Clavicle Fracture: Essential Guide to Your Broken Clavicle
Introduction & Epidemiology
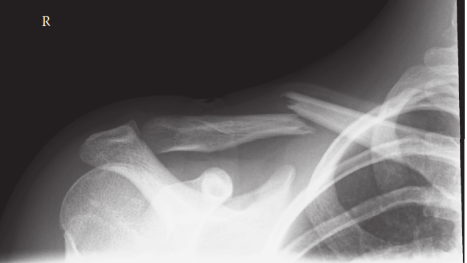
Clavicle fractures are among the most common fractures, accounting for approximately 2.6-10% of all fractures and 35-45% of shoulder girdle injuries. The peak incidence occurs in two distinct populations: young males involved in high-energy trauma (e.g., contact sports, motor vehicle accidents) and elderly females with osteoporotic bone following low-energy falls. The midshaft (diaphyseal) region is involved in 75-80% of cases, followed by the lateral (distal) third (15-20%) and the medial (proximal) third (5%). Understanding the epidemiology is crucial for anticipating patient demographics, injury mechanisms, and potential associated injuries. The increased incidence in young, active individuals often necessitates a meticulous approach to restore function and facilitate an early return to activity.
Surgical Anatomy & Biomechanics
The clavicle is an S-shaped long bone, serving as the sole bony strut connecting the appendicular skeleton of the upper limb to the axial skeleton. Its unique morphology contributes to its susceptibility to fracture and dictates biomechanical considerations for fixation.
Anatomic Zones:
*
Medial Third (Zone 1):
Proximal to the costoclavicular ligament. Fractures here are rare and often associated with high-energy trauma, frequently involving the sternoclavicular joint.
*
Midshaft (Zone 2):
Between the costoclavicular and coracoclavicular ligaments. This is the most common fracture site, often due to direct impact or fall onto the lateral shoulder.
*
Lateral Third (Zone 3):
Distal to the coracoclavicular ligaments, involving the acromioclavicular joint region. These fractures are classified by their relationship to the coracoclavicular ligaments and the integrity of the acromioclavicular joint.
Ligamentous Attachments:
*
Costoclavicular Ligament (Rhomboid Ligament):
Connects the medial clavicle to the first rib, providing significant sternoclavicular joint stability.
*
Coracoclavicular Ligaments:
Comprise the conoid and trapezoid ligaments, connecting the clavicle to the coracoid process. These are critical for suspending the scapula and resisting superior displacement of the lateral clavicle. The conoid is posteromedial, resisting superior and posterior rotation; the trapezoid is anterolateral, resisting superior and anterior rotation.
*
Acromioclavicular Ligaments:
Provide direct stability to the acromioclavicular joint.
Muscular Attachments:
*
Medial:
Sternocleidomastoid (superior), pectoralis major (inferior).
*
Midshaft:
Deltoid (superior, lateral), pectoralis major (inferior, medial). Subclavius muscle lies inferiorly, protecting neurovascular structures.
*
Lateral:
Deltoid (superior), trapezius (superior).
Neurovascular Proximity:
The inferior aspect of the clavicle overlies critical neurovascular structures within the thoracic outlet, including the subclavian artery and vein, and the brachial plexus. Fractures with severe displacement or callus formation can potentially compromise these structures. The supraclavicular nerves (branches of the cervical plexus) course superficially over the clavicle, making them vulnerable during surgical approaches.
Biomechanics:
The clavicle acts as a fulcrum, allowing maximal range of motion for the upper extremity. It transmits forces from the upper limb to the axial skeleton and protects the neurovascular structures. A fracture disrupts this bony strut, leading to shortening, superior displacement of the proximal fragment due to sternocleidomastoid pull, and inferior/anterior displacement of the distal fragment due to arm weight and pectoralis/latissimus dorsi pull. Loss of clavicular length compromises shoulder function, leading to a narrower shoulder girdle, potential scapular dyskinesis, and altered glenohumeral biomechanics.
Indications & Contraindications
The decision between operative and non-operative management of clavicle fractures has evolved significantly. While historically most were treated non-operatively, a growing body of evidence supports operative fixation for specific fracture patterns to improve functional outcomes, reduce nonunion rates, and hasten recovery.
Indications for Operative Fixation:
Absolute Indications:
*
Open fractures:
Require emergent irrigation, debridement, and stabilization to prevent infection.
*
Neurovascular compromise:
Fractures associated with signs of brachial plexus injury, subclavian artery/vein injury, or impending vascular compromise.
*
Skin tenting/impending skin compromise:
Severe displacement threatening skin integrity.
*
Polytrauma patient:
Facilitates early mobilization and rehabilitation, simplifying nursing care.
*
Floating shoulder:
Ipsilateral clavicle and scapular neck fracture, leading to unstable shoulder girdle.
Relative Indications (Midshaft Fractures):
*
Significant displacement:
Defined as >100% cortical apposition loss or complete displacement (no cortical contact).
*
Significant shortening:
Typically >15-20 mm (some literature suggests >2 cm in dominant arm or highly active individuals).
*
Comminution:
Extensive comminution, particularly if associated with shortening or displacement.
*
Specific fracture patterns:
Z-type fractures, butterfly fragments, or segmental fractures.
*
High-demand patients:
Athletes, manual laborers, or individuals desiring an early return to full function.
*
Symptomatic nonunion/malunion:
Persistent pain, weakness, or cosmetic deformity.
*
Bilateral clavicle fractures:
To facilitate overall recovery and function.
Relative Indications (Lateral Third Fractures):
*
Displacement associated with coracoclavicular ligament disruption:
Neer Type II fractures (IIA: conoid intact, trapezoid detached; IIB: conoid detached, trapezoid intact; IIB modified: both detached but no significant fragment inferiorly). These are unstable and prone to nonunion.
*
Displaced intra-articular acromioclavicular joint fractures.
*
Fractures extending into the acromion or scapular spine.
Relative Indications (Medial Third Fractures):
*
Significant displacement or instability:
Due to strong muscular attachments and proximity to vital structures, careful consideration is warranted.
*
Associated sternoclavicular joint dislocation.
Contraindications for Operative Fixation:
Absolute Contraindications:
*
Active infection:
In the operative field.
*
Severe uncontrolled comorbidities:
That preclude safe anesthesia and surgery.
Relative Contraindications:
*
Non-displaced, stable fractures:
Especially midshaft, which have excellent healing rates with non-operative management.
*
Poor soft tissue envelope:
Pre-existing skin conditions or compromised skin from trauma.
*
Elderly, low-demand patients:
With significant comorbidities where surgical risks may outweigh benefits.
*
Patient refusal:
After thorough informed consent.
Operative vs. Non-Operative Indications: A Summary
| Feature | Operative Indications | Non-Operative Indications |
|---|---|---|
| Fracture Type |
- Midshaft: >100% displacement, >15-20mm shortening, extensive comminution, Z-type, segmental, impending skin compromise.
- Lateral: Neer Type II (IIA, IIB, modified IIB), displaced intra-articular AC fractures. - Medial: Significant displacement/instability, associated SC joint dislocation. |
- Midshaft: Non-displaced, minimally displaced, or shortened <15mm.
- Lateral: Neer Type I, III (non-displaced distal to CC ligaments). - Medial: Non-displaced, stable. |
| Associated Injuries | - Open fractures, neurovascular compromise, floating shoulder, polytrauma. | - Isolated fracture with no neurovascular injury. |
| Patient Factors | - High-demand individuals (athletes, laborers), bilateral fractures, symptomatic nonunion/malunion. | - Low-demand individuals, elderly with significant comorbidities where surgical risk outweighs benefit, poor soft tissue envelope. |
| Specific Conditions | - Nonunion (symptomatic), malunion (symptomatic, cosmetic). | - None. Nonunion or symptomatic malunion become operative indications. |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is critical to ensure a successful outcome and minimize complications.
Pre-Operative Planning:
-
Clinical Assessment:
- Detailed history of injury mechanism, hand dominance, occupation, and functional demands.
- Thorough neurovascular examination, documenting any pre-existing deficits or signs of injury (e.g., absent pulses, paresthesias, motor weakness).
- Assess skin integrity for open wounds, tenting, or blistering.
- Evaluate for associated injuries (e.g., rib fractures, pneumothorax, scapular fracture, brachial plexus injury, AC/SC joint injury).
-
Imaging:
- Standard Radiographs: True AP, 30-45 degree cephalic tilt view (serendipity view), and potentially lateral views. These are essential for assessing fracture pattern, displacement, shortening, and comminution.
- Computed Tomography (CT) Scan: Highly recommended for complex fractures, particularly involving the medial or lateral third, to evaluate joint involvement, comminution, displacement, and relationship to neurovascular structures. A CT angiogram may be indicated if vascular injury is suspected.
- Magnetic Resonance Imaging (MRI): Rarely indicated acutely, but may be useful in chronic cases to assess soft tissue damage or for suspected brachial plexus avulsion.
-
Implant Selection:
-
Plating:
Most common fixation method. Precontoured clavicle-specific locking plates (superior or anteroinferior) are preferred.
- Superior plating: Offers high biomechanical stability due to its broad surface and resistance to bending forces. However, hardware prominence can be an issue.
- Anteroinferior plating: May reduce hardware prominence but requires more precise contouring and careful attention to screw length to avoid neurovascular structures. Less biomechanically robust than superior plating for some fracture patterns.
- Intramedullary (IM) Nailing: Less common for midshaft fractures due to inferior rotational control and higher rates of hardware complications/re-operation compared to plating. May be considered for less comminuted fractures with limited soft tissue stripping.
- Suture anchors/Coracoclavicular screws: For unstable lateral clavicle fractures (Neer Type II) involving coracoclavicular ligament disruption, often used in conjunction with a plate.
-
Plating:
Most common fixation method. Precontoured clavicle-specific locking plates (superior or anteroinferior) are preferred.
-
Templating: Use radiographs or CT reconstructions to estimate plate length, number of screws required, and ideal screw trajectory.
-
Anesthesia Considerations: Regional block (interscalene or supraclavicular) can provide excellent post-operative pain control, but care must be taken with distorted anatomy. General anesthesia is typically employed.
Patient Positioning:
- Beach Chair Position: Preferred by many surgeons. Allows for easier access to the entire clavicle, good visualization of shoulder girdle motion, and ability to assess reduction dynamically. The patient's head should be secured and slightly turned away from the operative side. Ensure adequate padding to prevent pressure injuries.
- Supine Position with a Shoulder Bump: An alternative, particularly if a posterior approach for other associated injuries is anticipated. A rolled towel or beanbag beneath the ipsilateral scapula helps elevate the shoulder, bringing the clavicle into a more horizontal position, allowing for optimal access to the superior aspect.
- Arm Positioning: The ipsilateral arm should be free-draped and placed on an arm board or surgical table. This allows for manipulation during reduction maneuvers and assessment of length.
Detailed Surgical Approach / Technique
The goal of surgical fixation is anatomical reduction of the fracture fragments, restoration of clavicular length, and rigid internal fixation to allow for early motion and rehabilitation.
Midshaft Clavicle Fractures (Zone 2) - Plate Osteosynthesis:
-
Incision:
- A transverse or slightly oblique incision centered over the fracture site is typically used, following Langer's lines to optimize cosmetic outcome. A length of 5-8 cm is usually sufficient.
- Carefully incise the skin and subcutaneous tissue. Identify and protect the supraclavicular nerves, which run obliquely over the clavicle. These nerves are often sacrificed or retracted, leading to an area of numbness inferior to the incision, which should be discussed pre-operatively.
-
Dissection:
- Incise the platysma muscle (if present in the medial aspect) in line with the skin incision.
- Carefully dissect through the subcutaneous fat and fascia down to the clavicle. Subperiosteal dissection is generally preferred to preserve the blood supply to the fragments, especially in comminuted fractures. However, excessive stripping should be avoided.
- Identify the fracture ends. Clear any intervening hematoma or soft tissue from the fracture site.
-
Reduction:
- Restore length, alignment, and rotation. This is a critical step.
- Indirect Reduction: Traction on the ipsilateral arm, combined with manual manipulation of the fragments. A small towel bump under the scapula can assist.
- Direct Reduction: Use reduction clamps (e.g., Verbrugge, pointed reduction clamps) to grasp the proximal and distal fragments and bring them into anatomical alignment. Provisional K-wire fixation can be used to hold the reduction, ensuring it is well away from the intended plate path.
- Ensure appropriate rotational alignment by aligning the superior and inferior cortical surfaces. Significant shortening, angulation, or malrotation can lead to functional deficits.
-
Fixation (Superior Plating):
- Plate Selection: Choose a precontoured locking compression plate (LCP) specific for the clavicle. The plate should be long enough to allow for at least three bicortical screws on each side of the fracture site, engaging dense cortical bone.
- Plate Placement: Position the plate on the superior surface of the clavicle. Ensure it is centrally located and does not impinge on the acromioclavicular or sternoclavicular joints.
- Initial Screw Placement: Secure the plate provisionally with K-wires or a single non-locking cortical screw at each end, ensuring the reduction is maintained.
-
Screw Insertion:
- Lag Screws (if applicable): For oblique fractures or butterfly fragments, a lag screw can be inserted prior to or through the plate to achieve interfragmentary compression.
- Locking Screws: These provide angular stability and are crucial for comminuted fractures or osteoporotic bone. Insert locking screws in a staggered fashion, alternating between proximal and distal fragments.
- Cortical Screws: Can be used in non-locking holes for additional compression if needed.
- Screw Length: Precise measurement of screw length is paramount to avoid neurovascular injury inferiorly. Use a depth gauge carefully. Screws should be bicortical but not excessively long. Aim for just through the far cortex.
- Plate Contour: While precontoured plates are common, minor adjustments may be needed to achieve optimal fit. Avoid excessive bending, which can weaken the plate.
Lateral Clavicle Fractures (Zone 3) - Neer Type II:
-
Incision & Dissection: Similar to midshaft, but often extended slightly more laterally, potentially towards the AC joint. Care for supraclavicular nerves.
-
Reduction & Fixation:
- The medial fragment tends to displace superiorly due to sternocleidomastoid pull. The distal fragment is unstable due to disruption of the coracoclavicular ligaments.
- Reduction involves pulling the distal fragment inferiorly and laterally, aligning it with the medial fragment.
-
Plating:
A precontoured hook plate or a lateral clavicle plate with a specific design for distal fixation is often used.
- Hook Plate: The hook engages the posterior-inferior aspect of the acromion, providing a stable platform to compress the distal fragment to the medial fragment. Ensure the hook does not impinge on the rotator cuff. Often temporary (removed at 3-6 months).
- Lateral Clavicle Plate: Utilizes multiple small locking screws into the distal clavicle fragment, potentially augmented with a coracoclavicular suture button or screw.
-
Coracoclavicular Augmentation:
For true Neer Type II fractures with CC ligament disruption, stabilization of the clavicle to the coracoid process is critical. This can be achieved with:
- Suture Button Systems (e.g., Dog Bone, TightRope): Two buttons (one superior on clavicle, one inferior on coracoid) connected by strong sutures, compressing the clavicle to the coracoid. This provides physiological stability.
- Coracoclavicular Screw: A large cortical screw passed through the clavicle into the coracoid. Less common due to rigidity and risk of breakage/loss of reduction.
Medial Clavicle Fractures (Zone 1):
- These are rare and often managed non-operatively. Surgical fixation is challenging due to the complex anatomy of the sternoclavicular joint and proximity to the great vessels.
- If operative, small fragment plates, tension band wiring, or screws may be used, often with careful consultation with thoracic or vascular surgery if great vessels are at risk.
Wound Closure:
- Thorough irrigation of the wound.
- Close the periosteum (if significantly elevated) and deep fascia.
- Close the platysma (if present).
- Subcutaneous fat layer closure.
- Skin closure with absorbable sutures for cosmetic outcome.
- Sterile dressing.
Complications & Management
Complications following clavicle fracture fixation can range from minor hardware irritation to significant functional deficits. Early identification and appropriate management are essential.
| Complication | Incidence | Management / Salvage Strategies The following guidelines are provided for the safe disposal of sharps:
* Place sharps in a puncture-resistant, rigid container immediately after use.
* Do not recap, bend, or break needles.
* Do not overfill sharps containers; observe the fill line.
* Keep sharps containers out of reach of children and pets.
* Dispose of full sharps containers according to local regulations (e.g., mail-back programs, community collection sites, special waste pick-up).
```
Complications and Management
Fractures of the clavicle, while often perceived as benign, are associated with a range of potential complications, particularly following surgical fixation. Comprehensive understanding of these complications is crucial for both prevention and effective management.
| Complication | Incidence | Management / Salvage Strategies Nonunion: Failure of fracture healing after an appropriate time interval (typically 6 months).
- Incidence: Highly variable, ranging from 0.1% to 15% in surgically treated fractures, but significantly higher (up to 30-40%) in specific non-operatively treated fracture patterns (e.g., displaced midshaft, Neer Type II lateral). Risk factors include severe comminution, displacement, shortening, open fracture, inadequate reduction/fixation, poor patient compliance, and specific patient factors (smoking, NSAID use, diabetes, poor nutrition).
-
Management:
- Symptomatic Nonunion: Requires surgical intervention.
- Debridement and Refixation: Remove fibrous tissue at the fracture site, debride sclerotic bone, achieve a fresh bleeding bone bed, re-reduce, and perform rigid internal fixation, often with a longer and stronger plate.
- Bone Grafting: Autogenous bone graft (iliac crest or distal radius) is often indicated, especially in atrophic nonunions, to stimulate healing. Allograft or synthetic bone substitutes can also be considered.
- Revision Plating: May involve changing plate position (e.g., from superior to anteroinferior, or adding an inferior plate for dual plating), or using a stronger plate.
Malunion: Healing of a fracture in a deformed position (shortening, angulation, or rotation).
- Incidence: Very common with non-operative management, especially in significantly displaced or shortened fractures. Symptomatic malunion rates vary from 10-30%.
-
Management:
- Asymptomatic Malunion: No intervention required.
-
Symptomatic Malunion:
(Pain, fatigue, functional limitations, cosmetic deformity, nerve irritation, thoracic outlet symptoms)
- Corrective Osteotomy: Surgical intervention to re-fracture the clavicle through the malunion site, restore length and alignment, and then perform rigid internal fixation. Bone grafting may be necessary.
- Hardware Removal: If hardware is causing impingement or irritation secondary to malunion.
Hardware-Related Complications:
- Incidence: Up to 30-50% in some series, making hardware removal a common secondary procedure (up to 20-30%).
-
Hardware Prominence/Irritation:
The superficial location of the clavicle often leads to palpable hardware, which can cause discomfort, skin irritation, or pain with backpack straps/seatbelts.
- Management: Typically symptomatic hardware removal after fracture union (usually 12-18 months post-op). Anteroinferior plating may reduce this risk compared to superior plating.
-
Plate Breakage:
Indicates persistent nonunion or inadequate initial fixation.
- Management: Revision surgery, often involving plate removal, debridement of nonunion, bone grafting, and re-plating with a stronger construct.
-
Screw Pullout/Loosening:
Can lead to loss of reduction or nonunion.
- Management: Revision surgery with screw replacement or re-plating.
Infection:
- Incidence: Relatively low, <5% for closed fractures, but significantly higher for open fractures.
-
Management:
- Superficial Infection: Oral antibiotics, local wound care.
- Deep Infection (Hardware in situ): Emergent surgical debridement, intravenous antibiotics, and potentially hardware removal if the fracture is united. If fracture is not united, staged approach with aggressive debridement, antibiotic spacers/beads, and delayed definitive fixation once infection is controlled.
- Prophylaxis: Pre-operative antibiotics.
Neurovascular Injury:
- Incidence: Very rare (<1%), but potentially devastating. Can be iatrogenic (during surgery) or related to the initial trauma.
-
Management:
- Pre-existing Injury: Consult vascular/thoracic surgery pre-operatively. May require their presence during the procedure.
- Iatrogenic Injury: Immediate recognition and repair. Meticulous surgical technique, precise screw length measurement, and avoiding excessive inferior dissection are critical preventative measures.
- Brachial Plexus Injury: Can range from transient neurapraxia (e.g., supraclavicular nerve neuropraxia) to permanent deficits. Careful intra-operative identification and protection of superficial nerves. Post-operative neurological deficit warrants immediate investigation (e.g., EMG, nerve conduction studies, MRI) and potential consultation with a neurosurgeon.
Refracture:
- Incidence: Low, 1-3%, but can occur after hardware removal, especially if removal is too early or bone quality is poor.
- Management: Treat as a new fracture, often requiring re-fixation.
Other Complications:
-
Pneumothorax:
Rare, but possible with excessively long screws or deep drilling, especially medially.
- Management: Chest X-ray if suspected; chest tube insertion if significant.
-
Adhesive Capsulitis ("Frozen Shoulder"):
More common with prolonged immobilization or inadequate rehabilitation.
- Management: Aggressive physiotherapy, consider steroid injections or MUA/arthroscopic capsular release if conservative measures fail.
-
Cosmetic Deformity:
More pronounced with non-operative management of displaced fractures.
- Management: Corrective osteotomy for symptomatic patients; hardware removal for prominence.
Post-Operative Rehabilitation Protocols
A structured, progressive post-operative rehabilitation protocol is crucial for optimizing functional recovery, preventing stiffness, and ensuring successful integration of the repaired clavicle into the shoulder girdle. Protocols are individualized based on fracture stability, fixation strength, patient comorbidities, and functional goals.
General Principles:
- Pain Control: Adequate analgesia is essential to facilitate early motion.
- Protection: Sling immobilization is typically used for comfort and protection, especially in the early phase. Duration varies based on fracture stability.
- Progressive Loading: Gradual increase in range of motion (ROM) and strengthening exercises.
- Patient Education: Crucial for adherence and understanding of precautions.
Phased Rehabilitation:
Phase 1: Immediate Post-Operative / Protection Phase (Weeks 0-4/6)
*
Goal:
Protect the repair, reduce pain and swelling, initiate gentle motion.
*
Immobilization:
Arm sling for comfort and protection. May be removed for hygiene and exercises.
*
Activities:
*
Elbow, Wrist, Hand ROM:
Active and passive exercises (e.g., pendulums for shoulder, but very limited).
*
Scapular Mobility:
Gentle scapular retraction and protraction within pain-free range.
*
Pain-Free Passive/Assisted Shoulder ROM:
Limited to ~90 degrees flexion and abduction, external rotation to neutral or slightly past (e.g., external rotation to 30 degrees with arm at side). No active lifting of the arm or weight-bearing through the arm.
*
Avoid:
Lifting, pushing, pulling, carrying anything heavier than a cup of coffee. Avoid reaching behind the back or overhead.
*
Precautions:
No active shoulder abduction or flexion above 90 degrees. No weight-bearing through the arm. No sudden movements.
Phase 2: Early Motion / Controlled Loading Phase (Weeks 4/6 - 10/12)
*
Goal:
Gradually increase ROM, improve muscle activation, and initiate light strengthening.
*
Immobilization:
Discontinue sling as comfort allows.
*
Activities:
*
Active-Assisted ROM:
Progress towards full active ROM of the shoulder in all planes.
*
Active ROM:
Begin gentle active ROM as pain allows.
*
Isometric Strengthening:
Initiate isometric exercises for deltoid, rotator cuff, and periscapular muscles (e.g., shoulder shrugs, gentle internal/external rotation against resistance).
*
Theraband Exercises:
Light resistance bands for external rotation, internal rotation, abduction, and flexion exercises, with good form.
*
Cardiovascular:
Stationary cycling, walking.
*
Precautions:
Still avoid heavy lifting, aggressive pushing/pulling, or high-impact activities. Avoid end-range stretching.
Phase 3: Strengthening / Advanced Loading Phase (Weeks 10/12 - 16/24)
*
Goal:
Restore full strength, endurance, and advanced functional capabilities.
*
Activities:
*
Progressive Resistance Exercises:
Incorporate dumbbells, resistance machines for all major shoulder muscle groups (deltoid, rotator cuff, pectoralis, trapezius, rhomboids, latissimus).
*
Proprioception and Neuromuscular Control:
Exercises using balance boards, unstable surfaces.
*
Sport-Specific Training:
Gradually introduce activities specific to the patient's sport or occupation (e.g., throwing drills, overhead movements, pushing/pulling tasks).
*
Endurance Training:
Continue general cardiovascular fitness.
*
Return to Activities:
* Light work/activity: Often possible by 3 months.
* Return to sport/heavy labor: Typically 4-6 months, provided radiographic union is confirmed, full pain-free ROM is achieved, and strength is >90% of the uninjured side.
*
Precautions:
Monitor for pain or recurrence of symptoms. Emphasize proper technique to prevent overload.
Phase 4: Return to Sport / Maintenance Phase (Month 6 onwards)
*
Goal:
Full, unrestricted return to all activities, including contact sports.
*
Activities:
Continue with strength and conditioning program. Focus on maintaining flexibility and muscle balance.
*
Hardware Removal:
If symptomatic, hardware removal may be considered 12-18 months post-op, once bone healing is robust. A brief period of protection/activity modification may be advised after hardware removal.
Summary of Key Literature / Guidelines
The management of clavicle fractures has undergone a significant paradigm shift over the past two decades, largely driven by a growing body of evidence challenging the traditional dogma of universal non-operative treatment for midshaft fractures.
Midshaft Clavicle Fractures:
*
Early Evidence for Non-operative:
Historically, the majority of midshaft clavicle fractures were treated non-operatively with sling immobilization, boasting high union rates (90-95%). However, this often overlooked rates of symptomatic malunion, persistent pain, and functional deficits.
*
The Canadian Orthopaedic Trauma Society (COTS) Study (2007):
This landmark prospective, randomized controlled trial compared plate fixation to non-operative treatment for displaced midshaft clavicle fractures. It demonstrated significantly improved functional outcomes (DASH scores), lower rates of nonunion (2% vs. 15%), and faster return to function in the operative group. This study was pivotal in shifting the pendulum towards operative management for significantly displaced midshaft fractures.
*
Subsequent Meta-analyses and Systematic Reviews:
Numerous studies have since corroborated the COTS findings, reinforcing the benefits of surgical fixation for displaced and shortened midshaft clavicle fractures in terms of reduced nonunion rates, improved functional scores, and patient satisfaction, despite a higher rate of hardware-related complications requiring removal.
*
Indications Consensus:
Current consensus generally supports operative fixation for midshaft fractures with >100% displacement, >15-20 mm shortening, significant comminution, or impending skin compromise, especially in active, high-demand individuals.
Lateral Clavicle Fractures (Neer Type II):
*
Instability:
Neer Type II fractures are inherently unstable due to the disruption of the coracoclavicular ligaments, which connect the medial fragment to the scapula. This instability predisposes them to high rates of nonunion with non-operative management (up to 30-50%).
*
Operative Preference:
Most literature supports operative fixation for displaced Neer Type II fractures to restore stability and prevent nonunion. Techniques range from hook plates (now less favored due to high removal rates and impingement) to modern lateral clavicle plates combined with coracoclavicular ligament reconstruction using suture buttons.
*
Suture Button Systems:
Recent literature highlights the efficacy of suture button devices (e.g., TightRope, Dog Bone) in stabilizing Neer Type II fractures and achieving anatomical reduction of the clavicle to the coracoid, with good functional outcomes and lower complication rates compared to hook plates.
Medial Clavicle Fractures (Zone 1):
*
Rarity and Non-operative Tendency:
These fractures are rare, and often managed non-operatively due to the typically good healing potential and the surgical challenges related to proximity to mediastinal structures.
*
Surgical Indications:
Operative intervention is reserved for highly unstable fractures, significant displacement threatening neurovascular structures, or open fractures. Surgical fixation is complex and carries higher risks.
Hardware Removal:
*
High Incidence:
Despite the benefits of surgical fixation, hardware prominence and irritation are common (20-50%), leading to hardware removal as the most frequent secondary procedure. This emphasizes the need for meticulous plate placement, low-profile implants, and thorough patient counseling regarding potential for a second surgery.
Current Guidelines:
* Major orthopedic societies (e.g., AAOS, BOA, OTA) acknowledge the shift in management, generally recommending operative fixation for specific fracture patterns (significantly displaced midshaft, unstable lateral clavicle) based on Level I evidence.
* The emphasis is on restoring anatomical length and alignment to optimize long-term shoulder function and minimize symptomatic nonunion or malunion. Non-operative management remains viable for truly non-displaced or minimally displaced fractures across all zones.
