Dorsal Midfoot Approaches: Surgical Anatomy, Indications, & Techniques

Key Takeaway
Dorsal midfoot surgical approaches provide critical access for diverse pathologies from the talonavicular to tarsometatarsal joints. These interventions are vital for treating Lisfranc injuries, midfoot fractures, painful degenerative arthritis, and excising exostoses. Mastery requires precise anatomical knowledge of the navicular, cuboid, cuneiforms, ligaments, and neurovascular structures, enabling effective fixation and fusion procedures.
Introduction and Epidemiology
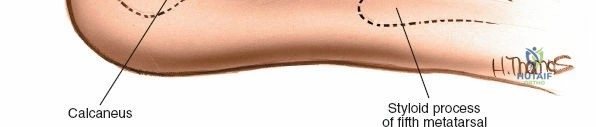
The middle part of the foot encompasses the region from the calcaneocuboid and talonavicular joints proximally to the tarsometatarsal or Lisfranc joints distally. This complex anatomical segment includes the navicular, cuboid, and three cuneiform bones, articulating with each other and with the bases of the metatarsals. While these bones and their associated joints are superficial and accessible via dorsal, medial, lateral, and plantar approaches, the dorsal approaches are paramount for a wide array of surgical interventions.
Operations in this area, though not as frequently performed as forefoot or ankle procedures, are critical for addressing specific pathologies related to trauma, degenerative conditions, and congenital or acquired deformities. The insertions of powerful muscles controlling foot inversion and eversion (tibialis anterior, peroneus longus, peroneus brevis, tibialis posterior) dictate the dynamic balance of the midfoot and are often involved in tendon transfers or repairs via dorsal or dorsomedial approaches. Beyond muscle imbalance and mobile flatfoot, dorsal approaches are primarily indicated for open reduction and internal fixation of midfoot fractures and fracture-dislocations, arthrodesis for painful degenerative arthritis or severe deformities, excision of symptomatic dorsal exostoses, and debridement of deep space infections.

Epidemiologically, Lisfranc injuries represent a significant, albeit relatively uncommon, traumatic pathology affecting approximately 1 in 55,000 people annually, with a high propensity for long-term disability if not accurately diagnosed and treated. Up to 20% of Lisfranc injuries are missed on initial emergency department presentation. Midfoot arthritis, often post-traumatic or associated with inflammatory conditions, is a prevalent cause of chronic foot pain, necessitating surgical intervention in advanced stages. Understanding the nuances of dorsal surgical exposures is fundamental for any orthopedic surgeon treating the foot and ankle, as precise dissection mitigates the risk to superficial neurovascular structures and preserves the tenuous soft tissue envelope.
Surgical Anatomy and Biomechanics
The middle part of the foot is a remarkably stable and complex region, crucial for load transfer, arch support, and adaptive pronation and supination during gait. Mastery of dorsal approaches demands an intimate understanding of its bony architecture, ligamentous stabilizers, musculotendinous units, and neurovascular pathways.
Osteology of the Midfoot
The midfoot comprises seven bones: the navicular, cuboid, and the three cuneiforms (medial, intermediate, lateral), which articulate with each other and the bases of the first through fifth metatarsals.
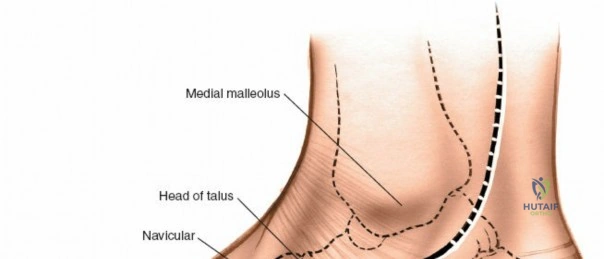
* Navicular: A boat-shaped bone articulating with the talar head proximally, the three cuneiforms distally, and the cuboid laterally. Its medial prominence, the tuberosity, is a key insertion site for the tibialis posterior tendon. The central third of the navicular is a known vascular watershed area, predisposing it to stress fractures and avascular necrosis (Kohler disease in pediatrics, Mueller-Weiss syndrome in adults).
* Cuneiforms: Three wedge-shaped bones that form the transverse arch of the foot.
* Medial Cuneiform: The largest, articulating with the navicular proximally, intermediate cuneiform laterally, and the first and second metatarsals distally. It receives insertions from the tibialis anterior and peroneus longus.
* Intermediate Cuneiform: The smallest, articulating with the navicular, medial and lateral cuneiforms, and the second metatarsal.
* Lateral Cuneiform: Articulates with the navicular, intermediate cuneiform, cuboid, and the second, third, and fourth metatarsals.
* Cuboid: Roughly cuboidal, articulating with the calcaneus proximally, lateral cuneiform and navicular medially, and the fourth and fifth metatarsals distally. The peroneus longus tendon grooves its plantar surface.
* Metatarsal Bases: The proximal ends of the metatarsals articulate with the cuneiforms and cuboid, forming the tarsometatarsal joints. The base of the second metatarsal is recessed between the medial and lateral cuneiforms, creating a "keystone" configuration critical for midfoot stability. The base of the fifth metatarsal serves as the insertion for the peroneus brevis tendon and is a frequent site of avulsion fractures.
Ligamentous Stabilizers
The stability of the midfoot relies heavily on its ligamentous complexes, as the dorsal bony architecture offers less inherent stability than the plantar aspect. The plantar ligaments are significantly thicker and stronger than their dorsal counterparts, reflecting their role as primary tension bands during weight-bearing.
The Lisfranc ligament complex is paramount. It is a stout interosseous ligament originating from the lateral aspect of the medial cuneiform and inserting onto the medial aspect of the second metatarsal base. Notably, there is no direct intermetatarsal ligament connecting the bases of the first and second metatarsals, making this interval uniquely vulnerable to diastasis. The plantar tarsometatarsal ligaments reinforce the longitudinal and transverse arches, while the dorsal ligaments are relatively thin capsular thickenings.
Neurovascular Anatomy
When executing dorsal midfoot approaches, precise identification and protection of superficial neurovascular structures are mandatory.
- Superficial Peroneal Nerve: Pierces the deep fascia in the distal third of the leg and divides into the medial dorsal cutaneous nerve (supplying the medial aspect of the hallux, and the adjacent sides of the second and third toes) and the intermediate dorsal cutaneous nerve (supplying the adjacent sides of the third, fourth, and fifth toes). These branches course directly through the subcutaneous tissues over the dorsal midfoot.
- Deep Peroneal Nerve: Courses deep to the extensor retinaculum alongside the dorsalis pedis artery. In the midfoot, it runs between the extensor hallucis longus (EHL) and extensor digitorum longus (EDL) tendons, specifically supplying sensation to the first web space and motor innervation to the extensor digitorum brevis (EDB) and extensor hallucis brevis (EHB).
- Dorsalis Pedis Artery: The continuation of the anterior tibial artery distal to the extensor retinaculum. It courses dorsally over the navicular and middle cuneiform, typically lying lateral to the EHL tendon and medial to the deep peroneal nerve. It dives plantarly at the proximal aspect of the first intermetatarsal space to join the deep plantar arch.
Indications and Contraindications
Dorsal approaches to the midfoot are versatile and provide the necessary exposure for a variety of complex reconstructive and traumatological procedures. The decision to proceed operatively depends on the degree of instability, the presence of articular incongruity, and the patient's functional demands.
Relative and absolute contraindications primarily revolve around the integrity of the soft tissue envelope. The dorsal midfoot has minimal subcutaneous fat; therefore, incisions through compromised skin (e.g., severe fracture blisters, active cellulitis, or profound peripheral vascular disease) carry an unacceptably high risk of wound dehiscence and deep infection. Active Charcot neuroarthropathy in the acute inflammatory phase (Eichenholtz Stage 1) is generally a contraindication for internal fixation, favoring total contact casting until consolidation occurs.
| Pathology Category | Operative Indications | Non Operative Indications |
|---|---|---|
| Trauma Lisfranc | Any displacement > 2mm, purely ligamentous instability, intra-articular comminution, compartment syndrome. | Nondisplaced injuries with stable weight-bearing radiographs, patients with severe medical comorbidities precluding surgery. |
| Midfoot Osteoarthritis | Intractable pain failing conservative management, progressive deformity (e.g., planovalgus collapse), osteophyte impingement. | Mild to moderate symptoms manageable with rigid orthotics, NSAIDs, or intra-articular corticosteroid injections. |
| Navicular Fractures | Displaced body fractures, tuberosity avulsions with significant displacement or nonunion, stress fractures failing prolonged immobilization. | Nondisplaced fractures, asymptomatic accessory navicular, stress fractures responding to non-weight-bearing cast immobilization. |
| Infection and Tumors | Abscess formation, osteomyelitis requiring debridement, symptomatic benign tumors (e.g., osteoid osteoma), malignant lesions. | Superficial cellulitis responding to oral or intravenous antibiotics. |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning ensures appropriate hardware selection, minimizes tourniquet time, and optimizes the surgical incision strategy to preserve skin bridges.
Imaging Modalities
Standard weight-bearing radiographs (anteroposterior, lateral, and 30-degree internal oblique views) are mandatory. On the AP view, the medial border of the second metatarsal should align perfectly with the medial border of the intermediate cuneiform. On the oblique view, the medial border of the fourth metatarsal should align with the medial border of the cuboid. A "fleck sign" (avulsion of the Lisfranc ligament from the second metatarsal base) is pathognomonic for a Lisfranc injury.
Computed Tomography (CT) is highly recommended for midfoot trauma to assess occult articular comminution, particularly at the plantar aspect of the tarsometatarsal joints, which dictates the feasibility of screw fixation versus dorsal spanning plates. Magnetic Resonance Imaging (MRI) is reserved for cases with high clinical suspicion of a purely ligamentous Lisfranc injury but normal weight-bearing radiographs.
Positioning and Tourniquet Application
The patient is positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, bringing the foot into a neutral, strictly vertical position. This facilitates true AP and lateral fluoroscopic imaging without requiring extreme rotation of the C-arm.
A thigh or calf tourniquet is applied based on surgeon preference and the anticipated duration of the procedure. A calf tourniquet is often preferred for isolated midfoot procedures to minimize thigh muscle ischemia and postoperative thigh pain, provided the proximal extent of the incision does not encroach on the tourniquet site. The limb is exsanguinated with an Esmarch bandage prior to tourniquet inflation. Prophylactic intravenous antibiotics are administered 30 minutes prior to inflation.
Detailed Surgical Approach and Technique
The dorsal approach to the midfoot is typically executed via one, two, or occasionally three longitudinal incisions, depending on the extent of the pathology. The dual-incision technique is the gold standard for comprehensive Lisfranc fracture-dislocations and multi-joint midfoot arthrodesis.
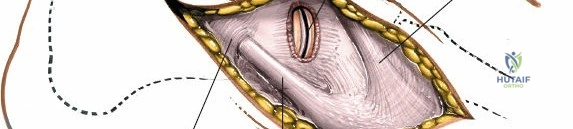
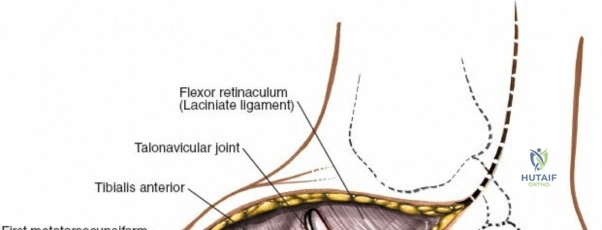
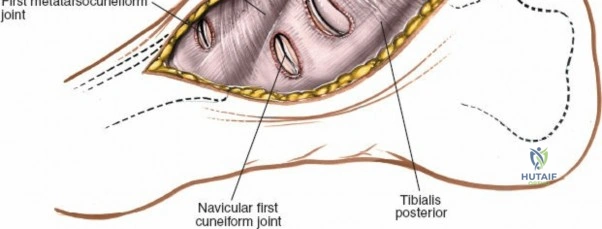
Medial Dorsal Incision
The medial dorsal incision accesses the medial column (first TMT joint, naviculocuneiform joint) and the intermediate column (second TMT joint).
1. Incision Placement: A longitudinal incision is centered over the first intermetatarsal space, beginning at the level of the navicular and extending distally to the proximal third of the first and second metatarsals.
2. Superficial Dissection: The skin and subcutaneous tissues are incised. Careful blunt dissection is required to identify and retract branches of the medial dorsal cutaneous nerve. The extensor hallucis longus (EHL) tendon is identified.
3. Deep Dissection: The deep fascia is incised. The EHL tendon is mobilized and retracted medially. The extensor hallucis brevis (EHB) muscle belly and the extensor digitorum longus (EDL) tendons are retracted laterally.
4. Neurovascular Protection: The neurovascular bundle, containing the dorsalis pedis artery and the deep peroneal nerve, typically lies between the EHL and EHB/EDL. This bundle must be meticulously mobilized and protected, usually by retracting it laterally with the EHB, although medial retraction is occasionally necessary depending on the specific anatomy and required exposure.
5. Capsulotomy: Longitudinal capsulotomies are performed over the first and second TMT joints, exposing the articular surfaces. Subperiosteal dissection is maintained to preserve the dorsal vascular supply to the metatarsal bases.
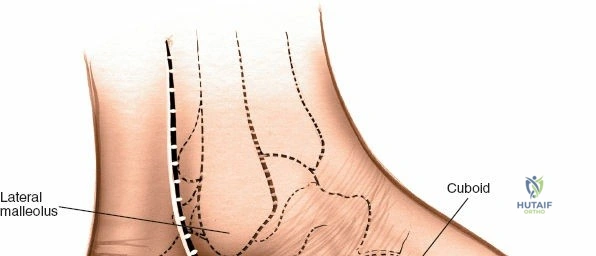
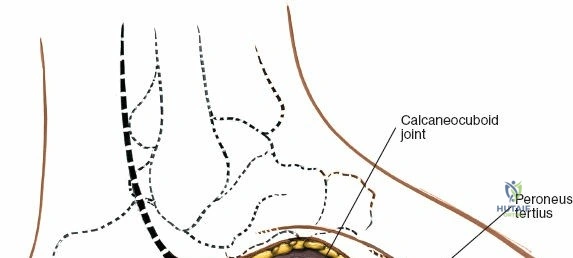
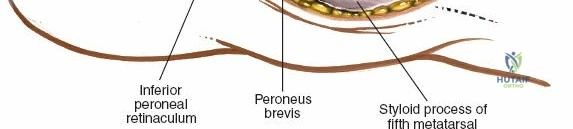
Lateral Dorsal Incision
The lateral dorsal incision provides access to the lateral column (third, fourth, and fifth TMT joints) and the calcaneocuboid joint.
1. Incision Placement: A second longitudinal incision is placed centered over the third or fourth metatarsal base. Crucially, a minimum skin bridge of 5 to 7 centimeters must be maintained between the medial and lateral incisions to prevent catastrophic skin necrosis.
2. Superficial Dissection: The intermediate dorsal cutaneous nerve branches are identified in the subcutaneous tissue and retracted.
3. Deep Dissection: The fascia is incised, and the EDL and peroneus tertius tendons are retracted medially or laterally to expose the underlying joints. The extensor digitorum brevis (EDB) muscle belly often overlies the lateral TMT joints and must be elevated from proximal to distal or split longitudinally to gain access to the third and fourth TMT joints and the cuboid.
4. Capsulotomy: Capsulotomies are performed over the relevant joints, allowing for joint debridement or fracture reduction.

Internervous Planes and Deep Dissection
Strictly speaking, there is no true internervous plane on the dorsum of the midfoot, as the EHL, EDL, EHB, and EDB are all innervated by the deep peroneal nerve. The approaches utilize intermuscular intervals. The medial approach uses the interval between the EHL and EDL/EHB. The lateral approach uses intervals between the EDL tendons or between the EDL and peroneus tertius. Deep dissection must remain subperiosteal and extra-articular until the specific joint capsule is incised to minimize heterotopic ossification and preserve local vascularity.
Reduction and Fixation Strategies
For Lisfranc injuries, the reduction sequence is critical and must proceed from medial to lateral.
1. First TMT Joint: The first metatarsal is reduced onto the medial cuneiform and provisionally pinned with a K-wire.
2. Second TMT Joint: The second metatarsal base (the keystone) is reduced into the recess between the medial and lateral cuneiforms. A reduction clamp is often placed from the medial cuneiform to the lateral aspect of the second metatarsal base to recreate the Lisfranc ligament tension.
3. Lateral Column: Once the medial and central columns are anatomically reduced, the lateral column (third, fourth, and fifth TMT joints) often reduces indirectly. If not, it is reduced and pinned.
Fixation options vary based on the specific pathology:
* Transarticular Screws: Historically the gold standard. Solid 3.5mm or 4.0mm cortical screws are placed from the medial cuneiform into the base of the first and second metatarsals. This provides rigid fixation but inherently damages the articular cartilage.
* Dorsal Spanning Plates: Increasingly preferred for purely ligamentous injuries and comminuted fractures. These plates bridge the joints without violating the articular surface, theoretically reducing the risk of post-traumatic arthritis.
* Flexible Fixation: Suture button constructs are sometimes utilized for the Lisfranc interval to allow for physiologic micromotion, avoiding the need for routine hardware removal.
* Arthrodesis: For chronic injuries or severe primary comminution, primary arthrodesis of the first, second, and third TMT joints is performed using a combination of crossed screws and dorsal locking plates after meticulous denudation of the articular cartilage and subchondral drilling.
Complications and Management
Surgical intervention in the dorsal midfoot carries inherent risks due to the tenuous soft tissue envelope, the density of superficial neurovascular structures, and the critical load-bearing function of the transverse and longitudinal arches. Anticipation and prompt management of complications are vital for optimizing patient outcomes.
Post-traumatic osteoarthritis is the most common long-term complication following midfoot trauma, particularly if anatomic reduction is not achieved or maintained. Hardware prominence is also frequent due to the lack of dorsal subcutaneous fat, often necessitating secondary procedures for hardware removal.
| Complication | Incidence | Etiology and Risk Factors | Salvage Strategies and Management |
|---|---|---|---|
| Post Traumatic Osteoarthritis | 25% - 50% (higher in ORIF vs primary fusion) | Cartilage damage at time of injury, non-anatomic reduction, transarticular screw damage. | Conservative management (orthotics, NSAIDs). Surgical salvage via midfoot arthrodesis. |
| Wound Dehiscence and Infection | 2% - 10% | Inadequate skin bridge (< 5cm), severe initial soft tissue trauma, smoking, diabetes. | Local wound care, culture-directed antibiotics. Negative pressure wound therapy. Flap coverage for exposed hardware/bone. |
| Hardware Failure or Prominence | 15% - 30% | Early weight-bearing, fatigue failure of transarticular screws, prominent dorsal plates. | Hardware removal once clinical and radiographic union is achieved (typically 4-6 months post-op). Revision fixation if nonunion is present. |
| Nerve Injury (Neuroma) | 5% - 15% | Iatrogenic traction or transection of superficial peroneal or deep peroneal nerve branches. | Gabapentinoids, targeted nerve blocks. Surgical excision of neuroma and implantation of the proximal stump into muscle or bone. |
| Nonunion or Malunion | 5% - 10% | Inadequate fixation rigidity, poor bone biology, smoking, failure to recognize subtle instability. | Revision arthrodesis with structural bone grafting (autograft or allograft) to restore arch height and rigid internal fixation. |
| Complex Regional Pain Syndrome | 2% - 5% | Exaggerated inflammatory response to trauma and surgery, prolonged immobilization. | Early recognition. Multidisciplinary approach: aggressive physical therapy, sympathetic nerve blocks, neuropathic pain modulators. |
Post Operative Rehabilitation Protocols
Rehabilitation following dorsal midfoot surgery is protracted and requires strict patient compliance to prevent catastrophic failure of fixation or loss of reduction. The protocol is generally divided into distinct phases, heavily dependent on whether the procedure was an ORIF or a primary arthrodesis.
Phase 1: Maximum Protection (Weeks 0-2)
Immediately postoperatively, the patient is placed in a bulky, non-weight-bearing Robert Jones splint. Strict elevation above the level of the heart is mandatory to control edema and protect the dorsal incisions. At the 2-week mark, sutures are removed, and the patient is transitioned to a short leg cast or a rigid fracture boot.
Phase 2: Immobilization and Early Motion (Weeks 2-6)
The patient remains strictly non-weight-bearing. If a removable fracture boot is utilized, gentle active range of motion of the ankle and metatarsophalangeal joints may be initiated to prevent stiffness, provided the midfoot remains rigidly supported.
Phase 3: Progressive Weight Bearing (Weeks 6-12)
Clinical and radiographic evaluation is performed at 6 weeks. If there is evidence of maintained reduction or early consolidation of an arthrodesis, progressive weight-bearing is initiated in a rigid fracture boot. Patients typically begin at 25% body weight and advance by 25% weekly. Physical therapy focuses on intrinsic foot muscle strengthening, proprioception, and graduated Achilles tendon stretching.
Phase 4: Return to Function (Months 3-6+)
Patients are transitioned from the boot to a stiff-soled shoe with a custom molded orthotic featuring longitudinal arch support. High-impact activities and sports are generally restricted until 5 to 6 months postoperatively. If transarticular screws were used across mobile joints (e.g., the 4th and 5th TMT joints), they are typically removed at 3 to 4 months to restore physiological motion and prevent screw breakage.
Summary of Key Literature and Guidelines
The surgical management of midfoot pathology, particularly Lisfranc injuries, has evolved significantly based on landmark biomechanical and clinical outcome studies.
- Primary Arthrodesis vs. ORIF: A paradigm shift occurred following the seminal randomized controlled trials by Ly and Coetzee (2006) and Henning et al. (2009). These studies demonstrated that for purely ligamentous Lisfranc injuries, primary arthrodesis of the medial and central columns resulted in superior functional outcomes, lower rates of hardware failure, and decreased necessity for secondary surgeries compared to traditional ORIF. ORIF remains the standard of care for acute, bony fracture-dislocations where the articular cartilage is largely preserved.
- Dorsal Spanning Plates: Recent literature has heavily supported the use of dorsal spanning plates for midfoot trauma. Studies indicate that extra-articular plating provides biomechanical stability comparable to transarticular screws while avoiding iatrogenic chondral damage, thereby theoretically reducing the incidence of post-traumatic osteoarthritis.
- Flexible Fixation: The use of suture button constructs for the Lisfranc interval has gained traction. Biomechanical studies show that suture buttons provide adequate stability to allow ligamentous healing while preserving the natural micromotion of the midfoot complex. Clinical series report favorable functional outcomes and eliminate the morbidity associated with routine hardware removal.
Academic orthopedic surgeons must synthesize these evidence-based guidelines with patient-specific factors—such as age, functional demands, bone quality, and soft tissue integrity—when selecting the optimal surgical approach and fixation strategy for the dorsal midfoot.

