Comprehensive Introduction and Patho-Epidemiology
Shoulder arthroscopy presents unique physiological, hemodynamic, and anatomical challenges compared to arthroscopic procedures of the knee, ankle, or wrist. The tissue planes penetrated by the arthroscope and working instruments—specifically the deltoid muscle, the rotator cuff, and the thick, highly reactive subacromial bursal tissues—are substantially thicker and more highly vascularized than the relatively thin, avascular capsule of the knee. Consequently, maintaining a pristine visual field requires a meticulous, multimodal approach to hemostasis, fluid management, and precise portal placement. The evolution of shoulder arthroscopy from a purely diagnostic modality to a highly advanced reconstructive field has necessitated a parallel evolution in our understanding of intraarticular fluid dynamics and extraarticular fluid extravasation.
For the practicing orthopedic surgeon, mastering these variables is not merely a matter of operative convenience; it is a fundamental requirement for the safe and reproducible execution of complex procedures such as massive rotator cuff repairs, intricate labral reconstructions, and extensive subacromial decompressions. The shoulder joint's lack of a watertight extraarticular envelope means that pressurized irrigation fluid will inevitably track into the surrounding soft tissues during prolonged cases. Failure to control intraarticular bleeding or mitigate this fluid extravasation can lead to catastrophic, limb- and life-threatening complications, including airway compromise from cervical fluid tracking, deltoid compartment syndrome, and iatrogenic neurovascular injury due to distorted anatomical landmarks.
The epidemiology of shoulder pathologies requiring arthroscopic intervention has expanded exponentially over the past three decades. With an aging, active population and advancements in high-definition arthroscopic imaging, the threshold for arthroscopic intervention has lowered, while the complexity of the procedures has increased. This demographic shift means surgeons are frequently operating on patients with concurrent medical comorbidities, including cardiovascular disease, hypertension, and cerebrovascular insufficiency. These systemic factors directly interact with the local demands of shoulder arthroscopy. For instance, the need for hypotensive anesthesia to maintain visual clarity must be carefully balanced against the patient's baseline cerebral perfusion requirements, particularly when the patient is placed in the upright beach chair position.
Understanding the patho-epidemiology of the subacromial space and glenohumeral joint is critical for anticipating intraoperative challenges. Inflammatory conditions, such as adhesive capsulitis or profound subacromial bursitis, induce profound neoangiogenesis. The hypervascularity of these inflamed tissues dramatically alters the local hemostatic baseline. Capillary beds in a highly inflamed bursa will bleed profusely at standard arthroscopic pump pressures, necessitating dynamic adjustments in fluid inflow, the judicious administration of pharmacologic adjuncts like epinephrine, and the strategic deployment of radiofrequency ablation. Ultimately, the surgeon must approach shoulder arthroscopy not just as a mechanical repair of torn tissues, but as a complex management of a pressurized, dynamic fluid environment within a heavily vascularized soft-tissue envelope.
Detailed Surgical Anatomy and Biomechanics
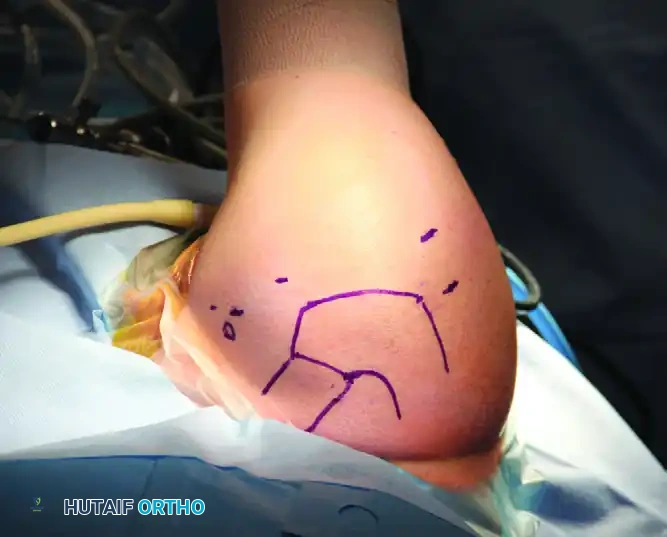
Before establishing any portal or initiating fluid infusion, a rigorous, three-dimensional understanding of the local surface anatomy and underlying neurovascular structures is mandatory. Precise preoperative marking of bony landmarks—the coracoid process, the anterior and posterior margins of the acromion, the acromioclavicular (AC) joint, and the scapular spine—is the first critical step. The shoulder is a highly mobile, unconstrained joint, relying heavily on the dynamic stabilization of the rotator cuff and the static stabilization of the capsuloligamentous complex. The biomechanics of the shoulder dictate that surgical portals must be placed not only to avoid neurovascular injury but also to provide optimal trajectories for suture anchor insertion and instrument manipulation without violating the critical stabilizing structures of the joint.
The two peripheral nerves at highest risk during shoulder arthroscopy are the axillary nerve and the suprascapular nerve. The axillary nerve, a terminal branch of the posterior cord of the brachial plexus, is particularly vulnerable during the placement of anterior, posterior, and lateral working portals. It courses inferior to the glenohumeral joint capsule, exiting the quadrangular space to wind around the surgical neck of the humerus, supplying motor innervation to the deltoid and teres minor. Nassar et al. demonstrated through meticulous cadaveric dissection that the distance from the lateral edge of the acromion to the axillary nerve is approximately 7.9 cm in men and 6.3 cm in women. However, this distance is dynamic and can be significantly reduced depending on arm positioning and the degree of subacromial fluid distension.
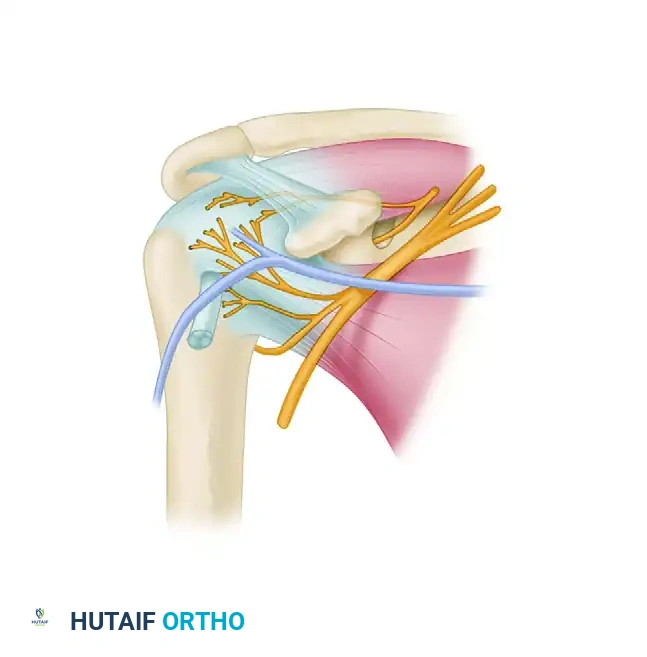
The suprascapular nerve and artery are at significant risk during the placement of posterior and superior accessory portals, particularly the Neviaser (suprascapular) portal. The suprascapular nerve courses through the suprascapular notch, beneath the transverse scapular ligament, and provides motor innervation to the supraspinatus before winding around the spinoglenoid notch to innervate the infraspinatus. Bigliani et al. mapped the suprascapular nerve, finding it located a mere 1.8 cm from the posterosuperior labrum and 2.5 cm from the superior glenoid tubercle. When establishing portals or placing suture anchors in the superior glenoid, the surgeon must remain acutely aware of this proximity to avoid catastrophic denervation of the posterior rotator cuff.
Furthermore, the anterior anatomy presents its own set of hazards. The cephalic vein, which courses through the deltopectoral groove, and the musculocutaneous nerve, which enters the coracobrachialis approximately 5 to 8 cm distal to the coracoid process, dictate the safe zones for anterior portal placement. The low anterior portal (often referred to as the 5 o'clock portal), utilized for inferior capsular work and Bankart repairs, passes perilously close to these structures. It must be established strictly under direct intraarticular visualization using an outside-in technique to ensure the trocar safely traverses the rotator interval without violating the conjoint tendon or the surrounding neurovascular bundle.
Exhaustive Indications and Contraindications
The indications for advanced shoulder arthroscopy encompass a broad spectrum of intraarticular and extraarticular pathologies. Diagnostic arthroscopy remains the gold standard for evaluating intraarticular derangements that are equivocal on magnetic resonance imaging (MRI). Therapeutically, arthroscopy is the primary modality for rotator cuff repairs, superior labrum anterior and posterior (SLAP) repairs, Bankart reconstructions for anterior instability, capsular releases for adhesive capsulitis, and subacromial decompressions. The minimally invasive nature of arthroscopy minimizes deltoid morbidity, accelerates early rehabilitation, and significantly reduces postoperative pain compared to traditional open approaches.
However, the decision to proceed with arthroscopy must be tempered by a thorough understanding of its limitations and contraindications. Severe glenohumeral osteoarthritis with significant bone loss or large osteophytes may physically preclude the insertion of arthroscopic instruments and is generally better served by arthroplasty. Similarly, massive, retracted, and fatty-infiltrated rotator cuff tears in elderly patients may be irreparable arthroscopically and might require superior capsular reconstruction, tendon transfers, or reverse total shoulder arthroplasty. Active local or systemic infection is an absolute contraindication to elective arthroscopy, as the pressurized fluid environment can disseminate the infectious burden through the soft tissue planes.
Surgeons must also carefully evaluate the patient's medical fitness for the specific demands of shoulder arthroscopy. As previously noted, the beach chair position combined with hypotensive anesthesia can severely compromise cerebral perfusion. Therefore, a history of transient ischemic attacks, severe carotid stenosis, or poorly controlled cardiovascular disease represents a strong relative contraindication to this specific operative setup. In such cases, the surgeon must either pivot to the lateral decubitus position or accept higher intraoperative blood pressures, which in turn necessitates superior fluid management and hemostatic techniques to maintain visibility.
| Category | Specific Conditions | Clinical Considerations |
|---|---|---|
| Absolute Indications | Acute traumatic Bankart lesions, symptomatic SLAP tears, full-thickness rotator cuff tears in active patients, septic arthritis (for irrigation and debridement). | Arthroscopy provides superior visualization of the glenohumeral joint and allows for anatomical, minimally invasive repair with less morbidity than open techniques. |
| Relative Indications | Partial-thickness rotator cuff tears, adhesive capsulitis failing conservative management, calcific tendinitis, multidirectional instability. | Conservative management (physical therapy, injections) should typically be exhausted prior to surgical intervention. Outcomes depend heavily on patient compliance. |
| Absolute Contraindications | Active localized soft tissue infection (cellulitis over portals), uncontrolled systemic sepsis, profound medical instability precluding anesthesia. | Pressurized fluid can drive superficial infections deep into the joint or fascial planes. Medical stabilization is paramount. |
| Relative Contraindications | Severe glenohumeral osteoarthritis, massive irreparable rotator cuff tears with advanced fatty infiltration (Goutallier stage 3-4), severe cervical spine stenosis (for beach chair positioning). | Arthroscopy may provide only temporary palliative relief in severe OA. Cervical stenosis increases the risk of spinal cord hypoperfusion in the upright position. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for shoulder arthroscopy begins with a meticulous review of advanced imaging, typically an MRI or MR arthrogram, to precisely define the pathology and anticipate the necessary portal trajectories. Templating the angles required for suture anchor insertion is critical; an anchor placed at an improper angle relative to the glenoid face or the humeral footprint can lead to catastrophic pullout, articular cartilage damage, or inadequate tissue tensioning. The surgeon must mentally map the planned portals to ensure they provide both an unobstructed view of the pathology and a biomechanically sound angle of approach for instrumentation.
The "beach chair" position is widely utilized in shoulder arthroscopy due to its excellent anatomical orientation, ease of conversion to an open procedure if necessary, and the ability to manipulate the arm freely through a physiological range of motion without the constraints of traction. The patient is positioned with the torso elevated to approximately 45 to 60 degrees, the knees slightly flexed to prevent sciatic nerve stretch, and the operative arm draped free. This upright posture leverages gravity to assist with venous drainage, naturally reducing venous bleeding in the surgical field and aiding in the clearance of the subacromial space.

However, the beach chair position introduces profound anesthetic complexities that must be managed collaboratively by the surgeon and the anesthesiologist. The upright posture creates a significant hydrostatic gradient between the heart and the brain. When utilizing the beach chair position, it is imperative to account for the discrepancy between the blood pressure measured at the brachial artery (or calf) and the actual cerebral perfusion pressure (CPP). For every inch of vertical height between the blood pressure cuff and the external auditory meatus, the mean arterial pressure (MAP) decreases by approximately 0.77 mm Hg. In older patients or those with pre-existing cerebrovascular disease, aggressive hypotensive anesthesia in this position can precipitate devastating cerebral ischemia or stroke.
Furthermore, surgeons must be vigilant regarding the Bezold-Jarisch reflex, a physiological response characterized by profound bradycardia and hypotension that can occur in the upright position due to venous pooling in the lower extremities and a hypercontractile, underfilled left ventricle. Mitigating these risks requires meticulous patient positioning, ensuring adequate intravenous hydration prior to elevation, utilizing sequential compression devices on the lower extremities, and maintaining strict parameters for acceptable blood pressure drops. Alternatively, the lateral decubitus position can be employed, which avoids the cerebral perfusion risks of the beach chair position but introduces challenges related to traction neuropraxia and a less intuitive anatomical orientation.
Step-by-Step Surgical Approach and Fixation Technique
The foundation of a successful surgical approach in shoulder arthroscopy is the mastery of hemostasis and fluid management. Without a clear visual field, precise tissue dissection and secure fixation are impossible. An automated arthroscopy pump is essential, typically set to maintain an intraarticular pressure of 60 to 70 mm Hg. Fluid inflow is generally established through the arthroscopy sheath using a high-flow cannula. The physiological impact of this pressurized fluid has been extensively validated; Lee et al. demonstrated that while intramuscular deltoid pressures transiently spike to 50 mm Hg during pump infusion, they normalize rapidly within 30 minutes postoperatively. Similarly, Ogilvie-Harris and Boynton showed that despite peak pressures reaching 120 mm Hg during subacromial work, no electromyographic evidence of ischemic muscle damage occurred, provided the procedure was completed within standard timeframes.
To further optimize the visual field, pharmacologic adjuncts are routinely employed. The addition of epinephrine to the irrigation fluid—typically 1 mL of 1:1000 epinephrine per 3000-mL bag of normal saline or lactated Ringer's—creates a dilute concentration (1:3,000,000) that induces potent alpha-1 adrenergic receptor-mediated vasoconstriction of the local capillary beds. Coupled with controlled hypotensive anesthesia (maintaining a systolic blood pressure between 90 and 100 mm Hg), this establishes a critical systolic-to-pump pressure gradient of approximately 30 mm Hg. This gradient effectively tamponades capillary bleeding without requiring dangerously high intraarticular fluid pressures that exacerbate extravasation.
Portal placement is the next critical phase of the surgical approach. The posterior portal serves as the primary viewing portal and the universal starting point. Located in the "soft spot" 1.5 to 3.0 cm inferior and 1.0 cm medial to the posterolateral tip of the acromion, it exploits a true internervous plane between the infraspinatus and teres minor. The trocar is directed anteriorly and slightly medially toward the coracoid process, piercing the posterior deltoid fascia and the posterior glenohumeral capsule. Once established, this portal provides a panoramic diagnostic view and serves as the visual guide for all subsequent anterior and superior portals.
Anterior portals are established under direct intraarticular visualization using an outside-in technique with a spinal needle to confirm the trajectory. The standard anterior portal is located within the rotator interval, safely bounded by the biceps tendon superiorly and the subscapularis tendon inferiorly. For inferior capsular work, the low anterior (5 o'clock) portal is utilized, requiring extreme caution due to its proximity to the axillary nerve and cephalic vein. Superior portals, such as the Neviaser portal, are highly useful for SLAP repairs and superior anchor trajectories. Fixation techniques rely entirely on these portal trajectories; for instance, inserting a suture anchor into the anterior glenoid rim requires a perfectly perpendicular approach through the anterior portal to ensure maximum pullout strength and to avoid skiving off the dense cortical bone.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, shoulder arthroscopy carries a distinct profile of intraoperative and postoperative complications, largely driven by the pressurized fluid environment and the proximity of vital neurovascular structures. Fluid extravasation is significantly more problematic in the shoulder than in the knee due to the lack of a robust, watertight capsule around the subacromial space. In a landmark study, Lo and Burkhart documented an average fluid weight gain of 8.7 lbs (approximately 3.9 liters) immediately following shoulder arthroscopy. While much of this fluid is absorbed systemically without issue, massive extravasation can track medially along the fascial planes of the chest and neck, leading to life-threatening tracheal compression and airway compromise.
Neurological complications, while relatively rare, can be devastating. They typically arise from either direct iatrogenic injury during portal placement or indirect traction neuropraxia, particularly when the lateral decubitus position is utilized with excessive arm traction. The axillary nerve is most frequently injured during the establishment of low anterior or posterior accessory portals, while the musculocutaneous nerve can be compromised if anterior portals are placed too medially or inferiorly. Prevention relies on strict adherence to anatomical landmarks and the use of blunt trocars when penetrating the capsule.
Compartment syndrome of the deltoid is an exceedingly rare but highly morbid complication of fluid extravasation. While transient pressure spikes are normal, persistent, severe, out-of-proportion pain accompanied by a tense, non-compressible deltoid in the recovery room warrants immediate clinical suspicion. If compartment pressures remain critically elevated, emergent open fasciotomy of the deltoid is required to prevent irreversible myonecrosis. Furthermore, the historical use of intraarticular bupivacaine pain pumps has been definitively linked to devastating post-arthroscopic glenohumeral chondrolysis, a complication that essentially destroys the articular cartilage and mandates salvage arthroplasty in young patients.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Massive Fluid Extravasation / Airway Compromise | < 1.0% | Prolonged subacromial procedures, high pump pressures, multiple portal re-entries. | Immediate cessation of procedure, delayed extubation, airway observation in ICU. Prevent by using threaded cannulas and minimizing extraarticular time. |
| Neurological Injury (Axillary / Suprascapular) | 1.0% - 2.0% | Errant portal placement, aggressive tissue retraction, excessive traction (lateral decubitus). | Most are neuropraxias that resolve with observation. Direct transection requires microsurgical repair or nerve grafting. Prevent via anatomical mastery. |
| Deltoid Compartment Syndrome | < 0.1% | Extreme fluid extravasation, failure of fluid egress, prolonged operative time. | Emergent open deltoid fasciotomy. Prevent by monitoring deltoid tension intraoperatively and maintaining pump pressures < 70 mm Hg. |
| Post-Arthroscopic Chondrolysis | Historically high, now rare | Intraarticular infusion of local anesthetics (bupivacaine) via continuous pain pumps. | Irreversible cartilage destruction. Salvage requires total shoulder arthroplasty or hemiarthroplasty. Prevent by strictly avoiding intraarticular pain pumps. |
Phased Post-Operative Rehabilitation Protocols
The success of advanced shoulder arthroscopy is intimately tied to the postoperative rehabilitation protocol, which must be carefully phased to protect the surgical repair while preventing the insidious onset of adhesive capsulitis. The immediate postoperative phase (Phase I: Weeks 0-4) is focused on protecting the structural integrity of the repair, managing the profound swelling associated with intraoperative fluid extravasation, and controlling pain. Patients are typically immobilized in a specialized sling or abduction orthosis. Cryotherapy is aggressively utilized to induce local vasoconstriction, reducing hemarthrosis and mitigating the inflammatory cascade. During this phase, the deltoid muscle, which has been subjected to significant hydrostatic distension and transient ischemia, requires time to recover its normal resting tone and contractility.
Phase II (Weeks 4-8) marks the initiation of protected, passive range of motion (PROM). The specific parameters of PROM are dictated by the surgical procedure; for example, following an anterior Bankart repair, external rotation is strictly limited to protect the anterior capsule, whereas following a massive rotator cuff repair, active-assisted motion is delayed to prevent premature tension on the healing tendon-to-bone interface. The physical therapist must be acutely aware of the portal sites, ensuring that aggressive mobilization does not disrupt the healing fascial planes or precipitate superficial wound dehiscence.
Phase III (Weeks 8-12) introduces active range of motion (AROM) and early isometric strengthening. The focus shifts to re-establishing the dynamic force couples of the shoulder, specifically the balance between the anterior and posterior rotator cuff, and the scapulothoracic stabilizers. The subacromial space, having been surgically altered (e.g., via acromioplasty or bursectomy), must be dynamically stabilized by a functional supraspinatus to prevent superior migration of the humeral head and secondary impingement.
Phase IV (Months 3-6+) represents the return to advanced functional activities, sport, or heavy labor. This phase involves plyometric training, advanced proprioceptive exercises, and sport-specific biomechanical retraining. The orthopedic surgeon must conduct serial clinical examinations to verify that the initial goals of hemostasis and anatomical restoration achieved during the arthroscopy have translated into a stable, pain-free, and mechanically sound joint capable of withstanding physiological loads.
Summary of Landmark Literature and Clinical Guidelines
The modern practice of shoulder arthroscopy is built upon a foundation of rigorous biomechanical, physiological, and anatomical research. Understanding this landmark literature is essential for the academic orthopedic surgeon, as it provides the evidence-based rationale for our fluid management protocols, positioning strategies, and portal placements. The physiological impact of pressurized fluid was definitively characterized by Lee et al., who utilized slit catheters to measure intramuscular deltoid pressure in patients undergoing shoulder arthroscopy. Their finding that compartment pressures spike significantly but normalize within 30 minutes postoperatively established the safety profile for automated infusion pumps. This was further corroborated by Ogilvie-Harris and Boynton, whose electromyographic data confirmed the absence of ischemic muscle damage despite high transient subacromial fluid pressures.
The phenomenon of fluid extravasation was quantified in the seminal work by Lo and Burkhart. By meticulously weighing patients immediately pre- and post-operatively, they demonstrated an average fluid weight gain of 8.7 lbs, highlighting the profound capacity of the extraarticular soft tissue envelope to sequester irrigation fluid. This study fundamentally changed how surgeons manage subacromial procedures, emphasizing the absolute necessity of maintaining established portal tracts with threaded cannulas and rubber diaphragm seals to minimize the creation of new, fluid-leaking micro-tracts in the deltoid fascia.
Anatomical safety during portal placement has been defined by several key cadaveric studies. Nassar et al. provided the critical measurements defining the safe zone for the axillary nerve relative to the acromion, dictating the limits of lateral and posterior portal placement. Similarly, Bigliani et al. mapped the precise location of the suprascapular nerve, providing the anatomical boundaries necessary to safely execute superior labral repairs and utilize the Neviaser portal without causing catastrophic denervation of the supraspinatus and infraspinatus.
Finally, current clinical guidelines regarding patient positioning heavily emphasize the anesthetic risks of the beach chair configuration. Following multiple case reports of devastating cerebral ischemic events, consensus statements from orthopedic and anesthesiology societies mandate strict monitoring of cerebral perfusion pressure. The physiological rule of thumb—that mean arterial pressure decreases by 0.77 mm Hg for every inch of vertical height between the cuff and the brain—is now a fundamental tenet of preoperative planning. These guidelines dictate that hypotensive anesthesia must be utilized with extreme caution, and the pressure gradient between the patient's systolic blood pressure and the arthroscopic pump pressure (ideally maintained at approximately 30 mm Hg) remains the critical metric for achieving hemostasis without compromising systemic perfusion.
