Introduction to Elbow Dislocation and Instability
Acute dislocation of the elbow occurs relatively frequently, accounting for approximately 28% of all injuries to the elbow joint. Elbow dislocation is typically a high-energy episode associated with severe soft-tissue injury, and residual loss of motion is a common postoperative or post-injury complication. While recurrent dislocation of the elbow is relatively rare—usually occurring in the posterior direction—persistence of posterolateral or medial instability is far more common. Linscheid and Wheeler, in a classic series of 110 elbow dislocations, found only two recurrent cases. However, subtle, chronic instability patterns, particularly in overhead athletes or following inadequate healing of the lateral ligamentous complex, require meticulous clinical evaluation. When symptomatic, these instability patterns must be surgically corrected in appropriate patients to prevent progressive articular degeneration.
Surgical Anatomy and Biomechanics
A profound understanding of the osseous and ligamentous anatomy is paramount for diagnosing and treating elbow instability. The elbow is a highly constrained hinge joint, relying on a complex interplay between its bony architecture and capsuloligamentous restraints.
The Lateral Collateral Ligament Complex
The lateral collateral ligament (LCL) of the elbow arises from the lateral epicondyle and inserts on the annular ligament. A distinct and critical band of the lateral ligamentous complex, the lateral ulnar collateral ligament (LUCL), arises at the lateral epicondyle, blends with the fibers of the annular ligament, and inserts on the supinator crest of the ulna.
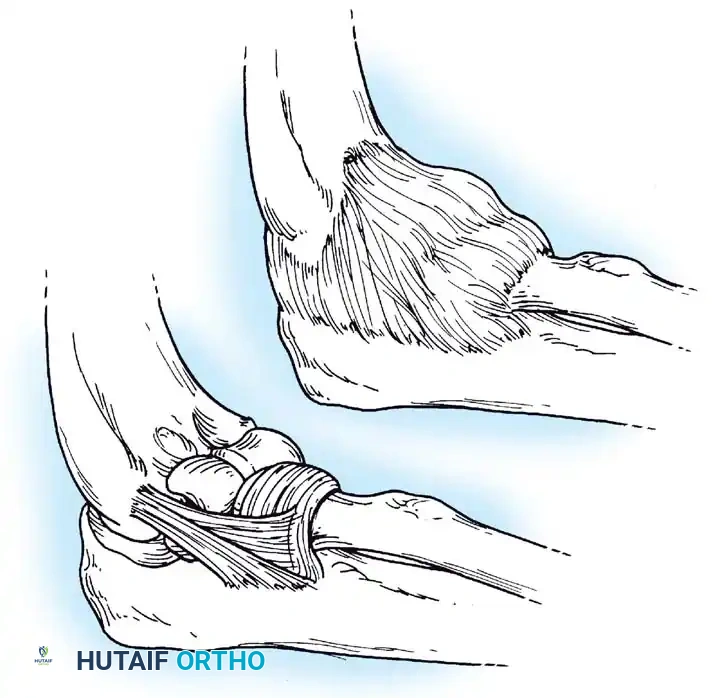
Morrey described the LUCL as the primary lateral stabilizer of the elbow, remaining taut in both flexion and extension. Disruption of this specific portion of the lateral complex results in posterolateral rotatory instability (PLRI), a kinematic abnormality elegantly described by O’Driscoll, Bell, and Morrey.
Biomechanically, Morrey and An have demonstrated that the lateral collateral ligament contributes only 14% of the varus stability of the elbow with the joint in full extension, and only 9% with the joint in 90 degrees of flexion. The remainder of varus stability is conferred by the highly congruent bony articular surfaces and the anterior capsule, with the osseous articulation supplying the vast majority of the restraint. The radial collateral ligament is primarily effective in extension to resist varus stress.
The Medial Collateral Ligament Complex
The medial collateral ligament (MCL), or ulnar collateral ligament (UCL), is a robust, well-developed structure. Tullos et al. anatomically divided it into three distinct portions: the anterior oblique, posterior oblique, and transverse bundles.
In stark contrast to the lateral collateral ligament, the MCL plays a dominant role in valgus stability. Valgus stability is divided equally among the medial collateral ligament, the anterior capsule, and the bony articulation when the elbow is in full extension. However, at 90 degrees of flexion, the medial collateral ligament provides a staggering 55% of the stability to valgus stress.
Clinical Pearl: The anterior oblique bundle is the primary soft-tissue stabilizer of the elbow against valgus and distraction stress. It is the most critical structure to evaluate in overhead throwing athletes presenting with medial elbow pain.
Pathophysiology of Elbow Instability
The etiology of recurrent dislocation or instability of the elbow varies, but it almost always stems from two basic abnormalities:
1. The trochlear notch of the ulna is misshapen (congenital or traumatic).
2. The collateral ligaments that should stabilize the elbow are incompetent.
Traumatic and Congenital Factors
If congenital, the trochlear notch may be excessively shallow or abnormal in contour. If traumatic, recurrent dislocation may result from fractures or severe ligamentous disruption. For instance, the retraction of a nonunited coronoid process fracture leaves the trochlear notch shallow anteriorly, predisposing the joint to recurrent posterior dislocation. Similarly, a nonunion or malunion of a lateral humeral condyle fracture can result in profound elbow instability.
Medial Instability and Valgus Extension Overload
Recurrent medial instability of the elbow has been extensively described by Jobe, Kvitne, Andrews, Tullos, and Morrey. This instability frequently results from microtraumatic injuries to the UCL in throwing athletes, leading to medial elbow pain and secondary ulnar nerve symptoms.
During the acceleration phase of throwing, the valgus stress applied to a pitcher’s elbow approaches the ultimate tensile failure point of the UCL. Because the MCL is the primary stabilizer when the elbow is flexed more than 30 degrees, the dynamic function of the flexor carpi ulnaris and flexor digitorum sublimis muscles is essential in preventing repeated overload.
Repeated microtraumatic injury causes inflammation, weakening, and progressive degenerative changes, often culminating in an undersurface tear (as described by Andrews and Timmerman) and eventual structural failure.
Incompetence of the UCL alters joint kinematics, leading to Valgus Extension Overload (VEO). This results in:
* Chondromalacia of the posteromedial aspect of the olecranon tip.
* Formation of posteromedial osteophytes as the olecranon impinges on the olecranon fossa.
* Chondromalacia of the radiocapitellar joint due to excessive lateral compression.
* Inflammation, scarring, and traction injuries to the ulnar nerve.
Posterolateral Rotatory Instability (PLRI)
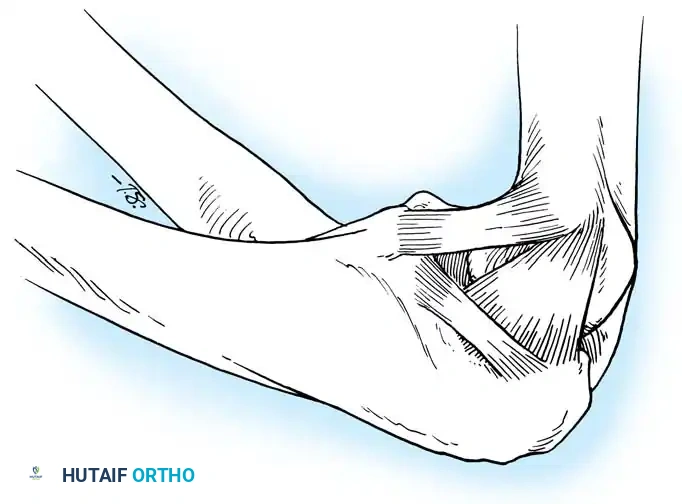
The posterolateral structures—the lateral capsule, LUCL, and radial collateral ligament—are typically injured via a hyperextension, external rotation, and valgus force mechanism, often from a fall on an outstretched hand (FOOSH).

Clinical Evaluation and Physical Examination
Examination of the elbow begins with a meticulous visual inspection for atrophy, swelling, or ecchymosis. The forearm circumference is measured 7 cm below the medial epicondyle to compare with the contralateral extremity. Joint effusion can often be detected in the "soft spot" posterolaterally (the center of the triangle formed by the lateral epicondyle, radial head, and olecranon tip).
Evaluating Medial Instability
The flexor-pronator mass, the UCL footprint, and the posteromedial olecranon tip are carefully palpated. Tenderness and swelling 2 to 3 cm distal to the olecranon tip may indicate an olecranon stress fracture.
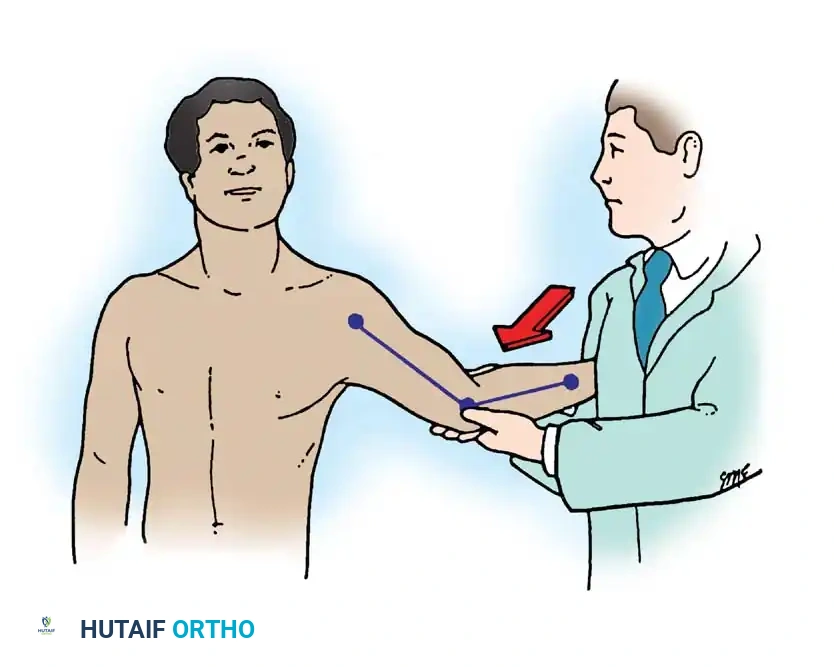
A valgus stress is applied to the elbow with the forearm in supinated and pronated positions, with the elbow unlocked at approximately 30 degrees of flexion to disengage the olecranon from its fossa. The examiner must note the amount of medial opening, the firmness of the end point, and the reproduction of medial pain.
Valgus Extension Overload Test: Maintained valgus stress is applied while the elbow is passively extended from 30 degrees to full extension. Pain along the posteromedial olecranon indicates impingement secondary to chronic instability.
Moving Valgus Stress Test (O’Driscoll): Considered highly accurate for UCL competence. With the patient’s shoulder abducted and externally rotated, a valgus stress is applied as the elbow is passively extended from 120 degrees down to 30 degrees, then flexed back rapidly. Generation of medial pain at the "shear angle" (typically between 70 and 120 degrees) indicates ligamentous incompetence.
Evaluating Posterolateral Instability
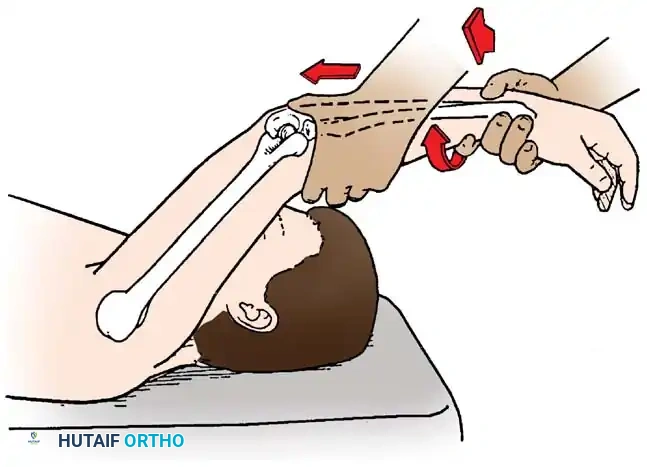
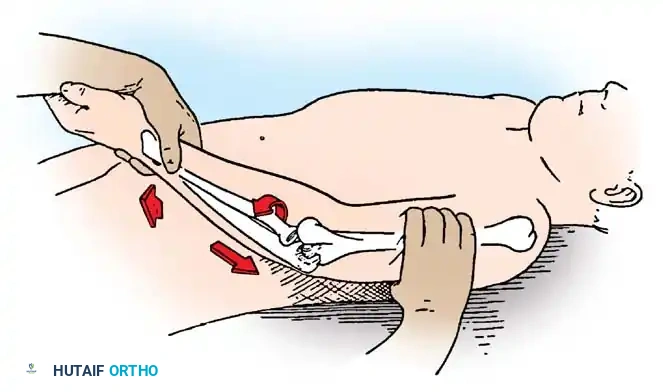
Posterolateral instability is evaluated via the Lateral Pivot-Shift Test of the Elbow. The patient is placed supine with the arm overhead. The examiner supinates the forearm and applies a valgus moment and axial compressive force while moving the elbow from extension into flexion.
As the elbow flexes past 40 degrees, the radial head subluxates posterolaterally, creating a visible prominence and a dimple in the soft spot. With further flexion, the triceps tension increases, and the radius and ulna snap back into place with a palpable "clunk."
Diagnostic Imaging
Diagnostic radiographs must include an anteroposterior (AP) view, a true lateral view, and two 45-degree oblique views to evaluate the radiocapitellar and ulnohumeral joints. In patients with chronic medial symptoms, a Jones view (acute flexion AP) is indicated to identify posteromedial olecranon osteophytes.
A gravity stress radiograph can be obtained with the patient supine, shoulder abducted 90 degrees, and externally rotated. A lateral radiograph demonstrates medial opening under gravity stress.
Currently, the gold standard for evaluating UCL integrity is a gadolinium-enhanced MRI (MR Arthrogram). Timmerman and Andrews described the "T-sign"—a leak of contrast material extending medially between the UCL and the sublime tubercle, indicating a partial undersurface tear. MRI also effectively visualizes bone bruising, chondral defects, and flexor-pronator mass pathology.
Arthroscopic Evaluation
Arthroscopy of the elbow is a powerful adjunct to confirm medial instability, remove loose bodies, and debride posteromedial osteophytes.
Surgical Warning: Elbow arthroscopy carries a high risk of neurovascular injury. Meticulous portal placement and adherence to safe zones are mandatory. The joint must be distended with fluid prior to establishing the anterolateral portal.
Andrews et al. described an arthroscopic valgus stress test performed under general anesthesia. Viewing from the anterolateral portal, valgus stress is applied with the elbow flexed to 70 degrees. An opening of the ulnohumeral joint greater than 1 to 2 mm is diagnostic of medial instability.
Surgical Management
Surgery is generally not indicated for acute, simple elbow dislocations unless the joint remains unstable after closed reduction or if dislocation recurs despite appropriate immobilization. Morrey et al. categorize acute complete dislocations as stable or unstable after reduction.
* Stable elbows: Early range of motion is indicated.
* Unstable elbows: An extension-block splint is utilized (blocking extension at 45 degrees for 1 week, 30 degrees for the next week).
When instability persists or recurs, surgical reconstruction of the medial or lateral collateral ligaments is indicated.
Indications for UCL Reconstruction (Jobe's Criteria)
- An acute complete rupture of the UCL in a competitive throwing athlete who wishes to remain active in their sport.
- Chronic medial instability that has failed a comprehensive conservative management program (minimum 3-6 months of rest, mechanics modification, and targeted rehabilitation) in a patient who wishes to return to high-level throwing.
Operative Technique: Medial Ulnar Collateral Ligament Reconstruction
1. Patient Positioning and Approach:
The patient is placed supine with the arm supported on a hand table. A tourniquet is applied high on the brachium. A medial curvilinear incision is made, centered over the medial epicondyle.
2. Ulnar Nerve Management:
The medial antebrachial cutaneous nerve branches are protected. The ulnar nerve is identified and decompressed. Depending on the surgeon's preference and the presence of preoperative ulnar neuritis, the nerve may be left in situ or transposed anteriorly (subcutaneous or submuscular).
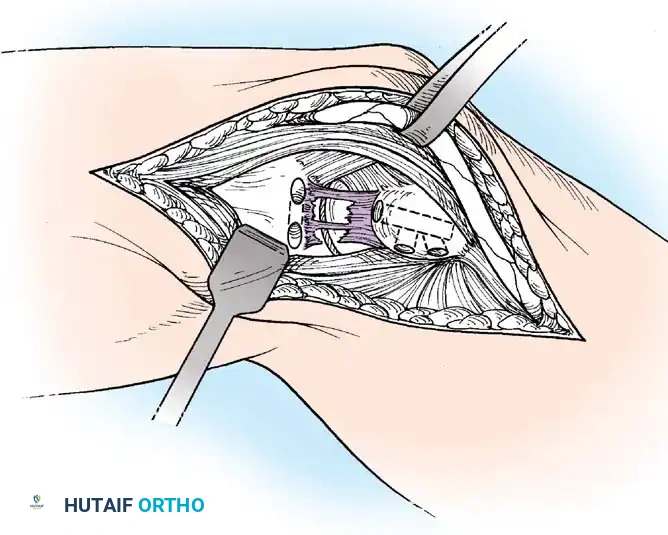
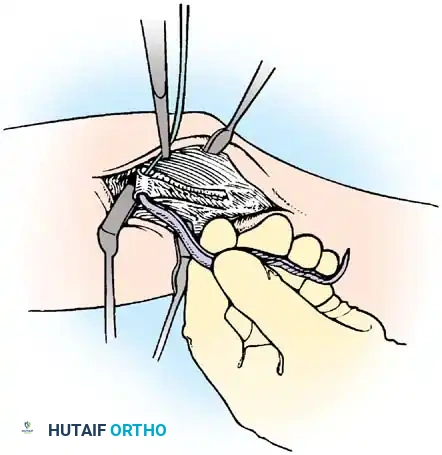
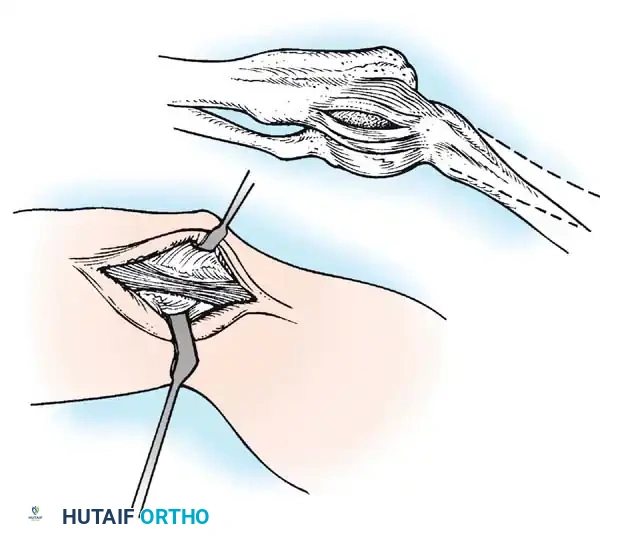
3. Exposure of the UCL:
The flexor-pronator mass is split longitudinally in line with its fibers (often between the two heads of the flexor carpi ulnaris) to expose the native UCL. The native ligament is incised longitudinally to expose the joint and inspect the articular surface.
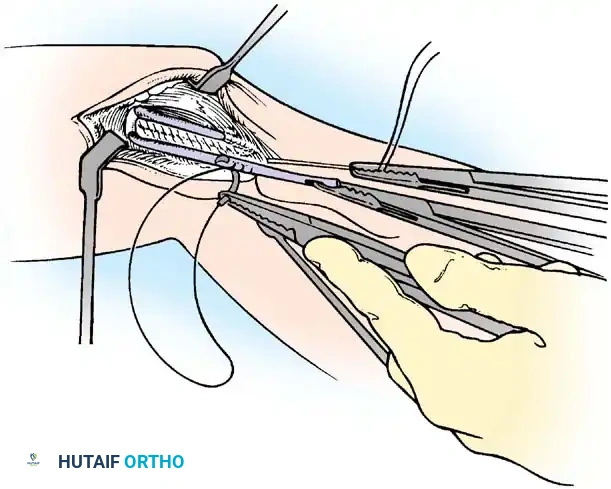
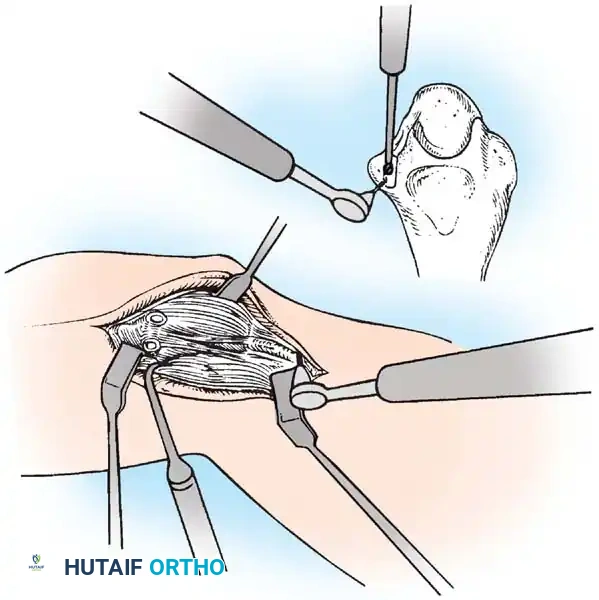
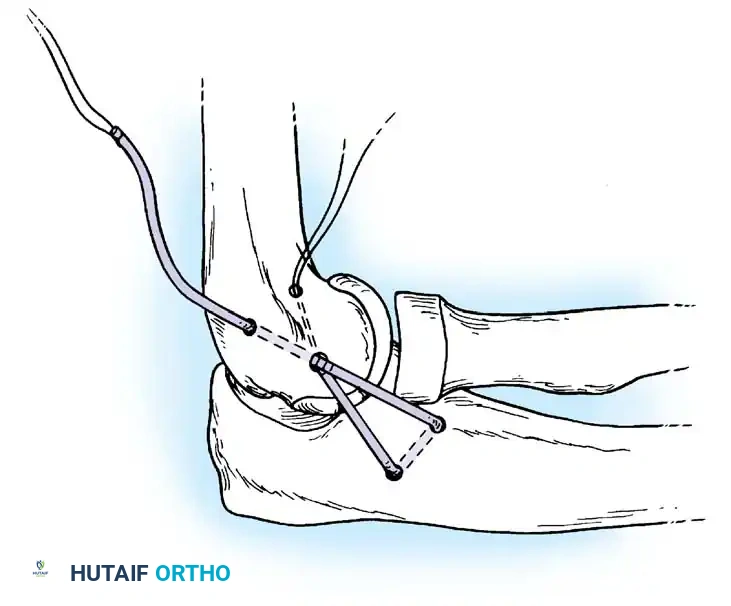
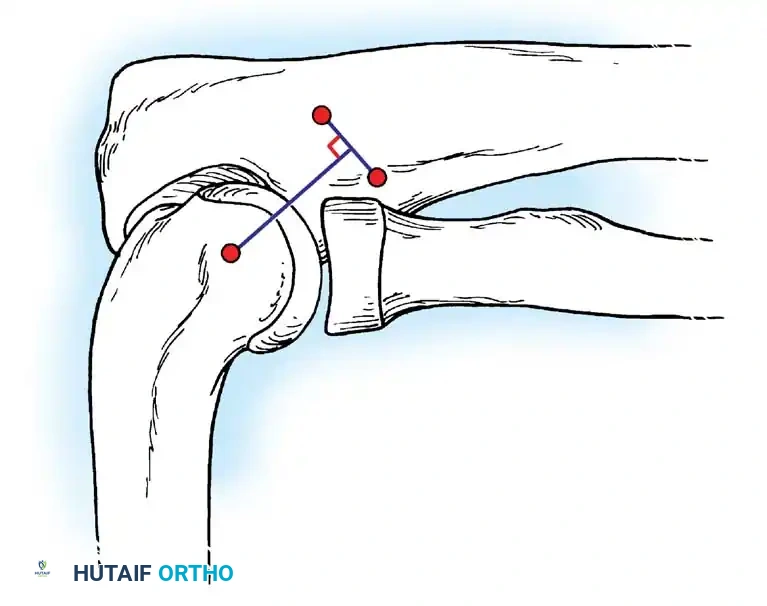
4. Tunnel Preparation:
Using a high-speed burr or drill, tunnels are created at the anatomic footprints. On the ulna, converging drill holes are made anterior and posterior to the sublime tubercle, leaving a 1 cm bone bridge. On the medial epicondyle, a Y-shaped or docking tunnel is created at the isometric point.
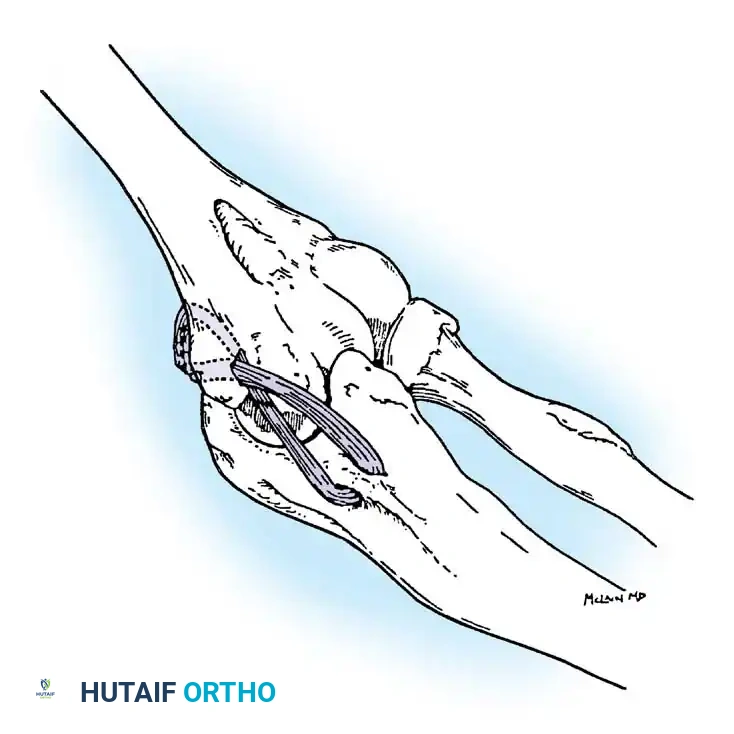
5. Graft Harvesting and Passage:
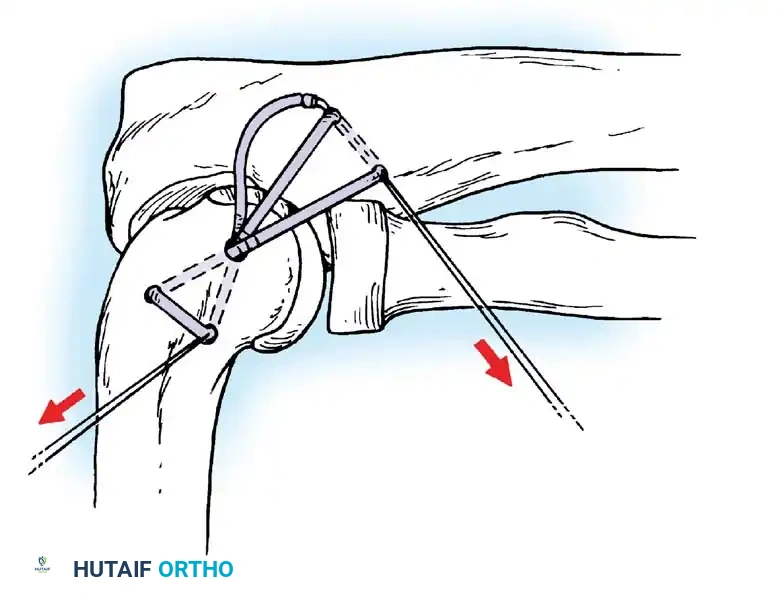
An autograft is harvested, most commonly the palmaris longus or gracilis tendon. The graft is passed through the ulnar tunnels in a figure-of-eight fashion.
6. Tensioning and Fixation:
The graft is passed into the humeral tunnel. The elbow is placed in 30 to 45 degrees of flexion, and a varus force is applied to close the medial joint space. The graft is tensioned and secured using non-absorbable sutures or an interference screw/suspensory button construct (Docking technique).
Operative Technique: Lateral Ulnar Collateral Ligament (LUCL) Reconstruction
For patients with symptomatic PLRI, LUCL reconstruction is the procedure of choice.
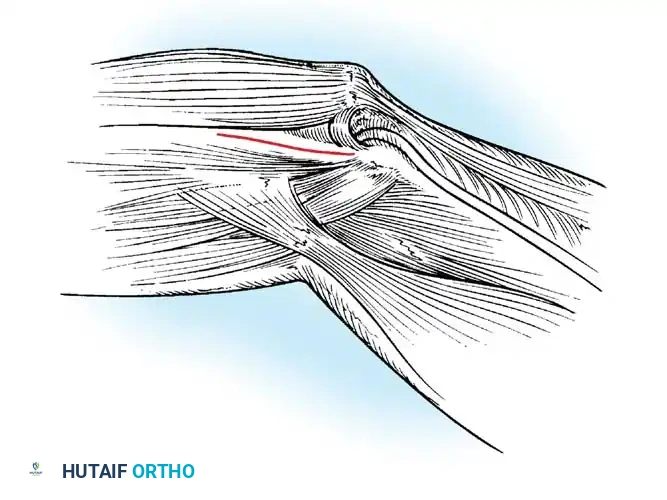
1. Approach:
A lateral Kocher approach is utilized, exploiting the internervous plane between the anconeus (radial nerve) and the extensor carpi ulnaris (posterior interosseous nerve).
2. Identifying the Isometric Point:
The common extensor origin is elevated or split to expose the lateral epicondyle and the supinator crest of the ulna. The isometric point on the lateral epicondyle is identified—this is critical to ensure the graft does not over-constrain the joint during flexion and extension.

3. Fixation:
Bone tunnels are created at the supinator crest and the lateral epicondyle. Alternatively, modern techniques utilize suture anchors at the anatomic footprints. The graft (palmaris longus or triceps fascia) is passed and tensioned with the elbow in 30 to 40 degrees of flexion and full pronation to reduce the posterolateral subluxation.
Postoperative Rehabilitation Protocol
Successful outcomes following elbow ligamentous reconstruction rely heavily on strict adherence to a phased rehabilitation protocol.
- Phase I (0-2 Weeks): The elbow is immobilized in a posterior splint at 90 degrees of flexion. For UCL reconstructions, the forearm is left in neutral; for LUCL reconstructions, the forearm is placed in pronation to protect the lateral repair.
- Phase II (2-6 Weeks): The patient is transitioned to a hinged elbow brace. Range of motion is gradually advanced. Extension is initially blocked at 30 degrees and advanced by 10 degrees weekly. Isometrics for the shoulder and wrist are initiated.
- Phase III (6-12 Weeks): The brace is discontinued. Full range of motion should be achieved. Progressive isotonic strengthening of the flexor-pronator mass (for UCL) or extensor mass (for LUCL) is emphasized.
- Phase IV (3-6 Months): Plyometric exercises and sport-specific drills begin. For throwing athletes, an interval throwing program is initiated at 4 months, with a return to competitive pitching typically expected between 9 and 12 months postoperatively.
Pitfall: Premature aggressive extension stretching can stretch out the reconstructed ligament. Extension should be regained passively through gravity and light, controlled stretching rather than forceful manipulation.
By meticulously adhering to anatomic principles, recognizing the subtle signs of microtraumatic instability, and executing precise surgical reconstruction, orthopedic surgeons can reliably restore elbow stability and return patients to their pre-injury level of function.
📚 Medical References
- elbow instability: the role of the medial collateral ligament, Clin Orthop Relat Res 146:42, 1980.
- Shuind F, O’Driscoll S, Korinek S, et al: Loose-hinge total elbow arthroplasty, J Arthroplasty 10:670, 1995.
- Implant Arthroplasty Aldridge JM III, Lightdale NR, Mallon WJ, et al: Total elbow arthroplasty with the Coonrad/Coonrad-Morrey prosthesis: a 10to 31-year survival analysis, J Bone Joint Surg 88B:509, 2006.
- Allieu Y, Meyer zu Reckendorf G, Daude O: Long-term results of unconstrained Roper-Tuke total elbow arthroplasty in patients with rheumatoid arthritis, J Shoulder Elbow Surg 7:560, 1998.
- Antuna SA, Morrey BF, Adams RA, et al: Ulnohumeral arthroplasty for primary degenerative arthritis of the elbow: longterm outcome and complications, J Bone Joint Surg 84A:2168, 2002.
- Athwal GS, Morrey BF: Revision total elbow arthroplasty for prosthetic fractures, J Bone Joint Surg 88A:2017, 2006.
- Birkedal JP, Deal DN, Ruch DS: Loss of fl exion after radial head replacement, J Shoulder Elbow Surg 13:208, 2004.
- Blaine TA, Adams R, Morrey BF: Total elbow arthroplasty after interposition arthroplasty for elbow arthritis, J Bone Joint Surg 87A:286, 2005.
- Brady O, Quinlan W: The Guildford elbow, J Hand Surg 18B:389, 1993.
- Bryan RS: Total replacement of the elbow joint, Arch Surg 112:1092, 1977.
- Burnett R, Fyfe IS: Souter-Strathclyde arthroplasty of the rheumatoid elbow, Acta Orthop Scand 62:52, 1991.
- Calfee R, Madom I, Weiss APC: Radial head arthroplasty, J Hand Surg 31A:314, 2006.
- Celli A, Arash A, Adams RA, et al: Triceps insuffi ciency following total elbow arthroplasty, J Bone Joint Surg 87A:1957, 2005.
- Chapman CB, Su BW, Sinicropi SM, et al: Vitallium radial head prosthesis for acute and chronic elbow fractures and fracturedislocations involving the radial head, J Shoulder Elbow Surg 15:463, 2006.
- Cobb TK, Morrey BF: Use of distraction arthroplasty in unstable fracture dislocations of the elbow, Clin Orthop Relat Res 312:201, 1995.
- Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for
