Dorsal Approach for Morton's Neuroma Excision: A Comprehensive Guide

Key Takeaway
The dorsal surgical approach for Morton's neuroma excision offers significant advantages, including incision placement in a non-weight-bearing area. This minimizes post-operative scar tenderness and facilitates earlier mobilization compared to traditional plantar approaches. Surgery is indicated after conservative management fails, for severe pain, and with clear radiographic diagnosis.
Introduction and Epidemiology
Morton's neuroma, or interdigital neuroma, is a common compressive neuropathy of the foot, characterized by perineural fibrosis and nerve degeneration, typically affecting the common digital nerve. While historically termed a "neuroma," it is pathologically not a true tumor but rather a reactive hyperplasia of the nerve sheath and surrounding tissues, involving demyelination, endoneurial edema, and vascular proliferation. The condition primarily manifests as forefoot pain, often described as burning, tingling, or electric shock-like sensations, exacerbated by weight-bearing activities and constrictive footwear. Pain frequently radiates into the toes. The most common location is the third intermetatarsal space, affecting the third common digital nerve which receives contributions from both the medial and lateral plantar nerves. The second intermetatarsal space is the next most common site, while the first and fourth spaces are rarely involved.
Epidemiologically, Morton's neuroma is significantly more prevalent in women than men, with a reported ratio of approximately 4:1. It most frequently affects individuals in their middle decades, typically between 30 and 60 years of age. Factors implicated in its etiology include repetitive microtrauma, biomechanical abnormalities leading to increased pressure on the interdigital nerve, and entrapment beneath the deep transverse metatarsal ligament. The dorsal surgical approach for Morton's neuroma excision offers distinct advantages, particularly concerning incision placement in a non-weight-bearing area, which minimizes post-operative scar tenderness and facilitates earlier mobilization compared to traditional plantar approaches.

Differential diagnosis is crucial and includes metatarsophalangeal joint synovitis, plantar plate tears, stress fractures of the metatarsals, Freiberg's infraction, ganglion cysts, and tarsal tunnel syndrome. Clinical diagnosis is supported by findings such as localized tenderness in the affected web space and a positive Mulder's click, though this sign is not pathognomonic. Diagnostic imaging, primarily ultrasound and magnetic resonance imaging, plays a vital role in confirming the diagnosis, assessing neuroma size, and excluding other forefoot pathologies. Ultrasound offers a dynamic evaluation, demonstrating the neuroma's compressibility and characteristic "tear-drop" shape. Magnetic resonance imaging provides superior anatomical detail and can differentiate the neuroma from soft tissue masses or inflammatory conditions.
Pathophysiology and Histology
Histological evaluation of excised interdigital neuromas consistently demonstrates marked perineural fibrosis, an increase in endoneurial collagen, and the presence of Renaut bodies. The epineurium is frequently thickened, and there is an associated proliferation of local vascular structures characterized by thickened vessel walls and hyalinization. These findings confirm that the pathology is primarily a degenerative and fibrotic process secondary to mechanical entrapment rather than a neoplastic proliferation of neural tissue. The chronic mechanical irritation leads to localized ischemia of the nerve, which further exacerbates the fibrotic cascade and subsequent demyelination, ultimately resulting in the characteristic neuropathic pain profile.
Surgical Anatomy and Biomechanics
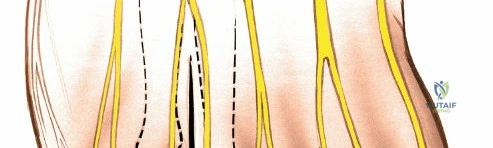
A thorough understanding of the surgical anatomy of the forefoot is paramount for a successful dorsal approach. The common digital nerves arise from the medial and lateral plantar nerves. The third common digital nerve, being the most frequently affected, is unique in receiving contributions from both the medial and lateral plantar nerves. This bifurcation often positions the nerve more anteriorly within the third web space, making it potentially more susceptible to compression.
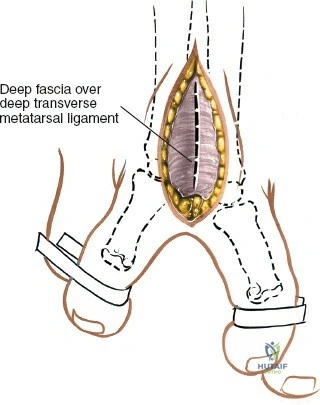
The common digital nerves run longitudinally within the intermetatarsal spaces, superficial to the interosseous muscles and deep to the deep transverse metatarsal ligament. The deep transverse metatarsal ligament is a strong fibrous band connecting the heads of the metatarsals, effectively creating a tunnel through which the common digital nerves pass as they bifurcate into their respective proper digital branches. Compression of the nerve beneath the deep transverse metatarsal ligament, exacerbated by metatarsal head splaying during weight-bearing and constrictive footwear, is a primary biomechanical factor in neuroma development. The nerve's vascular supply, derived from the plantar metatarsal arteries, is also vulnerable to this compression, potentially leading to ischemic changes and perineural fibrosis.
Adjacent structures including the lumbrical muscles, interosseous tendons, and the plantar plate must be carefully protected during surgical exploration. The lumbrical muscle typically runs on the medial aspect of the corresponding toe and passes plantar to the deep transverse metatarsal ligament alongside the neurovascular bundle.
Intermetatarsal Space Anatomy
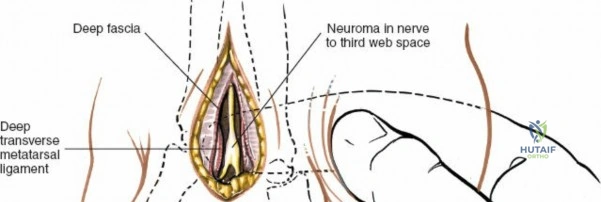
The intermetatarsal space is a distinct anatomical compartment bounded dorsally by the dorsal interosseous fascia and plantarly by the deep transverse metatarsal ligament. Within this space lies the intermetatarsal bursa, which is situated dorsal to the neurovascular bundle. In cases of Morton's neuroma, this bursa is frequently inflamed and hypertrophied, creating a bursitis that can obscure the underlying nerve during a dorsal approach. The surgeon must systematically excise or retract this bursal tissue to gain adequate visualization of the deep transverse metatarsal ligament and the underlying common digital nerve.
Biomechanical Considerations
Biomechanically, the forefoot undergoes significant stress during the terminal stance phase of the gait cycle. As the heel rises, the metatarsophalangeal joints dorsiflex, engaging the windlass mechanism. This action tightens the plantar fascia and the deep transverse metatarsal ligament, effectively narrowing the intermetatarsal space. In patients utilizing footwear with a narrow toe box or elevated heels, the metatarsal heads are subjected to increased extrinsic compression while simultaneously being forced into hyperextension. This combination creates a mechanical tethering of the common digital nerve against the unyielding distal edge of the deep transverse metatarsal ligament, precipitating the repetitive microtrauma fundamental to the pathogenesis of perineural fibrosis.
Indications and Contraindications
The decision to proceed with surgical excision of an interdigital neuroma via a dorsal approach requires a careful assessment of the patient's clinical history, physical examination findings, and response to conservative modalities. Surgery is generally reserved for patients who have experienced persistent, functionally limiting pain despite a comprehensive trial of non-operative management.
Operative Versus Non Operative Management
Conservative management should always be the initial line of treatment. This includes footwear modifications such as utilizing wide toe boxes, rigid soles, and lower heels. Metatarsal pads placed proximal to the metatarsal heads can help splay the intermetatarsal space and reduce pressure on the nerve. Pharmacological interventions, including nonsteroidal anti-inflammatory drugs and targeted corticosteroid injections, are frequently utilized. Corticosteroid injections can provide significant diagnostic and therapeutic utility, though repeated injections carry the risk of plantar fat pad atrophy and plantar plate attenuation. Alcohol sclerosing injections have also been described but remain controversial due to variable success rates and the risk of severe inflammatory reactions.
When non-operative measures fail to provide durable relief after a period of three to six months, surgical intervention is indicated. The dorsal approach is the preferred primary surgical strategy due to its favorable complication profile regarding scar formation and weight-bearing tolerance.
| Management Strategy | Indications for Use | Key Considerations and Outcomes |
|---|---|---|
| Conservative Footwear Modification | Initial presentation, mild to moderate symptoms, patient preference for non-operative care. | First-line therapy. Requires strict patient compliance. High initial success but variable long-term durability. |
| Orthotics and Metatarsal Pads | Biomechanical abnormalities (e.g., pes planus, hypermobility), localized pressure points. | Shifts weight-bearing forces proximal to the metatarsal heads. Can be combined with footwear modifications. |
| Corticosteroid Injection | Moderate to severe acute pain, diagnostic confirmation, failure of physical modifications. | Limits inflammation and edema. Risk of plantar fat pad atrophy if placed too superficially. Limit to 2-3 injections. |
| Primary Dorsal Neurectomy | Failure of 3-6 months of conservative management, persistent severe pain, positive MRI/Ultrasound. | Gold standard operative treatment. Avoids plantar scarring. Requires release of deep transverse metatarsal ligament. |
| Plantar Approach Neurectomy | Revision surgery for stump neuroma, extremely proximal primary neuromas. | Allows excellent proximal visualization. High risk of painful plantar keratosis and delayed weight-bearing. |
Contraindications to the dorsal approach include active localized soft tissue infection, severe vascular compromise (e.g., advanced peripheral arterial disease), and complex regional pain syndrome. In patients with concurrent severe metatarsophalangeal joint instability or plantar plate tears, isolated neuroma excision may fail to resolve the patient's symptoms, and a more comprehensive forefoot reconstruction should be considered.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential to ensure accurate localization of the pathology and to minimize the risk of wrong-site surgery. The clinical examination must be meticulously documented, noting the specific intermetatarsal space affected. The web space compression test (Mulder's sign) and the Sullivan sign (splaying of the adjacent toes upon weight-bearing) should be evaluated.
Clinical Evaluation and Imaging
While the diagnosis of Morton's neuroma is primarily clinical, advanced imaging is highly recommended prior to surgical intervention to confirm the diagnosis, assess the exact dimensions of the neuroma, and rule out concomitant pathology such as metatarsophalangeal joint synovitis or intermetatarsal bursitis. High-resolution ultrasound is highly sensitive and allows for dynamic assessment, often demonstrating a hypoechoic mass that reproduces the patient's symptoms upon transducer pressure (sonographic Mulder's sign). Magnetic resonance imaging without contrast is excellent for evaluating the entire forefoot anatomy and is particularly useful in cases of atypical presentation or suspected multiple neuromas.

Operating Room Setup
The patient is positioned supine on the operating table. A small bump may be placed under the ipsilateral hip to correct natural external rotation of the lower extremity, ensuring the dorsal aspect of the foot faces directly upwards. A well-padded thigh tourniquet or a calf tourniquet is applied to provide a bloodless surgical field, which is critical for identifying the delicate neural structures and maintaining hemostasis. The surgical site is marked in the preoperative holding area with the patient awake and participating in the site verification process. The specific web space is marked dorsally. Intravenous prophylactic antibiotics are administered according to institutional protocols, typically a first-generation cephalosporin, within one hour prior to tourniquet inflation.
Detailed Surgical Approach and Technique
The dorsal approach for Morton's neuroma excision requires meticulous soft tissue handling and precise anatomical dissection to ensure complete resection of the pathological nerve segment while preserving adjacent stabilizing structures.
Incision and Superficial Dissection
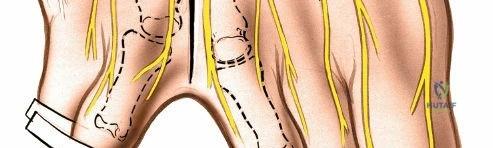
Following exsanguination and tourniquet inflation, a 2 to 3 centimeter longitudinal incision is made on the dorsal aspect of the affected web space. The incision should begin at the level of the web space commissure and extend proximally, bisecting the distance between the adjacent metatarsal heads. Care must be taken to avoid placing the incision too far distally into the web space skin fold, which can lead to maceration or painful contracture.
Blunt dissection is utilized to deepen the incision through the subcutaneous tissues. Small superficial dorsal veins are frequently encountered and should be meticulously electrocoagulated or ligated to prevent postoperative hematoma formation. A self-retaining Weitlaner retractor or small Senn retractors are placed to maintain exposure. The dorsal interosseous fascia is identified and incised longitudinally. Deep to this fascia, the intermetatarsal bursa is typically encountered. If the bursa is significantly hypertrophied, it may be excised at this stage to improve visualization of the deeper structures.
Deep Transverse Metatarsal Ligament Release
The critical step in the dorsal approach is the identification and complete transection of the deep transverse metatarsal ligament. The surgeon can place a blunt instrument, such as a Freer elevator or a small curved hemostat, deep to the ligament to protect the underlying neurovascular bundle. The deep transverse metatarsal ligament is then sharply divided under direct visualization. Complete release is verified by palpating the space and observing the splaying of the adjacent metatarsal heads.
Once the ligament is released, the surgeon applies upward pressure on the plantar aspect of the foot, directly beneath the affected web space. This maneuver pushes the common digital nerve and the associated neuroma dorsally into the surgical field. The neuroma typically appears as a fusiform, bulbous enlargement of the nerve, often exhibiting a yellowish or grayish discoloration compared to the normal proximal nerve tissue.
Nerve Resection and Closure
The proper digital branches of the nerve, which extend distally into the adjacent toes, are identified first. These branches are sharply transected as far distally as possible. The nerve is then mobilized proximally. It is imperative to dissect the common digital nerve proximally well beyond the deep transverse metatarsal ligament and the weight-bearing surface of the metatarsal heads.
Traction is applied to the nerve, and it is sharply transected at least 1 to 2 centimeters proximal to the deep transverse metatarsal ligament. A sharp scalpel or specialized nerve scissors should be used to ensure a clean cut, minimizing crush injury to the proximal stump. Following transection, the proximal nerve stump is observed to retract deeply into the intrinsic muscle belly of the interosseous muscles. This deep retraction is a critical technical endpoint, as it places the nerve stump in a protected, non-weight-bearing environment, significantly reducing the risk of a symptomatic recurrent stump neuroma.
The surgical field is thoroughly irrigated with sterile saline. The tourniquet is deflated prior to closure to achieve meticulous hemostasis, which is vital for preventing postoperative hematoma. The deep tissues are typically left open to avoid compartmental hypertension. The skin is closed using non-absorbable monofilament sutures (e.g., 4-0 nylon) in a simple interrupted or horizontal mattress fashion. A bulky, compressive soft dressing is applied to control edema and limit dead space.
Complications and Management
While primary excision of an interdigital neuroma via a dorsal approach yields high patient satisfaction rates, complications can occur and must be managed promptly to optimize clinical outcomes.
Prevention of Stump Neuroma
The most feared and challenging complication is the development of a true amputation stump neuroma. Unlike the primary Morton's neuroma, which is a perineural fibrosis, a stump neuroma is a disorganized proliferation of axonal sprouts attempting to regenerate following transection. If the primary nerve resection was inadequate and the stump rests in a weight-bearing zone beneath the metatarsal heads, severe, intractable pain will ensue.
Prevention is entirely dependent on meticulous surgical technique: ensuring the proximal cut is made well proximal to the metatarsal heads and confirming that the stump retracts into the intrinsic musculature. If a symptomatic stump neuroma develops, conservative management is rarely successful. Revision surgery is typically required, often necessitating a plantar approach to identify the retracted stump, followed by further proximal resection and potentially burying the nerve end into bone or deep muscle.
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage Strategy and Management |
|---|---|---|---|
| Stump Neuroma | 5% - 10% | Inadequate proximal resection; nerve stump resting in weight-bearing zone. | Revision neurectomy (often via plantar approach); proximal transposition of nerve stump into muscle or bone. |
| Hematoma | 2% - 5% | Inadequate hemostasis; failure to deflate tourniquet prior to closure; excessive dead space. | Evacuation if large and threatening skin viability; compressive dressings; meticulous intraoperative electrocautery. |
| Wound Dehiscence / Infection | 1% - 3% | Premature suture removal; excessive early weight-bearing; poor vascular supply. | Local wound care; oral or intravenous antibiotics based on culture; delayed secondary closure if necessary. |
| Complex Regional Pain Syndrome | < 1% | Unclear etiology; exaggerated inflammatory/sympathetic response to surgical trauma. | Early recognition; aggressive physical therapy; neuropathic pain medications (gabapentin, pregabalin); sympathetic nerve blocks. |
| Digital Numbness | 100% (Expected) | Inherent to neurectomy. | Preoperative patient counseling is critical. Not a true "complication" but an expected outcome of nerve resection. |
| Metatarsalgia | 5% - 8% | Altered forefoot biomechanics following deep transverse metatarsal ligament release. | Custom orthotics with metatarsal support; physical therapy focusing on intrinsic foot muscle strengthening. |
Hematoma formation is another potential complication, particularly given the vascularity of the intermetatarsal space. Deflating the tourniquet before wound closure allows for the identification and coagulation of bleeding vessels, significantly mitigating this risk. Postoperative infection is rare but must be treated aggressively with appropriate antibiotics and, if necessary, surgical debridement to prevent osteomyelitis of the adjacent metatarsals.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following a dorsal approach for Morton's neuroma excision is designed to protect the surgical incision, manage edema, and facilitate a safe return to weight-bearing activities.
Phased Recovery Guidelines
Phase 1: Immediate Postoperative Period (Weeks 0-2)
Immediately following surgery, the patient is placed in a bulky compressive dressing and provided with a rigid-soled postoperative shoe. Weight-bearing is typically restricted to heel-touch or flat-foot weight-bearing as tolerated. The patient is instructed to strictly elevate the operative extremity above the level of the heart for the first 48 to 72 hours to minimize edema and prevent hematoma formation. Ice application to the posterior ankle or popliteal fossa can be utilized for indirect cooling. The dressing is kept clean, dry, and intact until the first postoperative visit.
Phase 2: Suture Removal and Transition (Weeks 2-4)
The patient is evaluated in the clinic at approximately 10 to 14 days postoperatively for wound inspection and suture removal. If the incision is well-healed, the bulky dressing is discontinued. The patient may transition to a wide-toe box, supportive athletic shoe. Weight-bearing is advanced to full as tolerated. Physical therapy may be initiated at this stage, focusing on active and passive range of motion of the metatarsophalangeal joints to prevent stiffness and intrinsic muscle strengthening. Desensitization techniques for the surgical scar can also be introduced.
Phase 3: Return to Activity (Weeks 4-8)
During this phase, patients typically experience a significant reduction in surgical site pain. They are encouraged to gradually increase their walking distance and resume low-impact cardiovascular activities such as stationary cycling or swimming. High-impact activities, such as running or jumping, should be avoided until at least 6 to 8 weeks postoperatively to allow for complete soft tissue healing and stabilization of the intermetatarsal space. Patients must be counseled that mild, intermittent swelling may persist for several months following surgery and is generally managed effectively with compression stockings and activity modification.
Summary of Key Literature and Guidelines
The surgical management of Morton's neuroma has been extensively evaluated in the orthopedic literature, with a primary focus on comparing surgical approaches and assessing long-term patient outcomes. The consensus among foot and ankle specialists strongly supports the dorsal approach for primary neurectomy due to its favorable risk-to-benefit ratio.
Evidence Based Outcomes
Historically, there has been debate regarding the necessity of neurectomy versus isolated release of the deep transverse metatarsal ligament (neurolysis). Proponents of neurolysis argue that preserving the nerve maintains digital sensation and avoids the risk of a stump neuroma. However, comprehensive long-term studies have demonstrated that neurectomy provides a more reliable and durable resolution of symptoms in patients with established perineural fibrosis. A landmark study by Coughlin et al. reported excellent or good outcomes in over 85% of patients undergoing primary dorsal neurectomy, with a very low incidence of symptomatic stump neuromas when meticulous proximal resection techniques were employed.
The literature also heavily favors the dorsal approach over the plantar approach for primary excisions. While the plantar approach offers direct visualization of the nerve and facilitates a highly proximal resection, it is associated with a significantly higher rate of postoperative complications, most notably painful plantar keratosis and delayed wound healing due to the load-bearing nature of the plantar skin. Giannini and colleagues demonstrated that patients undergoing the dorsal approach returned to normal footwear and work activities significantly faster than those treated via a plantar incision.
Current clinical guidelines recommend that the plantar approach be reserved strictly for revision surgeries where the normal dorsal anatomy has been distorted by previous intervention, or for the excision of a known, proximally retracted stump neuroma. In primary cases, the dorsal approach, combining deep transverse metatarsal ligament release with aggressive proximal neurectomy, remains the gold standard, offering reproducible, high-quality outcomes for patients suffering from this debilitating compressive neuropathy.
