- Stage III: Fixed flatfoot deformity, significant tendon pathology. Requires arthrodesis (e.g., triple arthrodesis).
- Stage IV: Ankle valgus, deltoid ligament insufficiency. Requires ankle fusion or total ankle arthroplasty in addition to hindfoot correction.
- Conservative Management: Guidelines from organizations like the American Academy of Orthopaedic Surgeons (AAOS) emphasize a trial of non-operative treatment (orthotics, bracing, physical therapy) as first-line for Stage I/II PTTD.
- Surgical Options: A vast body of literature details various surgical approaches for PTTD, including tenosynovectomy, debridement, primary repair, FDL transfer, numerous osteotomies (medializing calcaneal, lateral column lengthening, Cotton), and fusions. The choice is dictated by the stage of deformity and patient factors. Studies by Myerson et al. (2002) and Conti et al. (2004) provide extensive reviews of surgical techniques and outcomes.
Ganglion Cysts & Other Soft Tissue Masses
-
Excision vs. Aspiration:
Open surgical excision remains the definitive treatment for symptomatic ganglion cysts due to significantly lower recurrence rates compared to aspiration (10-30% vs. 50-70%).
- Literature Insight: A systematic review by Head et al. (2015) in Cochrane Database supports excision for lower recurrence rates.
-
Nerve Sheath Tumors:
The literature emphasizes careful pre-operative imaging (MRI) and meticulous intraoperative dissection for these rare lesions. For schwannomas, enucleation is often possible, while neurofibromas may require resection. The challenge lies in balancing complete tumor removal with nerve function preservation.
- Guideline Insight: The principles of soft tissue tumor surgery, including clear margins and appropriate biopsy techniques, are critical, often guided by broader oncologic surgical principles.
General Guidelines
- Imaging: MRI is consistently recommended as the primary advanced imaging modality for evaluating soft tissue masses and tendon pathology, particularly PTTD.
- Evidence-Based Medicine: Continued emphasis on shared decision-making with patients, based on the best available evidence for each specific pathology and its stage.
- Multidisciplinary Approach: For complex cases, particularly suspected malignancies or severe deformities, a multidisciplinary team involving orthopedic surgeons, radiologists, oncologists, and physical therapists is ideal.
