Comprehensive Introduction and Patho-Epidemiology
Chronic tenosynovitis (whether traumatic, degenerative, or secondary to inflammatory arthropathies), loss of tendon continuity, and the disruption of normal anatomical relationships at the tendon's insertion (such as the accessory navicular or prehallux syndrome) frequently render the posterior tibial tendon (PTT) insufficient. When the PTT fails to perform its critical biomechanical tasks—plantar flexion, hindfoot inversion, and dynamic stabilization of the medial longitudinal arch—the resulting clinical cascade is classically termed Posterior Tibial Tendon Insufficiency (PTTI). In contemporary orthopedic literature, this condition is increasingly encompassed by the broader and more biomechanically accurate term, Progressive Collapsing Foot Deformity (PCFD), reflecting the multi-ligamentous and multi-planar nature of the failure.
Other than the rupture of the Achilles tendon, no single muscle-tendon unit distal to the knee can precipitate as profound a functional deficit as the loss of the posterior tibial tendon. Any pathological state that diminishes the effective excursion of this tendon produces a hallmark clinical deformity: the asymmetrical adult-acquired flatfoot. The epidemiology of PTTI reveals a strong predilection for women in their fifth and sixth decades of life. The condition is heavily associated with systemic comorbidities that compromise microvascular perfusion and tendon integrity, most notably obesity, hypertension, diabetes mellitus, and seronegative spondyloarthropathies. Furthermore, local corticosteroid injections around the medial malleolus have been historically implicated in precipitating acute-on-chronic ruptures.

The pathophysiology of PTTI is fundamentally a process of mechanically induced tendinosis exacerbating an underlying vascular vulnerability. The tendon undergoes a degenerative cascade characterized by mucinoid degeneration, fibroblast hypercellularity, and the disruption of the normal parallel collagen bundle architecture. Matrix metalloproteinases (MMPs) are upregulated, shifting the homeostatic balance toward collagen degradation. As the tendon elongates and loses its mechanical advantage, the dynamic support of the medial longitudinal arch is lost. This transfers immense, unphysiological loads onto the static stabilizers of the foot—primarily the spring ligament complex, the plantar fascia, and the plantar ligaments of the midfoot—initiating a predictable sequence of secondary ligamentous attenuation and eventual joint subluxation.


Detailed Surgical Anatomy and Biomechanics
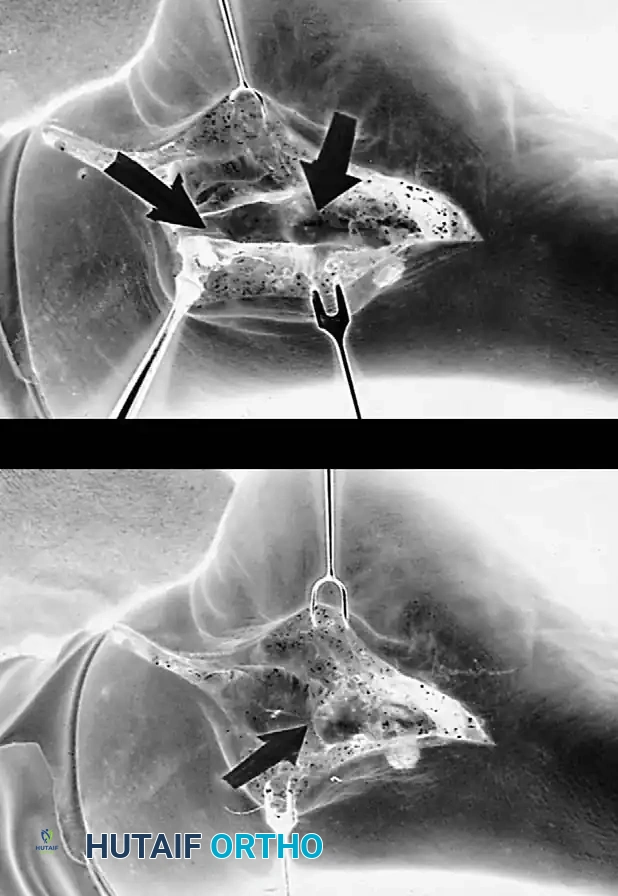
A profound understanding of the surgical anatomy of the posterior tibial tendon and its associated static stabilizers is non-negotiable for the reconstructive orthopedic surgeon. The tibialis posterior muscle originates from the posterior aspect of the interosseous membrane, the proximal posterior shaft of the tibia, and the medial aspect of the fibula. The muscle belly transitions into a robust tendon in the distal third of the leg, entering the retromalleolar groove of the medial malleolus. Here, it is constrained by the flexor retinaculum (laciniate ligament). The tendon possesses a critical hypovascular "watershed" zone located approximately 1 to 1.5 centimeters distal to the medial malleolus. This zone, supplied only by delicate vincula from the paratenon, is the most frequent epicenter for degenerative tearing and elongation.
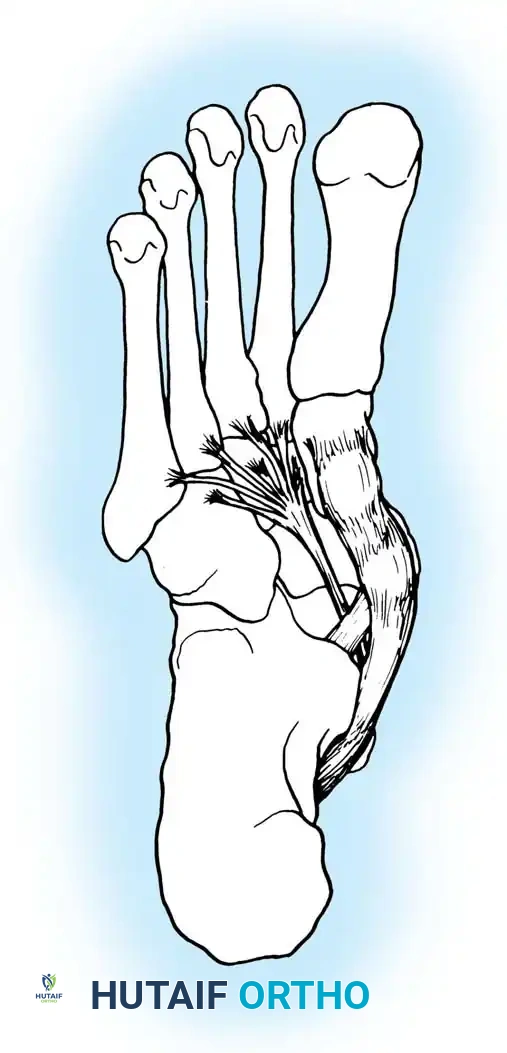
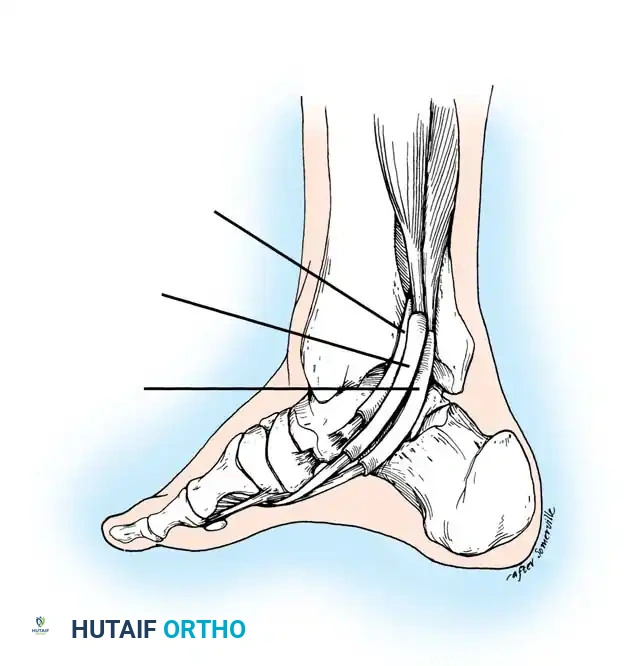
Distal to the medial malleolus, the PTT exhibits a broad, complex insertion footprint that is vital for its biomechanical function. The main tendon slip inserts directly onto the prominent tuberosity of the navicular bone and the plantar surface of the medial cuneiform. However, plantar extensions fan out to insert onto the middle and lateral cuneiforms, the cuboid, and the bases of the second, third, and fourth metatarsals. This diffuse insertion allows the PTT to act as a powerful supinator of the entire midfoot. During the normal gait cycle, as the foot transitions from midstance to terminal stance, the PTT fires to invert the subtalar joint. This inversion is the biomechanical linchpin of human ambulation: it aligns the axes of the talonavicular and calcaneocuboid joints in a non-parallel configuration, effectively "locking" the transverse tarsal joint. This converts the supple, shock-absorbing midfoot into a rigid lever arm essential for forceful propulsion by the gastrocnemius-soleus complex.

When the PTT becomes incompetent, the hindfoot is driven into unremitting valgus by the unopposed pull of the peroneus brevis. Consequently, the transverse tarsal joint remains unlocked throughout the stance phase. The gastrocnemius-soleus complex, rather than lifting the heel, acts to further plantarflex the talus and evert the calcaneus, driving the talar head plantarly and medially. This places catastrophic stress on the spring ligament complex (plantar calcaneonavicular ligament). The superomedial band of the spring ligament, which acts as a sling supporting the talar head, is the first static stabilizer to fail. As the talar head plantarflexes (creating a "sag" at the talonavicular joint), the midfoot abducts, and the forefoot is forced into compensatory supination to maintain plantigrade contact with the floor.


Exhaustive Indications and Contraindications
Surgical decision-making in PTTI is meticulously guided by the stage of the disease, the flexibility of the deformity, the competence of the medial collateral (deltoid) ligament of the ankle, and the presence of degenerative arthropathy. The classic Johnson and Strom classification, modified by Myerson, remains the foundational algorithm for surgical planning, though it must be integrated with an assessment of the patient's physiological age, bone quality, and vascular status.
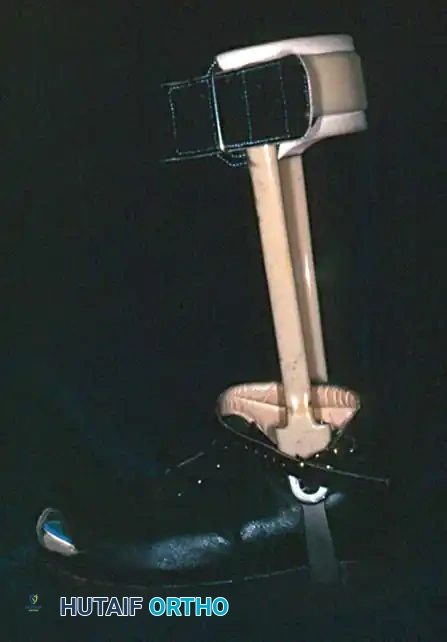
Conservative management—comprising rigid immobilization in a controlled ankle motion (CAM) boot, custom articulated ankle-foot orthoses (AFOs) such as the Arizona brace, non-steroidal anti-inflammatory drugs, and targeted physical therapy—is the mandatory first-line treatment. Surgical intervention is indicated only when a minimum of 3 to 6 months of comprehensive non-operative management has failed to arrest the progression of the deformity or alleviate debilitating pain.
The indications dictate a stepwise escalation in surgical magnitude. Stage I disease, characterized by tenosynovitis without morphological deformity, is an indication for tenosynovectomy and tendon debridement. Stage II disease, defined by a flexible flatfoot deformity, necessitates joint-sparing reconstruction to restore the medial longitudinal arch and re-establish the posterior tibial tendon's motor function. This typically involves a Flexor Digitorum Longus (FDL) transfer augmented by a Medial Displacement Calcaneal Osteotomy (MDCO) and, if severe forefoot abduction is present, a Lateral Column Lengthening (Evans osteotomy). Stage III disease, where the deformity has become rigid or subtalar/talonavicular arthritis has developed, mandates corrective arthrodesis, classically a triple or double arthrodesis. Stage IV disease, marked by deltoid ligament failure and tibiotalar tilt, requires complex tibiotalocalcaneal (TTC) or pantalar arthrodesis.
| Disease Stage | Pathoanatomy | Primary Surgical Indications | Absolute Contraindications |
|---|---|---|---|
| Stage I | Tenosynovitis, normal tendon length, no deformity, intact single-leg heel rise. | Failure of 3-6 months conservative care. Intractable medial pain. | Active local infection, severe peripheral vascular disease. |
| Stage IIa | Flexible hindfoot valgus, minimal midfoot abduction. | FDL transfer + MDCO. | Rigid deformity, subtalar/talonavicular osteoarthritis. |
| Stage IIb | Flexible hindfoot valgus, >40% talonavicular uncoverage (abduction). | FDL transfer + MDCO + Lateral Column Lengthening (Evans). | Rigid deformity, medial column arthritis. |
| Stage III | Rigid, fixed deformity. Degenerative joint changes in hindfoot. | Triple Arthrodesis or isolated subtalar/talonavicular fusion. | Active Charcot neuroarthropathy (relative), active infection. |
| Stage IV | Rigid flatfoot with deltoid failure and lateral talar tilt in ankle mortise. | Tibiotalocalcaneal (TTC) Arthrodesis or Deltoid reconstruction with hindfoot fusion. | Uncorrectable vascular insufficiency, profound immunocompromise. |



Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative clinical evaluation and radiographic templating are the cornerstones of successful PTTI reconstruction. The physical examination must systematically assess deformity flexibility, muscle strength, and the presence of contractures. The "too many toes" sign, observed from the posterior aspect, quantifies the degree of midfoot abduction. The single-leg heel rise test is paramount; failure to invert the calcaneus during this maneuver confirms PTT incompetence. The Silfverskiöld test is critical for identifying isolated gastrocnemius contracture versus global Achilles tendon tightness, as an unaddressed equinus contracture will place insurmountable stress on any medial column reconstruction, leading to inevitable failure.
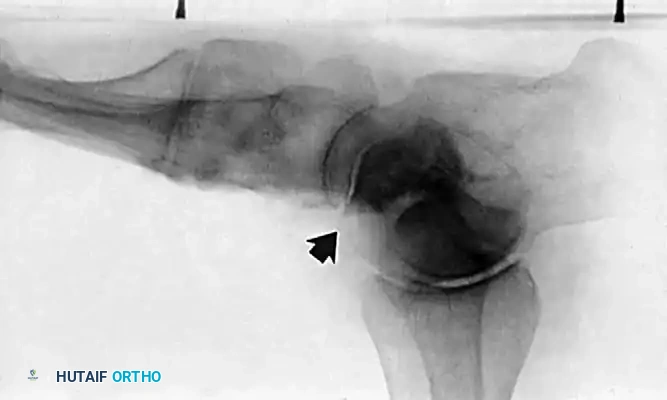
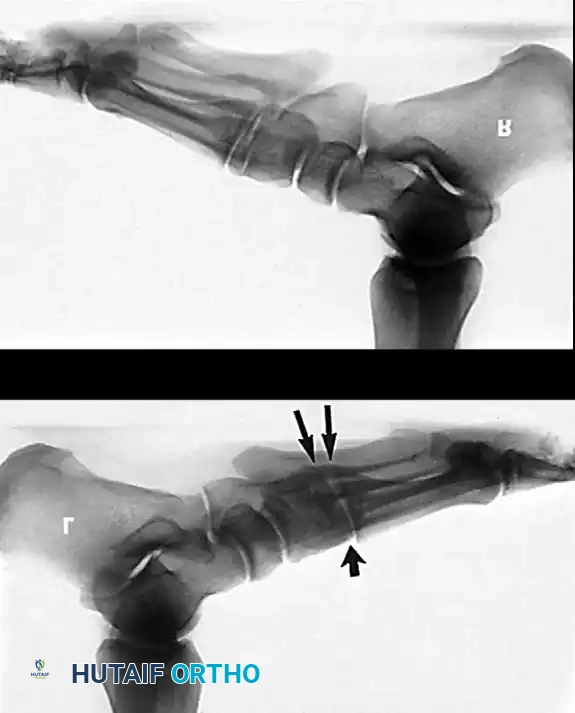
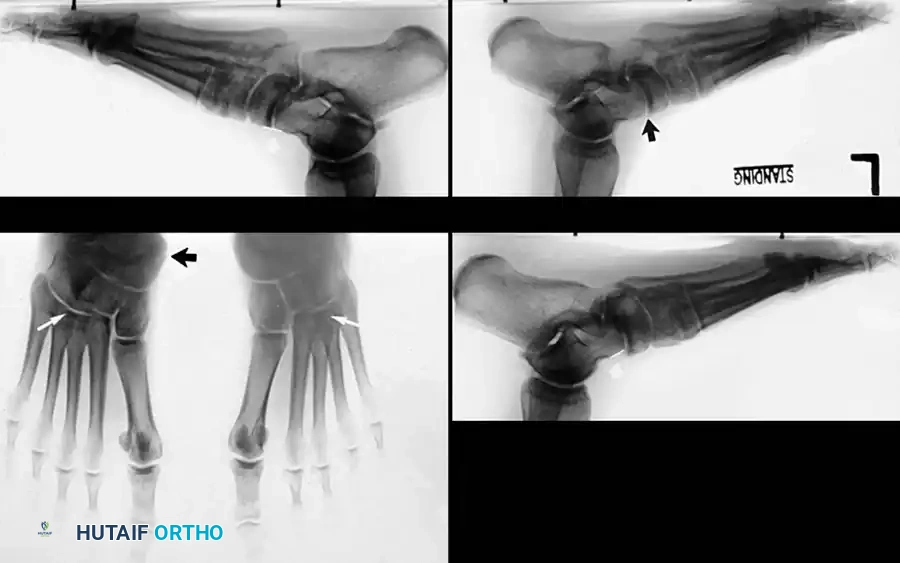
Radiographic evaluation requires weight-bearing anteroposterior (AP), lateral, and Harris axial heel views of the foot and ankle. On the weight-bearing AP view, the surgeon must quantify the talonavicular coverage angle; uncoverage greater than 30-40% indicates significant midfoot abduction and often necessitates a lateral column lengthening. On the weight-bearing lateral radiograph, Meary's line (the longitudinal axis of the talus intersecting the longitudinal axis of the first metatarsal) should be collinear. In PTTI, this line breaks, usually at the talonavicular or naviculocuneiform joint, indicating the apex of the collapse. The calcaneal pitch is decreased, and the lateral talocalcaneal angle is increased. The Harris heel view is utilized to assess the degree of hindfoot valgus and to template the medial displacement calcaneal osteotomy.


Advanced imaging is increasingly standard. Magnetic Resonance Imaging (MRI) is highly sensitive for evaluating the intrinsic substance of the PTT, identifying longitudinal split tears, and assessing the integrity of the spring ligament complex. However, Weight-Bearing Computed Tomography (WBCT) is rapidly becoming the gold standard for 3D pre-operative planning. WBCT allows for precise measurement of the Foot and Ankle Offset (FAO) and multiplanar assessment of peritalar subluxation, providing unparalleled data for osteotomy templating and hardware selection.
Patient positioning is dictated by the planned procedure. For Stage II reconstructions and Stage III triple arthrodeses, the patient is placed supine on the operating table with a bump under the ipsilateral hip to internally rotate the leg to a neutral position, allowing simultaneous access to both the medial and lateral aspects of the foot. A thigh tourniquet is applied, and the leg is prepped and draped free to above the knee. For Stage IV TTC arthrodesis utilizing a retrograde intramedullary nail, either a supine or lateral decubitus position may be utilized, with strict attention to fluoroscopic access for orthogonal imaging of the ankle and hindfoot.



Step-by-Step Surgical Approach and Fixation Technique
Surgical execution in PTTI demands meticulous soft-tissue handling and precise bony realignment. The surgical algorithm for Stage II flexible flatfoot is a multi-component reconstruction designed to restore the mechanical axis and provide a new dynamic stabilizer.
Stage II Reconstruction: Soft Tissue and Osteotomy Management
The procedure universally begins with addressing the equinus contracture. Based on the pre-operative Silfverskiöld test, either a gastrocnemius recession (Strayer or Baumann procedure) or a percutaneous Tendo-Achilles Lengthening (TAL) is performed. Releasing the deforming pull of the triceps surae is critical to reducing the pressure on the midfoot joints.
Attention is then directed to the medial displacement calcaneal osteotomy (MDCO). An oblique incision is made over the lateral hindfoot, carefully avoiding the sural nerve. The lateral wall of the calcaneus is exposed, and an oscillating saw is used to create an osteotomy perpendicular to the lateral wall, angled approximately 45 degrees to the plantar surface, exiting just posterior to the posterior facet of the subtalar joint. The posterior tuberosity is translated medially by 10 to 15 millimeters. This translation shifts the Achilles tendon insertion medially, converting it from a deforming evertor into a supinator, and profoundly reduces the mechanical strain on the medial column. Fixation is achieved with one or two large-fragment (6.5 mm or 7.3 mm) cannulated, partially threaded screws inserted from the posterior heel.


If severe midfoot abduction is present, a lateral column lengthening (Evans osteotomy) is performed through the same lateral incision, extended distally. An osteotomy is made 1.5 cm proximal to the calcaneocuboid joint. A lamina spreader is utilized to distract the osteotomy, swinging the midfoot out of abduction and covering the talar head. A tricortical iliac crest allograft or titanium wedge (typically 8-10 mm) is impacted into the defect and secured with a cervical plate or staple.
Medially, a longitudinal incision exposes the PTT and FDL. The diseased PTT is radically debrided or entirely excised if non-viable. The FDL is identified, traced distally to the master knot of Henry, and transected. A drill hole is created dorsal-to-plantar through the center of the navicular tuberosity. The FDL tendon is passed through this tunnel from plantar to dorsal. While the foot is held in maximal plantarflexion and inversion, the tendon is secured using a bio-tenodesis screw or sutured back onto itself. The spring ligament, if attenuated, is imbricated or reconstructed using local tissue flaps or suture tape augmentation. Finally, if residual forefoot varus (supination) exists after the hindfoot is corrected, a plantarflexion opening-wedge osteotomy of the medial cuneiform (Cotton osteotomy) is performed to render the foot plantigrade.


Stage III and IV Arthrodesis Techniques
For rigid Stage III deformities, a triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) is the gold standard. A dual-incision technique is utilized. The lateral incision exposes the subtalar and calcaneocuboid joints, while the medial incision exposes the talonavicular joint. Meticulous joint preparation is the most critical step; all articular cartilage and subchondral plate must be aggressively denuded down to bleeding, healthy cancellous bone using curettes, osteotomes, and high-speed burrs.
The deformity is manually reduced. The hindfoot must be fused in neutral to a maximum of 5 degrees of valgus. Fusing the hindfoot in any degree of varus is a disastrous technical error that will lead to a rigid, painful forefoot overload and lateral column pain. Fixation is typically achieved using large cannulated compression screws for the subtalar joint (calcaneus into the talus) and a combination of screws and low-profile locking plates for the talonavicular and calcaneocuboid joints.

In Stage IV disease with tibiotalar instability, a TTC arthrodesis is performed. The articular surfaces of the ankle and subtalar joints are prepared through a transfibular or anterior approach. The talus is centralized beneath the tibial plafond. A retrograde intramedullary nail is inserted through the plantar aspect of the calcaneus, driven through the talus, and locked into the tibial diaphysis. Robust compression across both fusion sites is achieved utilizing the nail's internal compression mechanism, often supplemented with independent compression screws to maximize construct rigidity.



Complications, Incidence Rates, and Salvage Management
Surgical management of PTTI is complex and fraught with potential complications. The surgeon must be acutely aware of these risks and possess the technical armamentarium to manage them effectively. Wound healing complications are particularly common on the medial aspect of the foot, especially in diabetic or obese patients, due to the tenuous vascularity of the skin flaps over the medial malleolus.
Nonunion is a significant concern, particularly in arthrodesis procedures. The talonavicular joint is notoriously difficult to fuse, with historical nonunion rates reported between 5% and 15%. This is attributed to the joint's complex spherical topography, which makes rigid planar compression challenging, and its precarious blood supply. If a symptomatic nonunion occurs, salvage requires revision arthrodesis with aggressive debridement, utilization of autologous bone graft (such as iliac crest or proximal tibia), and enhanced biological adjuvants like bone morphogenetic proteins (BMPs) or platelet-rich plasma, combined with extremely rigid plate fixation.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Sural Nerve Neuritis | 5% - 10% | Iatrogenic injury during lateral approach for MDCO or Evans osteotomy. | Initial: Gabapentinoids, desensitization. Late: Surgical neurolysis or neurectomy with muscle burying. |
| Talonavicular Nonunion | 5% - 15% | Inadequate joint preparation, poor compression, smoking, diabetes. | Revision arthrodesis with structural autograft and rigid locked plating. |
| Lateral Column Overload | 10% - 20% | Over-lengthening of the lateral column (Evans > 10mm), uncorrected equinus. | Orthotic offloading. Surgical: Hardware removal, partial wedge resection. |
| Hardware Prominence | 15% - 25% | Prominent screw heads at the heel (MDCO) or medial column plates. | Simple hardware removal after radiographic confirmation of bony union (typically > 6 months). |
| Recurrent Deformity | 5% - 10% | Failure to recognize/treat equinus contracture, spring ligament failure, FDL stretch. | Conversion of failed joint-sparing reconstruction to a rigid Triple Arthrodesis. |



Lateral column overload is a specific and highly morbid complication associated with the Evans calcaneal lengthening osteotomy. If the graft inserted is too large (typically exceeding 10 mm), it drastically increases the pressure across the calcaneocuboid joint, leading to intractable lateral foot pain and rapid degeneration of the joint. Prevention via precise intraoperative templating and avoiding overcorrection is paramount. If conservative management with custom orthotics fails, salvage may necessitate calcaneocuboid arthrodesis or revision of the osteotomy.
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following PTTI reconstruction is lengthy and requires immense patient compliance. The biological healing of tendon transfers and bony osteotomies dictates a strict, phased progression. Premature weight-bearing is the leading cause of construct failure and recurrent deformity.
Phase I: Maximal Protection (Weeks 0-2)
Immediately post-operatively, the patient is placed in a well-padded, short-leg plaster or fiberglass splint. The foot is immobilized in slight equinus and inversion to remove all tension from the FDL transfer and medial soft-tissue repairs. The patient is strictly non-weight-bearing (NWB). Elevation above the level of the heart is critical to mitigate edema and protect the surgical incisions.
Phase II: Early Mobilization and Bony Healing (Weeks 2-6)
At the two-week mark, sutures are removed. If the incisions are fully healed, the patient is transitioned to a removable CAM boot. The patient remains strictly NWB. For joint-sparing procedures (Stage II), gentle, passive range of motion (ROM) of the ankle and midfoot may be initiated by a physical therapist to prevent crippling arthrofibrosis, specifically focusing on dorsiflexion and plantarflexion while avoiding active eversion. For arthrodesis procedures (Stage III/IV), the foot remains rigidly immobilized without ROM to ensure uninterrupted bony consolidation.
Phase III: Progressive Weight-Bearing and Tendon Retraining (Weeks 6-12)
At six weeks, weight-bearing radiographs are obtained. If there is evidence of bridging callus at the osteotomy sites or consolidation at the arthrodesis interfaces, progressive weight-bearing is initiated. Patients begin at 25% body weight in the CAM boot, advancing by 25% weekly. Physical therapy becomes aggressive. For FDL transfers, neuromuscular re-education is vital. The FDL originally functioned to flex the lesser toes; the brain must be retrained to fire this muscle to invert the hindfoot. Exercises such as "picking up marbles" with the toes while actively attempting to invert the heel are utilized to facilitate this cortical remapping.
Phase IV: Return to Function (Months 3-6+)
By 10 to 12 weeks, patients are transitioned out of the CAM boot into supportive athletic footwear fitted with a custom, rigid medial longitudinal arch support or an AFO. Strengthening of the entire lower extremity kinetic chain, focusing on the gluteus medius, quadriceps, and intrinsic foot musculature, is emphasized. Maximum medical improvement and final functional outcome are rarely achieved before 12 to 18 months post-operatively.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the surgical management of Posterior Tibial Tendon Insufficiency is deeply rooted in several landmark publications that have shaped modern orthopedic guidelines. The seminal work by Johnson and Strom in 1989 first categorized the pathology into three distinct stages, providing the first coherent framework for surgical decision-making. They established that tenosynovectomy was sufficient for Stage I, while Stage II required tendon transfer, and Stage III necessitated arthrodesis.
In 1996, Mark Myerson significantly advanced this classification by recognizing the involvement of the deltoid ligament and the tibiotalar joint, adding Stage IV to the algorithm. Myerson's work highlighted that hindfoot arthrodesis alone would fail catastrophically if ankle valgus instability was ignored. Furthermore, the biomechanical studies by Jonathan Deland in the late 1990s and early 2000s revolutionized our understanding of the spring ligament complex. Deland demonstrated that the PTT does not fail in isolation; the superomedial calcaneonavicular ligament is a critical co-stabilizer, and its repair
