INTRODUCTION TO BLADDER EXSTROPHY
Exstrophy of the bladder represents a profound failure of embryological development, characterized by a congenital failure of fusion of the midline tissues of the pelvis and lower abdomen. The primary anomaly is a severe maldevelopment of the lower abdominal wall and the anterior wall of the bladder. Consequently, the anterior surface of the posterior wall of the bladder is exposed directly to the exterior environment.
While the most visually striking and functionally critical aspects of this condition are urological and gastrointestinal, the orthopaedic manifestations are equally profound. Hernias and other structural defects of the anterior abdominal wall are frequently present more proximally. The orthopaedic surgeon becomes an indispensable member of the multidisciplinary treatment team primarily due to the severe diastasis of the symphysis pubis and the pronounced lateral flare of the innominate bones.

Fig. 27-37 A: Congenital exstrophy of the bladder in a newborn boy, demonstrating the exposed bladder mucosa and lower abdominal wall defect.
Without orthopaedic intervention to reconstruct the pelvic ring, the urological surgeon faces insurmountable tension when attempting to close the bladder and abdominal wall. Failure to achieve a tension-free closure inevitably leads to wound dehiscence, bladder prolapse, and failure of the bladder neck reconstruction, which is critical for future urinary continence.
PATHOMECHANICS AND PELVIC DEFORMITY
Understanding the 3D pathoanatomy of the exstrophic pelvis is paramount for successful surgical reconstruction. The deformity is not merely a simple separation of the pubic bones; it is a complex, multiplanar rotational anomaly of the entire pelvic ring.
Key Anatomical Alterations
- Pubic Diastasis: The symphysis pubis is widely separated, often by several centimeters, creating a massive anterior defect.
- External Rotation of the Hemipelves: The iliac wings are flared outward (externally rotated) relative to the sacroiliac joints. The sacroiliac joints themselves are typically morphologically normal but act as the hinge point for this external rotation.
- Acetabular Retroversion: Due to the external rotation of the hemipelves, the acetabula are retroverted. While this rarely causes frank hip dislocation, it contributes to the characteristic "waddling" gait seen in uncorrected older children.
- Shortened Pubic Rami: The superior and inferior pubic rami are structurally shorter than in a normal pelvis, meaning that even with perfect rotational correction, a small anterior gap may persist.

Fig. 27-37 B: Preoperative anteroposterior radiograph of a 1-year-old child demonstrating severe pubic diastasis and lateral flare of the iliac wings.
Clinical Pearl: The primary goal of orthopaedic intervention is not to create a radiographically perfect pelvis, but rather to provide a mechanically stable, tension-free environment for the urologist to perform a secure closure of the bladder, bladder neck, and abdominal wall.
INDICATIONS AND TIMING FOR OSTEOTOMY
Historically, some neonates treated within the first 48 to 72 hours of life underwent primary closure without osteotomy, relying on the residual elasticity of maternal relaxin. However, modern consensus heavily favors concomitant pelvic osteotomies for nearly all cases, as it significantly decreases the risk of dehiscence and improves long-term continence rates.
Absolute Indications for Pelvic Osteotomy:
* Infants older than 72 hours at the time of primary closure.
* Any patient undergoing a re-closure following a previous dehiscence or failure.
* Pubic diastasis exceeding 4 cm in a newborn.
* Classic bladder exstrophy or cloacal exstrophy variants requiring complex abdominal wall reconstruction.
SURGICAL APPROACHES TO THE EXSTROPHIC PELVIS
Several osteotomy techniques have been described historically, including bilateral posterior iliac osteotomies.

Fig. 27-37 C: Postoperative radiograph demonstrating an older technique utilizing bilateral posterior iliac osteotomies and anterior reconstruction.
While posterior osteotomies were once popular, they require flipping the patient intraoperatively and often fail to provide the necessary rotational mobility of the anterior ring. Today, the gold standard is the Bilateral Anterior Iliac Osteotomy, popularized by Sponseller, Gearhart, and Jeffs. This technique allows for simultaneous exposure, excellent mobilization of the anterior segment, and the ability to perform the entire procedure in the supine position.
SURGICAL TECHNIQUE: BILATERAL ANTERIOR ILIAC OSTEOTOMIES (Sponseller, Gearhart, and Jeffs)
This technique utilizes bilateral Salter-type innominate osteotomies to free the ischiopubic segments, allowing them to be rotated medially to close the anterior defect.
1. Positioning and Preparation
- Place the patient supine on a radiolucent operating table.
- Elevate the sacrum on folded towels or a small gel pad. This elevation is critical as it allows the mobilized iliac segments to drop posteriorly during medial rotation, facilitating the closure of the anterior ring.
- Circumferentially prepare and drape the entire body from the costal margin down to the toes. The legs must be draped free to allow for intraoperative manipulation.
2. Surgical Approach
- Utilize an anterior iliofemoral approach (Smith-Petersen type) to the pelvis. This is identical to the approach used for a standard Salter innominate osteotomy.
- Both sides can be exposed simultaneously by a two-surgeon team to minimize operative time.
- Incise the skin along the anterior iliac crest, extending distally toward the anterior superior iliac spine (ASIS).
- Develop the interval between the tensor fasciae latae and the sartorius.
- Protect the Lateral Femoral Cutaneous Nerve (LFCN), which may have an aberrant course in these dysplastic pelves.
3. Subperiosteal Exposure
- Widely expose the medial and lateral cortices of the ilium.
- Carefully elevate the periosteum posteriorly around the greater sciatic notch. Use curved elevators and gauze sponges to gently sweep the tissues.
- Pass a right-angle clamp or a specialized sciatic notch retractor through the notch from medial to lateral.
Surgical Warning: Dissection within the sciatic notch must be strictly subperiosteal. Straying from the bone places the superior gluteal artery and the sciatic nerve at high risk of iatrogenic injury.
4. Executing the Osteotomy
- The osteotomy is designed to separate the upper ilium from the lower ischiopubic segment.
- Make the osteotomy cut starting 5 mm above the anterior inferior iliac spine (AIIS) and direct it to the most cranial portion of the greater sciatic notch. This specific trajectory leaves a sizable, robust inferior segment necessary for subsequent internal fixation.
- Instrument Selection Based on Age:
- Children > 6 months: A Gigli saw is highly effective. If difficult to pass, thread it through the notch using a leader of umbilical tape.
- Infants < 6 months: Use an oscillating saw. The force applied by a Gigli saw in a very young infant can cause preferential, iatrogenic separation of the triradiate cartilage rather than cutting the bone.
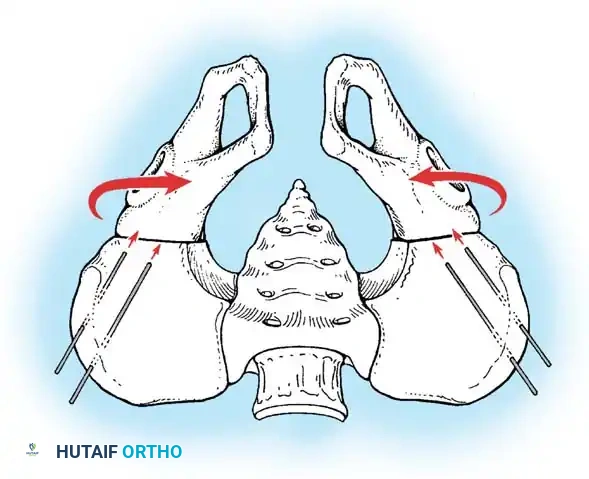
Fig. 27-38 A: Diagrammatic representation of the bilateral anterior Salter innominate osteotomies. The red arrows indicate the medial rotation of the freed ischiopubic segments to close the symphyseal gap. Note the pin placement for external fixation.
5. Mobilization and Rotation
- Once the osteotomies are complete bilaterally, grasp the distal fragments with a towel clip or bone holding forceps.
- Rotate the freed ischiopubic segments 30 to 45 degrees medially. This maneuver brings the pubic rami together in the midline.
6. Application of Fixation Pins
External fixation is the preferred method of stabilization, providing rigid support while avoiding hardware in the contaminated anterior urological field.
* Pin Sizing:
* Children > 6 months: 2-mm pins.
* Children 4 to 10 years: 4-mm pins.
* Children > 10 years: 5-mm pins.
* Insert two pins into each intact proximal iliac wing and two pins into each mobilized distal fragment.
* Predrilling is highly recommended in small infants to prevent splitting the fragile cortical bone.
* Distal Pin Placement (Critical Step):
* Place the first distal fragment pin starting from the AIIS, directing it toward the sciatic notch. It must run parallel to, and 5 to 10 mm inferior to, the osteotomy line. Ensure this pin engages the dense, deep posterior cortex of the notch for maximum pull-out strength.
* Insert the second threaded pin just below the first, but angle it externally by 30 degrees to create a divergent, biomechanically stable construct.
7. Urological Phase and Anterior Closure
- At this stage, the orthopaedic team steps back, and the urological surgeon prepares the operative field to identify the abnormal bladder and urethral structures, performing the necessary visceral reconstruction.
- Once the urologist is ready for abdominal closure, the orthopaedic surgeon returns to close the pelvic ring.
- Use a single, heavy suture (e.g., #2 or 2-0 nylon) in a horizontal mattress stitch to approximate the pubic bones.
- Tie this suture anterior to the neourethra and bladder neck.
- Crucial Maneuver: While the knot is being tied, an assistant must forcefully rotate the greater trochanters medially. This removes all tension from the suture line, allowing the bones to meet without tearing through the cartilage.
- Place heavy sutures of polyglactin (Vicryl) in the rectus fascia just superficial to the pubic closure to reinforce the anterior wall.
8. Finalizing Fixation
- After the pelvic ring is securely closed anteriorly, assemble and tighten the external fixator bar connecting the pins.
- Verify that the fixator construct is rigid and that the skin is not under tension around the pin sites.

Fig. 27-38 B: Postoperative anteroposterior radiograph demonstrating successful closure of the pubic diastasis following bilateral anterior Salter innominate osteotomies and application of an external fixator.
Alternative Fixation (Spica Cast)
In environments where external fixation is unavailable, or in specific surgeon preferences, the procedure can be modified. The osteotomies can be stabilized with heavy Kirschner wires (K-wires) driven across the osteotomy sites, followed by the application of a rigid bilateral hip spica cast. The cast must be worn for 8 to 12 weeks. However, external fixation remains the superior choice for wound care and nursing management.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative phase is critical to prevent loss of reduction and hardware failure. The reconstructed pelvis is under immense biomechanical stress due to the natural tendency of the pelvic ring to spring open.
Immediate Postoperative Care
- Immobilization: Light Buck traction or a modified spica cast can be utilized for the first 1 to 2 weeks to maintain strict bed rest, control pain, and prevent sudden movements that could compromise the fixation.
- Infant Considerations: Strict bed rest and traction are mandatory in children younger than 1 year old. Their bones have relatively less cortical density, making pin pull-out a significant risk if they are allowed to move freely.
- Older Children: If excellent, rigid external fixation is achieved, older children can be mobilized to a wheelchair and discharged from the hospital earlier.
Fixator Management and Removal
- Duration of Fixation:
- Children younger than 2 years: The external fixator is maintained for 4 weeks.
- Children older than 2 years: The external fixator is maintained for 6 weeks.
- Pin site care must be performed daily using chlorhexidine or half-strength hydrogen peroxide to prevent superficial infections, which are common given the proximity to the urostomy/diaper region.
Rehabilitation
- Following fixator removal, a gradual resumption of activities is permitted.
- No formal, aggressive physical therapy program is typically necessary, as children will naturally resume weight-bearing as their comfort allows.
- A pediatric walker is highly recommended during the first 1 to 2 weeks of ambulation in older children to provide stability as they adjust to their new pelvic biomechanics and altered center of gravity.
COMPLICATIONS AND PITFALLS
Orthopaedic surgeons must be vigilant regarding several potential complications specific to this complex reconstruction:
- Loss of Reduction / Recurrent Diastasis: The most common complication. Often results from inadequate medial rotation of the fragments, premature removal of the external fixator, or pin pull-out due to poor bone purchase.
- Pin Tract Infections: Given the anatomical location, contamination from urine or feces is a high risk. Aggressive local wound care and early oral antibiotics for erythema are required. Deep infections necessitating premature pin removal are catastrophic for the reconstruction.
- Nerve Injury: The sciatic nerve is at risk during the subperiosteal dissection of the greater sciatic notch. The lateral femoral cutaneous nerve is at risk during the anterior approach.
- Triradiate Cartilage Injury: As noted, using a Gigli saw in infants under 6 months can shear the triradiate cartilage, leading to premature closure and severe acetabular dysplasia later in life. Always use an oscillating saw in this age group.
- Delayed Union / Nonunion: While rare in the pediatric population, inadequate apposition of the osteotomy surfaces can lead to delayed healing, requiring prolonged immobilization.
By adhering strictly to the biomechanical principles of the anterior innominate osteotomy and maintaining meticulous postoperative care, the orthopaedic surgeon provides the foundation upon which the urological team can successfully reconstruct the exstrophic bladder, profoundly altering the patient's quality of life.
📚 Medical References
- bladder exstrophy: a biomechanical analysis, J Pediatr Orthop 20:296, 2000.
- Jones D, Parkinson S, Hosalkar HS: Oblique pelvic osteotomy in the exstrophy/epispadias complex, J Bone Joint Surg 88B:799, 2006.
- Kantor R, Salai M, Ganel A: Orthopaedic long-term aspects of bladder exstrophy, Clin Orthop Relat Res 335:240, 1997.
- Kasat LS, Borwankar SS: Factors responsible for successful primary closure in bladder exstrophy, Pediatr Surg Int 16:194, 2000.
- Loder RT, Dayioglu MM: Association of congenital vertebral malformations with bladder and cloacal exstrophy, J Pediatr Orthop 10:389, 1990.
- Okubadejo GO, Sponseller PD, Gearhart JP: Complications in orthopedic management of exstrophy, J Pediatr Orthop 23:522, 2003.
- O’Phelan EH: Iliac osteotomy in exstrophy of the bladder, J Bone Joint Surg 45A:1409, 1963.
- Satsuma S, Kobayashi D, Yoshiya S, et al: Comparison of posterior and anterior pelvic osteotomy for bladder exstrophy complex, J Pediatr Orthop B 15:141, 2006.
- Sponseller PD, Gearhart JP, Jeffs RD: Anterior innominate osteotomies for failure or late closure of bladder exstrophy, J Urol 146:137, 1991.
- Sponseller PD, Jani MM, Jeffs RD, et al: Anterior innominate osteotomy in repair of bladder exstrophy, J Bone Joint Surg 83A:184, 2001.
- Yazici M, Kandermi U, Atilla B, et al: Rotational profi le of lower extremities in bladder exstrophy patients with unapproximated pelvis: a clinical and radiologic study in children older than 7 years, J Pediatr Orthop 19:531, 1999.
- Yazici M, Sozubir S, Kilicoglu G, et al: Three-dimensional anatomy of the pelvis in bladder exstrophy: description of bone pathology by using three-dimensional computed tomography and its clinical relevance, J Pediatr Orthop 18:132, 1998.
