Introduction and Pathoanatomy
Hyperextension deformity of the proximal interphalangeal (PIP) joint is a debilitating condition most frequently encountered as the primary pathology in a swan neck deformity. This kinematic collapse is characterized by PIP joint hyperextension coupled with distal interphalangeal (DIP) joint flexion. The deformity typically arises from a primary attenuation or rupture of the volar plate at the PIP joint, which allows the proximal phalanx to hyperextend. Consequently, the lateral bands of the extensor mechanism subluxate dorsally, altering the moment arm and locking the joint in hyperextension, while the terminal extensor tendon becomes relatively elongated or ruptures, leading to the reciprocal DIP flexion.
The etiology of PIP hyperextension is diverse, encompassing inflammatory arthropathies (predominantly rheumatoid arthritis), traumatic volar plate avulsions, spastic conditions (such as cerebral palsy), and generalized ligamentous laxity (e.g., Ehlers-Danlos syndrome).
The Beckenbaugh technique is a highly effective, soft-tissue reconstructive procedure designed to correct this deformity. By utilizing a slip of the flexor digitorum superficialis (FDS) tendon to create a volar tenodesis, the procedure effectively reconstructs the checkrein function of the deficient volar plate. This textbook-level guide delineates the precise surgical steps, biomechanical rationale, and postoperative protocols required to execute the Beckenbaugh procedure successfully.
Indications and Patient Selection
Proper patient selection is paramount for the success of an FDS tenodesis. The Beckenbaugh technique is primarily indicated for flexible deformities where the articular cartilage remains preserved.
Primary Indications
- Nalebuff Type I Swan Neck Deformity: The PIP joint is flexible in all positions of the metacarpophalangeal (MCP) joint.
- Nalebuff Type II Swan Neck Deformity: PIP joint flexion is limited when the MCP joint is extended (due to intrinsic tightness) but flexible when the MCP is flexed. (Note: Intrinsic release may be required concomitantly).
- Traumatic Volar Plate Incompetence: Chronic, symptomatic hyperextension following a missed or failed conservative treatment of a volar plate injury.
- Ligamentous Laxity: Symptomatic locking or snapping of the PIP joint in patients with hypermobility syndromes.
Contraindications
- Rigid Deformities (Nalebuff Types III and IV): Fixed PIP joint contractures with or without articular destruction. These require joint release, arthrodesis, or arthroplasty.
- Severe Flexor Tendon Tenosynovitis: If the FDS is severely attenuated or ruptured due to rheumatoid disease, it cannot provide a robust tenodesis.
- Incompetent A2 Pulley: The technique relies on a structurally sound A2 pulley to act as the proximal anchor for the tenodesis.
Clinical Pearl: Always assess the integrity of the FDS tendon preoperatively. In advanced rheumatoid arthritis, spontaneous rupture of the FDS may have occurred, rendering this specific tenodesis technique impossible. In such cases, alternative procedures like lateral band mobilization or dermodesis must be considered.
Preoperative Planning and Positioning
- Anesthesia: The procedure can be performed under regional block (axillary or supraclavicular brachial plexus block) or wide-awake local anesthesia no tourniquet (WALANT). WALANT is particularly advantageous as it allows for intraoperative active movement to assess the tension of the tenodesis and ensure the elimination of the hyperextension deformity.
- Positioning: The patient is placed supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: If WALANT is not utilized, a well-padded pneumatic upper arm tourniquet is applied and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
- Preparation: Standard surgical preparation and draping of the hand and forearm are performed. Multiple digits can be operated on during a single sitting if required.
Surgical Anatomy of the Flexor Sheath
A profound understanding of the digital flexor sheath is required to navigate this procedure safely. The flexor tendon pulley system consists of five annular (A1-A5) and three cruciate (C1-C3) pulleys.
* A2 Pulley: Arises from the proximal phalanx and is critical for preventing bowstringing. The Beckenbaugh technique utilizes the robust distal portion of the A2 pulley as an anchor.
* C1 Pulley: Located between the A2 and A4 pulleys, overlying the PIP joint. This is the site of surgical entry to access the flexor tendons.
* Camper's Chiasm: The decussation of the FDS tendon over the proximal phalanx, where it splits to allow the flexor digitorum profundus (FDP) to pass superficially before the FDS slips insert into the middle phalanx.
Detailed Surgical Technique: The Beckenbaugh Procedure
1. Incision and Exposure
The operation begins with a meticulous approach to the volar aspect of the digit.
Make a volar zigzag (Bruner) incision centered over the PIP joint. The apices of the flaps should reach the midaxial lines to provide adequate exposure without creating scar contractures across the flexion creases.
Surgical Warning: Extreme caution must be exercised during the elevation of the skin flaps. In chronic hyperextension deformities, the digital neurovascular bundles are often displaced volarly and may adhere tightly to the attenuated pulley system and volar plate. Dissect bluntly and identify the neurovascular bundles early.
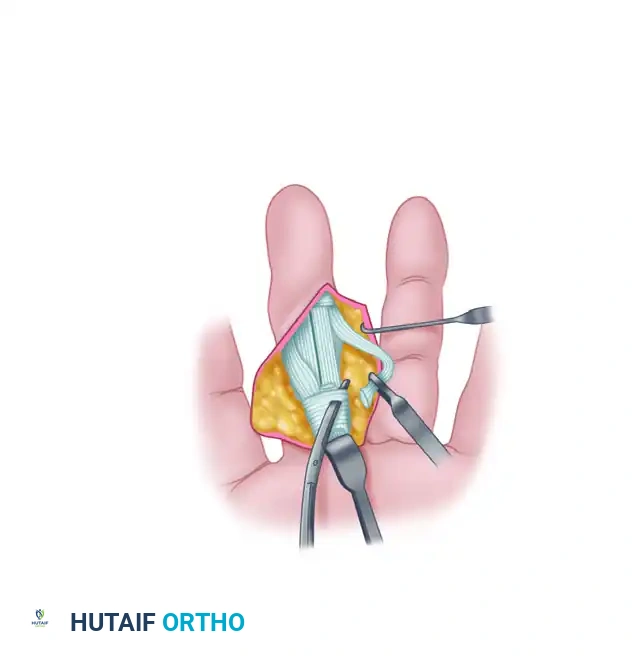
2. Pulley System Identification
Once the skin flaps are elevated, expose the underlying flexor tendon pulley system over the proximal and middle phalanges. This is achieved by carefully mobilizing and retracting the neurovascular bundles medially and laterally using blunt retractors or vessel loops.
Identify the distinct transverse fibers of the A2 pulley over the proximal phalanx and the A4 pulley over the middle phalanx.
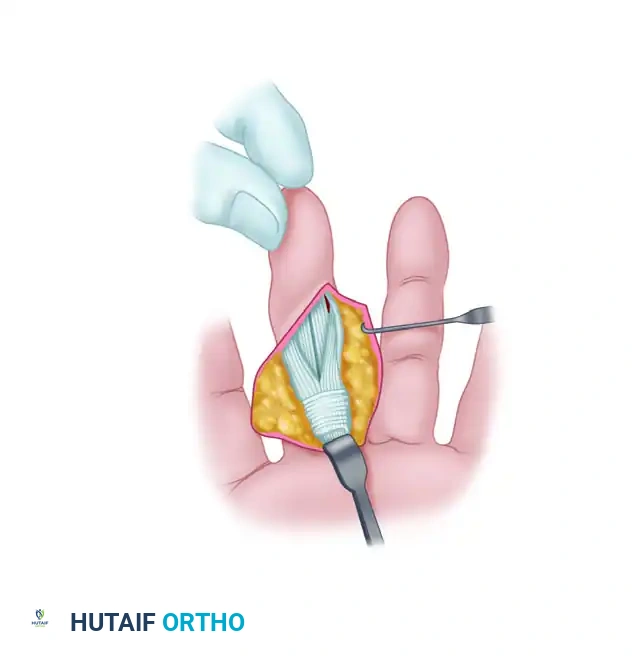
3. Tendon Exposure and Synovectomy
Locate the first cruciate (C1) pulley, which lies in the interval between the distal end of the A2 pulley and the proximal end of the A4 pulley. Incise the C1 pulley to open the flexor tendon sheath and expose the underlying flexor tendons.
Retract the flexor digitorum profundus (FDP) tendon laterally to expose the underlying flexor digitorum superficialis (FDS) tendon. In patients with inflammatory arthropathies, extensive tenosynovitis is often present. Perform a meticulous synovectomy, releasing any adhesions that may tether the FDS or FDP tendons, ensuring smooth, unhindered excursion.
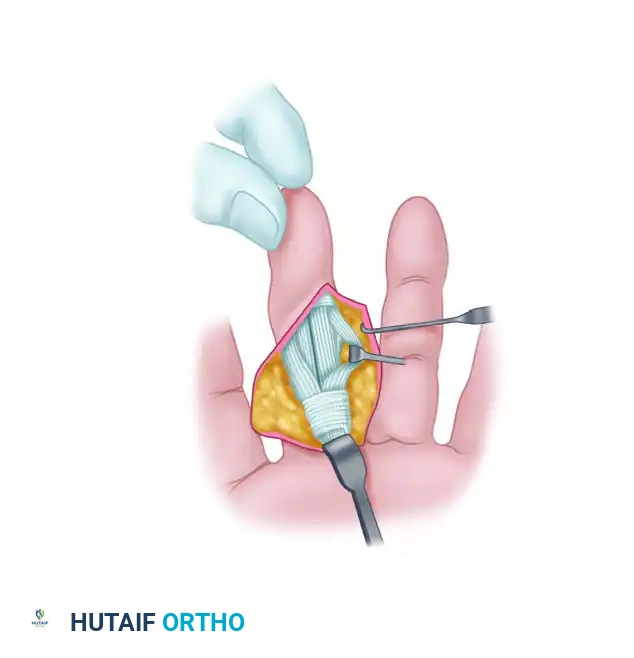
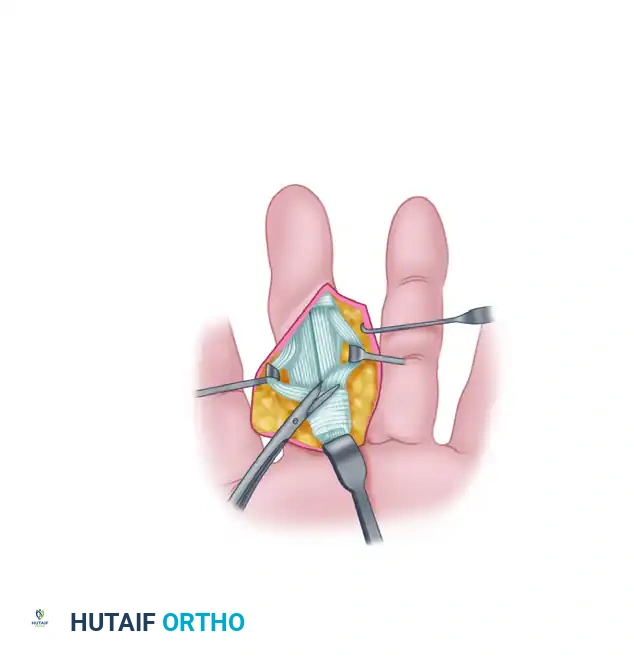
4. Preparation of the Flexor Digitorum Superficialis Slip
Apply distal traction to the FDS tendon to bring Camper's chiasm into view. Incise the decussation longitudinally, effectively splitting the FDS tendon into its two distinct radial and ulnar slips.
Pull the divided FDS tendon distally. Isolate and incise the ulnar slip proximally, ensuring you leave a robust 5-cm slip of tendon that remains firmly attached to its anatomical insertion on the ulnar aspect of the middle phalanx.
Clinical Pearl: After isolating the 5-cm ulnar slip, pull it firmly with forceps. This stress test is critical to ensure that its insertion into the middle phalanx has not been weakened or compromised by chronic synovitis. If the insertion is avulsed during testing, the radial slip must be utilized, or a suture anchor must be placed into the middle phalanx to secure the slip.
Special Consideration for the Little Finger: In the fifth digit, the FDS tendon is anatomically diminutive and occasionally absent. A single slip is usually insufficient to withstand the mechanical forces of tenodesis. Therefore, in the little finger, both the radial and ulnar slips must be incised and utilized together to create a composite, stronger tenodesis.
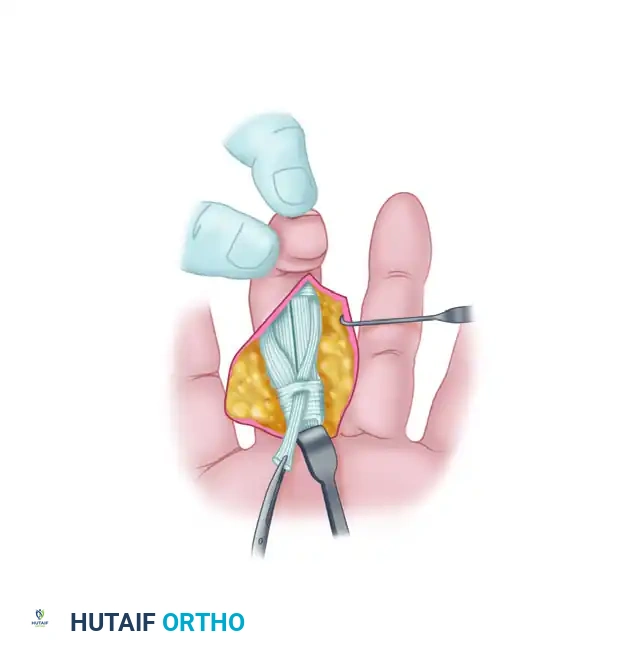
5. Modification of the A2 Pulley
Attention is now turned to the A2 pulley, which will serve as the proximal anchor for the tenodesis. Using a #15 blade, carefully puncture a small hole in the volar aspect of the A2 pulley, approximately 3 to 4 mm proximal to its distal border.
Ensure the puncture is central and does not compromise the structural integrity of the lateral insertions of the pulley to the proximal phalanx.
6. Routing the FDS Slip
Pass a small, curved hemostat (such as a mosquito forceps) through the newly created hole in the A2 pulley, directing the tip distally into the flexor sheath.
Grasp the free proximal tip of the prepared FDS ulnar slip with the hemostat. Gently pull the tendon slip proximally, routing it through the hole in the A2 pulley from inside out.
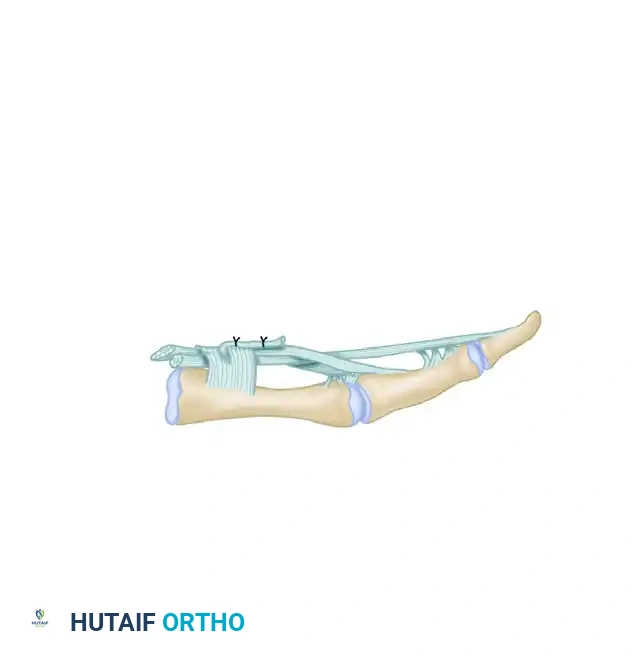
7. Tenodesis Fixation and Tensioning
Bring the routed slip of the FDS tendon distally, folding it back upon itself. This creates a robust loop around the distal 3 to 4 mm of the A2 pulley.
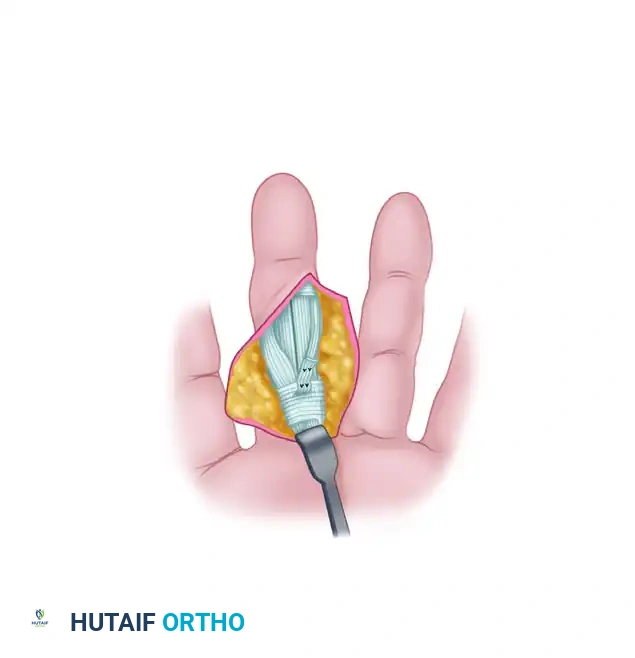
The critical step of tensioning now occurs. Adjust the tension on the folded tendon slip so that the PIP joint is held statically at exactly 5 degrees of flexion.
Once the optimal tension is achieved, suture the tendon slip to itself using multiple interrupted nonabsorbable 4-0 sutures (e.g., braided polyester or polypropylene).
This configuration establishes a permanent tenodesis across the volar aspect of the PIP joint, effectively acting as a checkrein ligament that prevents hyperextension while allowing full active flexion.
8. Closure and Management of Concomitant Deformities
After securing the tenodesis, evaluate the flexor sheath. If feasible and without causing constriction, repair the C1 cruciate pulley using fine absorbable sutures to restore the gliding surface.
Addressing the DIP Joint:
In a classic swan neck deformity, the DIP joint is fixed in a flexed position. If the DIP joint remains flexed after correcting the PIP hyperextension, it must be addressed to restore full digital balance. Manipulate the DIP joint into neutral extension. If it is passively correctable, pin the DIP joint in extension using a 0.035-inch or 0.045-inch Kirschner wire (K-wire) driven longitudinally across the joint. This pin should be left in place for 3 weeks.
Wound Closure:
Deflate the tourniquet and achieve meticulous hemostasis. Close the skin flaps using 5-0 nonabsorbable monofilament sutures. If significant dead space or oozing is present, a small volar drain may be placed.
Apply a sterile, non-adherent dressing followed by a bulky soft bandage. Crucially, support the digit with a dorsal blocking splint fabricated to hold the PIP joint in 10 to 15 degrees of flexion, absolutely preventing any postoperative hyperextension that could compromise the tenodesis.
Postoperative Care and Rehabilitation Protocol
The success of the Beckenbaugh procedure relies heavily on a strict, well-monitored postoperative rehabilitation protocol. The goal is to allow the tenodesis to heal securely while preventing restrictive flexor tendon adhesions.
Phase 1: Early Healing (Days 1 to 21)
- Day 3: The bulky surgical dressing is removed. The wound is inspected, and a lighter dressing is applied.
- Splinting: A custom thermoplastic dorsal blocking splint is fabricated. The splint must hold the MCP joints in neutral to slight extension and the PIP joints in 10 to 15 degrees of flexion.
- Motion: Active and active-assisted flexion of the PIP and DIP joints is initiated within the constraints of the dorsal blocking splint. Passive extension is strictly prohibited.
- DIP Management: If a K-wire was placed across the DIP joint, it remains in situ, and DIP motion is deferred until pin removal.
Phase 2: Intermediate Phase (Weeks 3 to 6)
- Week 3: If applicable, the DIP joint K-wire is removed, and active DIP motion is commenced.
- Splinting: The dorsal blocking splint is continued during the day for high-risk activities and is worn strictly as a static splint at night to hold the MCP joints in extension and the PIP joints in slight flexion.
- Therapy: Gentle active extension is allowed up to the limit of the splint (which blocks the final 10 degrees of extension). Scar massage and edema control are emphasized.
Phase 3: Maturation Phase (Weeks 6 to 12)
- Week 6: The daytime dorsal blocking splint is discontinued. The night splint is maintained for an additional 2 to 4 weeks depending on the stability of the joint.
- Therapy: Progressive strengthening is initiated. Patients are monitored closely for any signs of recurrent hyperextension. If the PIP joint begins to hyperextend beyond neutral, daytime extension-block splinting (e.g., a figure-of-eight ring splint) is immediately reinstituted.
Complications and Pitfalls
While highly effective, the Beckenbaugh technique carries specific risks that the orthopedic surgeon must anticipate and mitigate.
- Recurrent Hyperextension: This is the most common complication, usually resulting from inadequate initial tensioning of the FDS slip, failure of the suture construct, or premature aggressive extension therapy. Salvage may require revision tenodesis or, ultimately, PIP joint arthrodesis.
- Flexion Contracture: Over-tensioning the FDS slip (securing it in more than 10-15 degrees of flexion) can lead to a fixed PIP flexion contracture. While a 5-degree contracture is the goal, anything exceeding 15 degrees can impair grip mechanics and require surgical release.
- Tendon Rupture: In rheumatoid patients, utilizing a severely diseased FDS slip can lead to postoperative rupture of the tenodesis. Rigorous intraoperative stress testing of the tendon insertion is mandatory.
- Digital Nerve Injury: The zigzag incision places the volarly subluxated digital nerves at high risk. Meticulous blunt dissection and continuous visualization are required.
- Swan Neck Recurrence via DIP Pathology: Failure to address a concomitant mallet deformity at the DIP joint can lead to recurrent imbalance of the extensor mechanism, eventually placing undue stress on the PIP tenodesis and causing late failure.
Conclusion
The Beckenbaugh technique remains a cornerstone in the surgical armamentarium for correcting flexible PIP joint hyperextension deformities. By meticulously utilizing the FDS tendon to reconstruct the volar checkrein mechanism, surgeons can restore digital kinematics, improve grip strength, and alleviate the functional deficits associated with swan neck deformities. Strict adherence to the anatomical principles of the flexor sheath, precise tensioning of the tenodesis, and a rigorously controlled postoperative rehabilitation protocol are the absolute prerequisites for achieving excellent, long-lasting clinical outcomes.
