Introduction & Epidemiology
Chronic foot pain is a ubiquitous presenting complaint in orthopedic practice, often posing diagnostic and therapeutic challenges. While myriad pathologies can contribute, conditions affecting the flexor digitorum longus (FDL) tendon and its sheath represent a distinct subset that, when appropriately identified, can benefit from targeted surgical intervention. Debridement of the FDL tendon or its surrounding synovium is a procedure indicated for refractory FDL tenosynovitis, tendinopathy, or specific instances of FDL involvement in complex foot deformities.
FDL tenosynovitis, characterized by inflammation of the tendon sheath, often presents with pain along the posteromedial ankle and medial midfoot, exacerbated by activity and resisted toe flexion. Tendinopathy, encompassing degenerative changes within the tendon structure, can manifest similarly but may also include palpable nodularity or thickening. The incidence of isolated FDL pathology is not as well-defined as more common conditions like Achilles tendinopathy or plantar fasciitis, often being a concurrent finding or a secondary complaint in the context of posterior tibial tendon dysfunction (PTTD), accessory navicular syndrome, or tarsal tunnel syndrome. Epidemiologically, it is more commonly observed in active individuals, particularly runners, dancers, or those engaging in activities requiring repetitive toe flexion or propulsion. Mechanical overload, anatomical variations leading to impingement, inflammatory arthropathies, and systemic conditions such as diabetes can predispose individuals to FDL pathology. A thorough differential diagnosis is crucial, distinguishing FDL-related pain from nerve entrapment, osteochondral lesions, spring ligament pathology, or other tendinopathies.
Surgical Anatomy & Biomechanics
A precise understanding of the FDL's anatomy and biomechanical role is paramount for surgical success and complication avoidance.
Anatomy
The FDL muscle originates from the posterior surface of the tibia, distal to the soleal line, and medial to the tibialis posterior muscle. Its robust tendon descends distally, passing through the tarsal tunnel posterior to the medial malleolus, deep to the flexor retinaculum. Within the tarsal tunnel, the FDL tendon lies anterior to the posterior tibial neurovascular bundle (posterior tibial artery, posterior tibial nerve, and venae comitantes) and posterior to the tibialis posterior tendon (PTT). The FDL's course within the tarsal tunnel is often deep and immediately adjacent to the sustentaculum tali of the calcaneus, where it can be subject to compression or friction.
Distal to the tarsal tunnel, the FDL tendon crosses superficial to the flexor hallucis longus (FHL) tendon in a configuration known as the "knot of Henry" or master knot of Henry, typically located beneath the navicular tuberosity or medial cuneiform. At this intersection, a communicating slip of tendon often transfers from the FDL to the FHL, or vice versa, contributing to a synergistic action. The FDL then bifurcates, sending slips to the plantar aspects of the distal phalanges of the second through fifth toes, each enclosed within its own synovial sheath and fibrous flexor sheath system. The quadratus plantae muscle inserts into the FDL tendon, altering its line of pull.
Key relationships:
*
Posterior Tibial Tendon (PTT):
FDL is deep to PTT at the level of the medial malleolus. PTT lies more anterior within the tarsal tunnel.
*
Flexor Hallucis Longus (FHL):
FDL crosses superficial to FHL at the knot of Henry. FHL is the most lateral tendon within the tarsal tunnel.
*
Neurovascular Bundle:
The posterior tibial nerve and artery are superficial and posterior to the FDL within the tarsal tunnel, making them susceptible to injury during a posteromedial approach. The saphenous nerve and great saphenous vein are more superficial and anterior, near the incision site.
Biomechanics
The FDL primarily functions as a flexor of the second through fifth toes at the distal interphalangeal (DIP) and proximal interphalangeal (PIP) joints, and secondarily as a plantarflexor of the ankle and supinator of the subtalar joint. Its action is critical during the propulsion phase of gait, contributing to forefoot rigidity and efficient toe-off. In the context of chronic foot pain, repetitive microtrauma from these functions, especially with inadequate recovery or excessive load, can lead to tendinopathy or tenosynovitis. Its role in dynamic arch support, though less significant than the PTT, contributes to hindfoot stability. Overactivity of the FDL can sometimes contribute to hammer toe deformities, particularly in the lesser toes.

Indications & Contraindications
The decision for surgical debridement of the FDL tendon requires careful consideration of patient symptoms, imaging findings, and failure of non-operative measures.
Indications
- Chronic FDL Tenosynovitis: Persistent inflammation of the FDL tendon sheath, refractory to a minimum of 3-6 months of conservative management (e.g., rest, NSAIDs, physical therapy, orthotics, corticosteroid injections). Symptoms typically include localized pain, swelling, and tenderness along the FDL course, especially posteromedially.
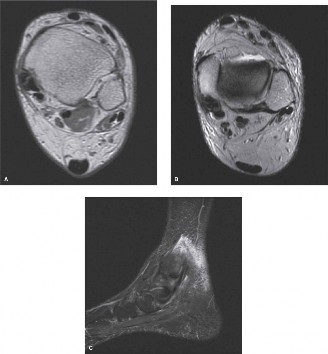
- FDL Tendinopathy: Degenerative changes within the FDL tendon (e.g., mucoid degeneration, focal tears, hypertrophic nodularity) causing persistent pain and dysfunction. MRI often reveals increased signal intensity within the tendon substance, thickening, or intratendinous tears.
- Mechanical Impingement: Documented impingement of the FDL tendon due to anatomical variations, osteophytes, or adjacent soft tissue pathology within the tarsal tunnel or at the master knot of Henry.
- Space-Occupying Lesions: Ganglion cysts or other benign masses within the FDL tendon sheath causing compressive symptoms or direct pain.
- Adjunctive Procedure: In cases of severe PTTD (typically Stage II or greater), where FDL transfer is performed for hindfoot stabilization and arch reconstruction, debridement of associated FDL tendinopathy is often undertaken concurrently. However, the primary indication for debridement as a standalone procedure is usually severe FDL-specific pathology.
- Failed Previous Surgery: Recurrence of symptoms after prior unsuccessful conservative or minimally invasive treatments.
Contraindications
- Acute Infection: Local or systemic infection, which must be controlled prior to elective surgery.
- Uncorrected Severe Biomechanical Deformities: Significant underlying structural deformities (e.g., severe pes planus without planned correction) that would perpetuate FDL overload and render isolated debridement ineffective.
- Poor Surgical Candidate: Significant comorbidities (uncontrolled diabetes, peripheral vascular disease, severe neuropathy) that increase surgical risks or impair healing.
- Non-Compliance: Patients unwilling or unable to adhere to post-operative rehabilitation protocols.
- Diffuse Undifferentiated Foot Pain: When FDL pathology is not clearly identified as the primary pain generator or when symptoms are vague and widespread, without focal tenderness or imaging correlation.
- Early-Stage Pathology: Initial presentations of FDL tenosynovitis or mild tendinopathy that have not undergone an adequate course of non-operative management.
Operative vs. Non-Operative Indications
| Feature | Operative Indications | Non-Operative Indications |
|---|---|---|
| Duration of Symptoms | Chronic (> 6 months) | Acute or subacute (< 6 months) |
| Response to Conservative Rx | Failure of comprehensive non-operative management (e.g., NSAIDs, PT, orthotics, injections) for at least 3-6 months. | Initial presentation, mild to moderate symptoms, first-line treatment. |
| Imaging Findings (MRI/US) | Severe tenosynovitis (thickened sheath, effusion), significant tendinopathy (intratendinous signal changes, degeneration, partial tears), mechanical impingement, space-occupying lesions. | Mild tenosynovitis (minimal effusion), early tendinosis (minor signal changes), no significant tears or impingement. |
| Clinical Presentation | Persistent, localized posteromedial pain, swelling, tenderness along FDL, pain with resisted toe flexion, functional impairment, palpable nodules/thickening. | Intermittent pain, pain improving with rest, no significant functional limitation, diffuse non-specific pain, systemic inflammatory conditions responding to medical management. |
| Patient Factors | Motivated patient, good overall health, understanding of surgical risks and recovery, desire to return to higher-level activities. | Uncontrolled systemic comorbidities, active infection, severe peripheral neuropathy, unaddressed psychological factors, non-compliance concerns, patient preference for non-surgical options. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to optimize outcomes and mitigate complications.
Pre-Operative Planning
-
Detailed History and Physical Examination:
- History: Ascertain chronicity, precise location, character of pain, aggravating/alleviating factors, previous treatments and their efficacy, activity level, and systemic medical conditions.
- Physical Exam: Inspect for swelling, erythema, or deformity. Palpate along the entire course of the FDL tendon, focusing on the posteromedial ankle, tarsal tunnel, and distal course towards the toes. Assess pain with resisted toe flexion (second through fifth toes). Evaluate foot posture (pes planus, cavus), ankle and subtalar range of motion, and gait mechanics. Rule out other pathologies such as PTTD (too many toes sign, single leg heel raise test), spring ligament laxity, or nerve entrapment (Tinel's sign for posterior tibial nerve).
-
Imaging Studies:
- Radiographs: Weight-bearing anteroposterior, lateral, and oblique views of the foot and ankle are standard to assess bony alignment, rule out fractures, arthritis, or osseous impingement.
- Magnetic Resonance Imaging (MRI): The gold standard for evaluating soft tissues. MRI can delineate FDL tenosynovitis (fluid within the sheath, synovial thickening), tendinopathy (intratendinous signal alteration, thickening), partial or full-thickness tears, and associated pathologies like spring ligament injury or PTTD. It is crucial for guiding the extent of debridement.
- Ultrasound: Dynamic ultrasound can be a useful adjunct to assess FDL tendon motion, effusion, and identify areas of impingement or tendinosis, particularly in experienced hands. It can also guide diagnostic/therapeutic injections.
- Patient Education and Consent: Thoroughly discuss the diagnosis, surgical procedure (debridement, potential for tenosynovectomy), expected outcomes, potential complications (e.g., residual pain, nerve injury, infection, stiffness), and post-operative rehabilitation protocol. Ensure the patient has realistic expectations.
- Anesthesia Consultation: General anesthesia or spinal/regional anesthesia (e.g., popliteal block) is typically employed. The choice depends on patient comorbidities and surgeon/anesthesiologist preference.
Patient Positioning
- Supine Position: The patient is positioned supine on the operating table.
- Tourniquet Application: A high thigh tourniquet is applied to achieve a bloodless field, which is critical for visualizing delicate soft tissue structures and minimizing nerve injury risk. A low ankle tourniquet can also be used for shorter procedures or specific patient indications.
- Leg Prep and Drape: The affected limb is prepped circumferentially from the knee to the toes with an antiseptic solution (e.g., povidone-iodine or chlorhexidine gluconate). Sterile draping isolates the operative field.
- Foot Positioning: The foot is positioned in slight dorsiflexion and eversion, often with a bump or sandbag placed under the ipsilateral hip to allow for easier access to the posteromedial aspect of the ankle and foot. This positioning helps open the surgical field and relax the FDL tendon for optimal exposure.
Detailed Surgical Approach / Technique
The primary goal of FDL debridement is to remove inflamed synovium, degenerate tendon tissue, and any sources of mechanical impingement, while preserving tendon integrity and function.
Surgical Approach: Posteromedial Incision
- Incision Planning: A curvilinear longitudinal incision is typically employed along the posteromedial aspect of the ankle, centered posterior to the medial malleolus. The incision usually starts approximately 2-3 cm proximal to the medial malleolus, curves gently around its posterior aspect, and extends distally for 5-7 cm, often ending just proximal to the navicular tuberosity. The length can be adjusted based on the anticipated extent of pathology identified pre-operatively. Careful planning is made to avoid the greater saphenous vein and saphenous nerve.
-
Skin and Subcutaneous Dissection:
- Incise the skin with a No. 15 blade.
- Carefully dissect through the subcutaneous fat. Identify and protect the saphenous vein and saphenous nerve , which typically lie anterior to the incision line, but can be variable. Retract them gently.
- Deep Fascia Incision: The deep fascia is incised longitudinally. This exposes the flexor retinaculum, which forms the roof of the tarsal tunnel.
-
Identification of Tendons and Neurovascular Bundle:
- Incise the flexor retinaculum longitudinally. This exposes the contents of the tarsal tunnel.
- The tibialis posterior tendon (PTT) is usually the most anterior structure encountered, lying directly against the tibia/medial malleolus.
- Deep and slightly posterior to the PTT lies the FDL tendon .
- Posterior and superficial to the FDL tendon, and often more posterior within the tarsal tunnel, is the posterior tibial neurovascular bundle (tibial nerve, posterior tibial artery, venae comitantes). This bundle is extremely vulnerable and must be protected. Gentle retraction using vessel loops or blunt retractors is critical.
- The flexor hallucis longus (FHL) tendon lies most laterally within the tarsal tunnel, deep to the neurovascular bundle, and is usually not directly exposed unless the incision is more extensive or pathology dictates.
FDL Tendon Sheath Exploration and Debridement
- Tendon Sheath Incision: Once the FDL tendon is clearly identified, its synovial sheath is incised longitudinally along its length, typically on its anterior or superficial aspect, to expose the tendon. This tenosynovectomy can be performed sharply with a scalpel or tenotomy scissors.
- Synovial Debridement: The inflamed, hypertrophic, or scarred synovium is carefully excised using fine rongeurs, curettes, or a motorized shaver. Complete tenosynovectomy is performed to remove all pathologic tissue and reduce the likelihood of recurrence.
-
Tendon Assessment:
Thoroughly inspect the FDL tendon for signs of tendinopathy:
- Color changes: Loss of normal glistening white appearance, yellowish or grey discoloration.
- Thickening or Nodularity: Focal areas of hypertrophy or myxoid degeneration.
- Fraying or Degeneration: Longitudinal tears, surface irregularities, or areas of compromised integrity.
- Partial Tears: Assess the extent and depth of any partial tears.
-
Tendon Debridement:
- Debridement of Degenerate Tissue: Using a small, sharp scalpel (e.g., #15 blade) or rongeurs, carefully debride any visibly degenerate, hypertrophic, or unhealthy tendon tissue. The goal is to remove pathologic tissue while preserving as much healthy tendon as possible. Be conservative to avoid weakening the tendon excessively.
- Smoothing Frayed Edges: Smooth any frayed edges with a scalpel to prevent further irritation or tearing.
- Addressing Partial Tears: For minor longitudinal partial tears, simple debridement of the unhealthy tissue may suffice. Larger, more significant partial tears may require longitudinal repair with fine non-absorbable sutures (e.g., 4-0 Ethibond) to prevent propagation, though this transitions beyond simple debridement into repair. For the context of this document focused on debridement, extensive repair is not the primary intervention.
- Impaction/Impingement Release: Explore the entire exposed FDL course for any areas of impingement, particularly at the sustentaculum tali or where it crosses the FHL. Release any restricting fibrous bands or osteophytes that may be impinging the tendon.
- Irrigation: Copiously irrigate the surgical site with sterile saline to remove debris.
-
Adjunctive Procedures (Optional but relevant for context):
- While the primary focus is debridement, in some cases of severe degeneration or concomitant pathology (e.g., PTTD Stage II), an FDL tendon transfer might be considered for augmentation of the PTT. If a transfer is planned, the tendon is usually harvested distally and rerouted. This is a distinct procedure from isolated debridement.
- Concomitant nerve decompression (e.g., tarsal tunnel release) may be performed if there is documented nerve entrapment.
Closure
- Sheath Closure (Optional): The synovial sheath is typically left open or loosely closed, especially if significant edema or hypertrophy was present, to prevent recurrence of impingement. If closed, use fine absorbable sutures (e.g., 5-0 Vicryl).
- Retinaculum Closure: The flexor retinaculum may be loosely approximated or left open, depending on the need for decompression and surgeon preference.
- Fascial Closure: Close the deep fascia with absorbable sutures (e.g., 2-0 or 3-0 Vicryl).
- Subcutaneous Closure: Close the subcutaneous layer with interrupted absorbable sutures (e.g., 3-0 or 4-0 Vicryl).
- Skin Closure: Close the skin with non-absorbable sutures (e.g., 3-0 or 4-0 Nylon) or staples.
- Dressing and Splint: Apply a sterile dressing. A posterior splint or CAM boot is typically applied in slight plantarflexion to reduce tension on the FDL and protect the surgical site.
Complications & Management
While FDL debridement is generally safe, potential complications exist, necessitating vigilant post-operative monitoring and prompt management.
| Complication | Incidence | Salvage Strategies / Management |
|---|---|---|
| Infection | 1-5% | Superficial: Oral antibiotics based on culture (if possible), local wound care, close monitoring. Deep: Surgical debridement, IV antibiotics (often prolonged), hardware removal if applicable, consultation with infectious disease specialist. |
| Wound Healing Issues | 5-10% | Dehiscence/Necrosis: Strict wound care, dressing changes, avoidance of tension. May require secondary closure, local flap, or skin grafting in severe cases. Scar Hypersensitivity/Hypertrophy: Scar massage, silicone sheeting, desensitization therapy, steroid injections for hypertrophic scars. |
| Nerve Injury | Variable (2-8%) | Saphenous Nerve: Sensory deficits along medial ankle/foot. Usually transient neuropraxia, managed with observation, NSAIDs. Persistent neuroma may require local injections, nerve block, or surgical excision/neurolysis. Posterior Tibial Nerve: Sensory and/or motor deficits (toe flexion, plantar intrinsic muscles). Acute injury may require exploration and primary repair/grafting. Chronic irritation/entrapment may necessitate formal tarsal tunnel release, pain management. |
| Residual Pain / Recurrence | 5-15% | Incomplete Debridement: Revision surgery for further debridement or release. Progression of Tendinopathy: Further conservative management (PT, orthotics), biological augmentation (e.g., PRP), or repeat debridement. Undiagnosed Concomitant Pathology: Re-evaluation to identify other pain generators (e.g., spring ligament, PTTD, tarsal tunnel syndrome). Referred Pain: Address contributing spinal or hip pathology. |
| Tendon Rupture | <1% | Very rare after debridement alone, more common with aggressive debridement or prior severe degeneration. May require primary tendon repair (if acute and viable), or FDL transfer from another donor tendon, or fusion if repair is not feasible and toe function is severely compromised. |
| Stiffness / Adhesions | 5-10% | Early supervised physical therapy emphasizing range of motion. Scar massage. Manipulations under anesthesia. Tenolysis (surgical release of adhesions) in refractory cases. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Early recognition is key. Aggressive multidisciplinary pain management (medications, nerve blocks, physical therapy focused on desensitization and graded motor imagery), psychological support. Consultation with pain specialist. |
| Over-Debridement / Tendon Weakness | Rare | Careful intraoperative assessment is critical to avoid excessive tissue removal. If symptomatic weakness occurs, non-operative strengthening. Severe cases may require augmentation (e.g., FDL transfer) or tendon grafting, though this is an extreme measure for a typically minor procedure. |
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is crucial for optimizing outcomes, restoring function, and preventing recurrence after FDL debridement. The protocol must be individualized based on the extent of debridement, any concomitant procedures, and patient-specific factors.
Phase 1: Protection and Early Healing (Weeks 0-2)
- Goal: Protect surgical site, control pain and swelling, promote initial healing.
- Weight Bearing: Non-weight bearing (NWB) with crutches in a posterior splint or CAM boot.
-
Activity:
- Strict elevation of the limb.
- Ice application for 20 minutes, several times a day.
- Gentle ankle pumps (dorsiflexion/plantarflexion) without resisted toe flexion to promote circulation and prevent stiffness (ensure FDL remains relaxed).
- Wound care as directed by surgeon.
- Precautions: Avoid active or resisted toe flexion, excessive passive stretching of the toes, or any activity that puts tension on the FDL.
- Medications: Analgesics, NSAIDs (if not contraindicated), potentially short course of antibiotics.
Phase 2: Gradual Mobilization and Controlled Loading (Weeks 2-6)
- Goal: Initiate gentle range of motion, controlled weight bearing, begin scar management.
-
Weight Bearing:
- Weeks 2-4: Progress to partial weight bearing (PWB) in CAM boot as pain allows.
- Weeks 4-6: Progress to full weight bearing (FWB) in CAM boot.
-
Activity:
- Range of Motion: Begin gentle active and passive ankle range of motion (dorsiflexion, plantarflexion, inversion, eversion). Start gentle active and passive toe flexion/extension (non-resisted initially).
- Scar Management: Once incision is well-healed, begin gentle scar massage to prevent adhesions.
- Strengthening (Isometric): Isometric ankle exercises (plantarflexion, dorsiflexion, inversion, eversion) without engaging FDL significantly .
- Precautions: Continue to avoid aggressive resisted toe flexion or activities placing excessive stress on the FDL. Continue wearing CAM boot for protection.
Phase 3: Progressive Strengthening and Functional Training (Weeks 6-12)
- Goal: Restore strength, improve proprioception, prepare for return to daily activities.
- Weight Bearing: Transition out of CAM boot to supportive lace-up shoes (e.g., athletic shoes).
-
Activity:
-
Strengthening:
- Progressive resisted toe flexion exercises (e.g., towel crunches, marbles pickup, thera-band).
- Calf raises (bilateral progressing to unilateral).
- Balance and proprioception exercises (e.g., wobble board, single leg stance).
- Closed-chain exercises (mini-squats, lunges).
- General ankle strengthening.
- Cardiovascular: Stationary cycling, swimming (once incision is fully healed).
-
Strengthening:
- Precautions: Listen to pain, avoid sudden increases in activity intensity or duration.
Phase 4: Advanced Activity and Return to Sport (Weeks 12+)
- Goal: Return to full activity, including sport-specific training.
-
Activity:
- Sport-Specific Training: Gradually introduce activities mimicking desired sports or work demands.
- Plyometrics: Begin low-impact plyometrics, gradually progressing intensity.
- Running Progression: Initiate walk-to-run program, progressing mileage and speed as tolerated.
- Maintenance: Continue FDL and general lower extremity strengthening.
-
Return to Play Criteria:
- Full pain-free range of motion.
- Symmetrical strength (at least 90% compared to contralateral limb).
- Absence of swelling or tenderness.
- Successful completion of sport-specific drills without pain.
- Precautions: Gradual progression is key. Any recurrence of pain warrants rest and re-evaluation. Long-term use of supportive footwear or orthotics may be beneficial. Full return to demanding activities (e.g., competitive running, dancing) can take 4-6 months or longer.
Summary of Key Literature / Guidelines
The literature specifically addressing isolated FDL debridement for chronic foot pain is less robust than for more common tendon pathologies. Often, FDL debridement or tenosynovectomy is performed as part of a larger procedure, particularly in the context of posterior tibial tendon dysfunction (PTTD) repair or reconstruction.
- Level of Evidence: Most of the evidence supporting FDL debridement for tenosynovitis or tendinopathy comes from retrospective case series or expert opinion, rather than high-level prospective randomized controlled trials. This reflects the relative rarity of isolated, severe FDL pathology requiring surgery compared to, for example, Achilles tendinopathy.
- Diagnostic Accuracy: Imaging, particularly MRI, plays a critical role in confirming FDL pathology and differentiating it from other causes of posteromedial ankle pain. Studies emphasize the importance of clinical correlation with imaging findings to ensure accurate diagnosis. Ultrasound has also emerged as a useful dynamic diagnostic tool.
- Conservative Management: The consensus across orthopedic literature strongly advocates for a comprehensive trial of non-operative management (rest, NSAIDs, activity modification, physical therapy, orthotics, injections) for at least 3-6 months before considering surgical intervention for FDL pathology.
- Surgical Efficacy: When conservative measures fail, surgical debridement and tenosynovectomy of the FDL have been reported to achieve good to excellent results in reducing pain and improving function, particularly in cases of clear, focal pathology (e.g., severe tenosynovitis with hypertrophic synovium, localized tendinosis). The success is highly dependent on accurate diagnosis and careful patient selection.
- Role in PTTD: In Stage II PTTD, FDL transfer is a well-established procedure to augment the incompetent PTT. During this procedure, any coexisting FDL tenosynovitis or tendinopathy is typically addressed with debridement. The outcomes in these combined procedures are generally favorable, with FDL providing robust power for transfer.
- Comparison to Minimally Invasive Techniques: While arthroscopic or endoscopic techniques have gained traction for other tendon pathologies (e.g., FHL tenosynovitis), dedicated minimally invasive approaches for FDL debridement are less common and less well-described in the literature. Open debridement remains the standard, offering superior visualization and control for thorough pathology removal and neurovascular protection.
- Long-Term Outcomes: Long-term studies focusing solely on FDL debridement are scarce, but clinical experience suggests that if the primary pathology is addressed, outcomes are durable. Recurrence is possible, particularly if underlying biomechanical factors or systemic conditions are not managed.
In summary, debridement of the flexor digitorum longus tendon and its sheath is a viable and effective solution for carefully selected patients with chronic, refractory FDL tenosynovitis or tendinopathy. It is most successful when part of a meticulous diagnostic workup and a structured post-operative rehabilitation program. While robust high-level evidence is limited for isolated FDL debridement, existing data and clinical experience support its role in the surgical armamentarium for specific causes of chronic foot pain.
