THE EVOLUTION OF CLAVICLE FRACTURE MANAGEMENT
Historically, the vast majority of clavicular fractures were managed nonoperatively, relying on the premise that these fractures universally heal with minimal functional deficit. Traditional nonoperative treatment consisted primarily of a simple sling for comfort, as figure-of-eight splinting has largely been abandoned due to patient discomfort, axillary skin complications, and a lack of proven biomechanical or clinical benefit.
However, critical appraisal of long-term outcomes has identified a distinct subgroup of patients—specifically those with completely displaced midshaft fractures—who experience significantly poorer outcomes than previously recognized. Severe displacement, shortening greater than 2 cm, and comminution are now recognized as potent risk factors for nonunion, malunion, and persistent shoulder dyskinesia.
These biomechanical and clinical concerns prompted the Canadian Orthopaedic Trauma Society (COTS) to initiate a landmark multicenter prospective randomized trial comparing nonoperative treatment with plate fixation for displaced midshaft clavicular fractures. The findings fundamentally shifted the treatment paradigm. Operative treatment resulted in significantly improved functional outcomes (Constant and DASH scores were approximately 10 points higher in the operative group at all time points up to 52 weeks) and drastically lower rates of malunion and nonunion.
Clinical Pearl: Treatment should never be an “all or nothing” approach. It must be individualized, aiming to provide optimal outcomes based on fracture morphology, patient demands, and associated injuries. A frank, evidence-based discussion with the patient regarding the risks of surgery versus the risks of nonunion is mandatory.
Evidence-Based Outcomes and Complication Rates
The data strongly supports operative intervention for displaced fractures. According to comprehensive systematic reviews (e.g., Zlowodzki et al.), the nonunion rate for all displaced fractures treated nonoperatively is approximately 15%, compared to just 2.2% for those treated with plate osteosynthesis and 2.0% for intramedullary pinning.
Furthermore, the COTS trial highlighted a distinct complication profile between the two modalities. Complications occurred in 37% (23 of 62) of patients treated operatively, compared with 63% (31 of 49) of those treated nonoperatively. Notably, the nonoperative group suffered higher rates of nonunion (7 vs. 2), symptomatic malunion requiring further treatment (9 vs. 0), and dissatisfaction with the cosmetic appearance of the shoulder (e.g., "droopy" shoulder, prominent bump). Conversely, the operative group experienced complications inherent to surgery, including hardware irritation requiring removal (5 vs. 0) and incisional numbness (18 vs. 0).
INDICATIONS FOR OPERATIVE TREATMENT
The decision to proceed with Open Reduction and Internal Fixation (ORIF) relies on a combination of absolute and relative indications. The relative indications for primary fixation of midshaft clavicular fractures can be categorized into fracture-specific factors, associated injuries, and patient-specific factors.
Fracture-Specific Indications
- Displacement: Greater than 2 cm of translation (no cortical contact).
- Shortening: Greater than 2 cm, which alters the resting length of the shoulder girdle and impairs rotator cuff biomechanics.
- Comminution: Increasing comminution (greater than 3 fragments), particularly segmental fractures (Z-type fractures).
- Soft Tissue Compromise: Open fractures or impending open fractures where the skin is blanched and under severe tension.
- Clinical Deformity: Obvious clinical deformity associated with scapular malposition and winging at initial examination.
Associated Injuries
- Neurovascular Compromise: Vascular injury requiring repair or a progressive neurological deficit (e.g., brachial plexus compression).
- Polytrauma: Ipsilateral upper extremity injuries or fractures, multiple ipsilateral upper rib fractures, or a “floating shoulder” (ipsilateral surgical neck of scapula fracture).
- Bilateral Injuries: Bilateral clavicular fractures, which severely restrict patient mobility and respiration.
Patient Factors
- Rehabilitation Needs: Polytrauma patients requiring early upper extremity weight-bearing (e.g., crutch use for lower extremity fractures).
- Functional Demands: High patient motivation for rapid return of function, such as elite athletes or self-employed manual laborers.
SURGICAL ANATOMY AND BIOMECHANICS
The clavicle is an S-shaped tubular bone that acts as the sole osseous strut connecting the axial skeleton to the upper extremity. The medial two-thirds are convex anteriorly, while the lateral third is concave anteriorly. The bone transitions from a robust, tubular cross-section medially to a flattened, broad cross-section laterally. This transitional zone in the midshaft is the thinnest portion of the bone, lacks ligamentous support, and is the most frequent site of fracture.
Deforming Forces
Understanding the muscular deforming forces is critical for achieving reduction:
1. Medial Fragment: Pulled superiorly and posteriorly by the sternocleidomastoid (SCM) muscle.
2. Lateral Fragment: Pulled inferiorly by the weight of the arm and medially by the pectoralis major and latissimus dorsi, resulting in the characteristic shortened and displaced deformity.
Neurovascular Proximity
The subclavian vessels and the brachial plexus lie directly posterior and inferior to the middle third of the clavicle. The distance between the posterior cortex of the clavicle and these critical structures can be as little as 10 to 15 millimeters. Plunging with a drill bit or utilizing excessively long screws poses a catastrophic risk of neurovascular injury or pneumothorax.
PREOPERATIVE PLANNING AND POSITIONING
Radiographic Evaluation
Standard evaluation requires an anteroposterior (AP) view and a 15- to 20-degree cephalad tilt view. The cephalad view projects the clavicle above the thoracic cage, providing a clear assessment of superior/inferior displacement and shortening. 3D CT reconstruction is rarely required for midshaft fractures but is invaluable for medial or lateral third fractures with intra-articular extension.
Patient Positioning
The patient is placed in the beach chair position with the head of the bed elevated 30 to 45 degrees. A small bump is placed between the scapulae to allow the shoulder girdle to fall posteriorly, which aids in restoring clavicular length and reducing the fracture.
Surgical Warning: Ensure the head and neck are securely stabilized in a neutral position. Excessive rotation of the head away from the operative site can place undue tension on the brachial plexus.
The entire upper extremity, hemithorax, and neck are prepped and draped free to allow manipulation of the arm during reduction.
SURGICAL APPROACH
Meticulous soft tissue handling is paramount. The clavicle has a precarious periosteal blood supply, and aggressive stripping will inevitably lead to nonunion.
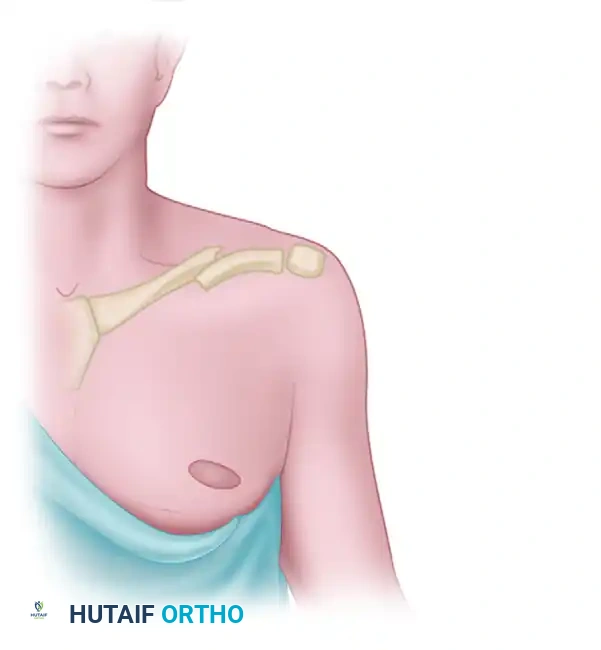
Figure: Incision planning for open reduction and internal fixation of a midshaft clavicular fracture.
- Incision: Make an oblique or curvilinear incision centered over the fracture site, following Langer’s lines when possible to optimize cosmesis. Alternatively, an incision placed slightly inferior to the clavicle can prevent the scar from resting directly over the prominent hardware.
- Superficial Dissection: Incise the platysma in line with the skin incision.
- Nerve Preservation: Carefully identify and protect the branches of the medial supraclavicular nerve. These nerves course perpendicular to the clavicle. While sacrificing a branch is sometimes unavoidable, preserving them significantly reduces the incidence of postoperative anterior chest wall numbness—a common patient complaint (noted in 18 of 62 operative patients in the COTS trial).
- Deep Dissection: Incise the clavipectoral fascia. Perform minimal subperiosteal stripping—only enough to visualize the fracture edges and apply the plate. Leave soft tissue attachments on comminuted butterfly fragments intact to preserve their vascularity.
PLATE OSTEOSYNTHESIS TECHNIQUES
Plating techniques continue to evolve. Historically, 3.5-mm reconstruction plates were utilized because they allowed easy contouring to the S-shape of the clavicle. However, these plates are biomechanically weak and prone to deformation or fatigue failure prior to fracture union. Today, precontoured, anatomically specific locking plates are the gold standard. They provide accurate fitting, superior biomechanical strength, and reduce operative time.
There are two primary locations for plate application: Superior and Anteroinferior.
1. Superior Plate Fixation
Superior placement is the most commonly utilized technique. Biomechanically, the superior surface of the clavicle is the tension side of the bone. Placing the plate on the tension surface provides optimal biomechanical stability, neutralizing the inferior bending forces exerted by the weight of the arm.

Figure: Preoperative radiograph demonstrating a displaced midshaft clavicular fracture suitable for superior plating.
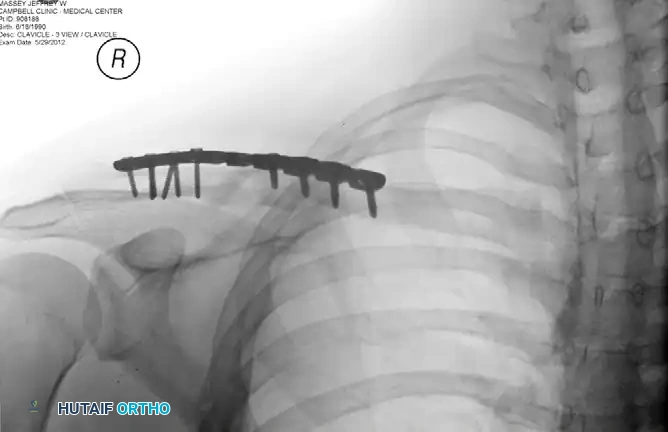
Figure: Postoperative radiograph demonstrating anatomic reduction and fixation with a superiorly placed precontoured plate.
Surgical Steps for Superior Plating:
* Reduction: Clear the fracture site of interposed hematoma and periosteum. Use pointed reduction forceps to achieve anatomic reduction. If a large butterfly fragment is present, it should be reduced and provisionally held with K-wires.
* Lag Screw Fixation: Whenever the fracture pattern allows (e.g., oblique or spiral fractures), insert a 3.5-mm cortical lag screw across the fracture site to provide interfragmentary compression. This screw can be placed independently or through the plate.
* Plate Application: Apply the precontoured superior plate. Ensure the plate spans the fracture adequately, aiming for at least three (preferably four) bicortical screws in both the medial and lateral main fragments.

Figure: The plate must be carefully prebent or selected from an anatomic set to match the normal S-shaped clavicular anatomy.
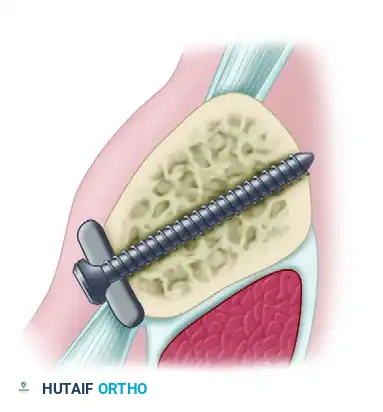
Figure: Screw placement must be directed posteriorly and slightly superiorly to avoid plunging into the neurovascular bundle.
Pitfall: The primary disadvantage of superior plating is hardware prominence. Because there is minimal subcutaneous fat over the superior clavicle, patients frequently complain of irritation from backpack straps or seatbelts, leading to a higher rate of secondary surgeries for hardware removal.
2. Anteroinferior Plate Fixation
When the fracture configuration allows, many master surgeons prefer anteroinferior plate placement. While this is technically the compression side of the bone, modern locking plates provide more than adequate stability to achieve union.
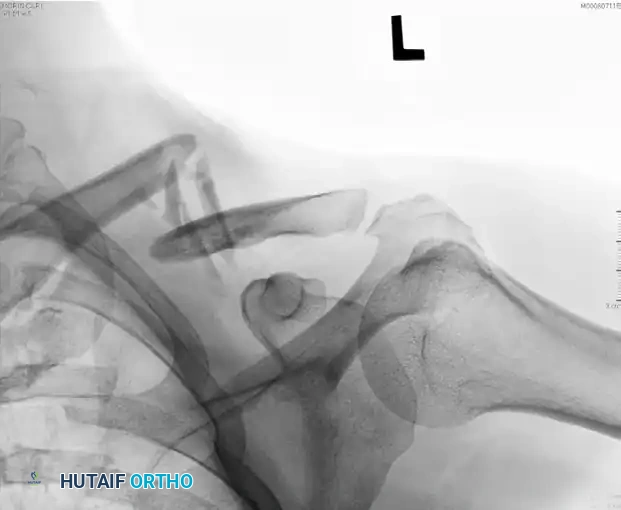
Figure: Preoperative radiograph of a displaced midshaft fracture.

Figure: Postoperative radiograph demonstrating fixation with an anteroinferior plate.
Advantages of Anteroinferior Plating:
1. Safer Screw Trajectory: Screws are directed from anterior to posterior (and slightly superior). This trajectory directs the drill bit away from the subclavian vessels and pleura, drastically reducing the risk of iatrogenic neurovascular injury.
2. Longer Screw Purchase: The AP diameter of the clavicle is often greater than the superior-inferior diameter, allowing for longer screws and improved pull-out strength.
3. Decreased Hardware Prominence: The plate sits beneath the anterior border of the clavicle and is padded by the superior fibers of the pectoralis major, significantly reducing hardware irritation and the subsequent need for plate removal.
Regardless of the plate placement technique used, meticulous attention is mandatory to preserve the periosteum and avoid injury to the subclavian vessels and lungs. A blunt retractor (such as a Darrach or a malleable retractor) should always be placed deep to the clavicle during drilling and tapping to protect the underlying structures.
CLOSURE AND POSTOPERATIVE PROTOCOL
Closure
Thoroughly irrigate the wound to remove bone debris. Obtain meticulous hemostasis. The clavipectoral fascia and platysma must be closed as a distinct layer over the plate using absorbable sutures (e.g., 2-0 Vicryl) to provide soft tissue coverage and reduce hardware prominence. The skin is closed with a running subcuticular suture for optimal cosmesis.
Postoperative Rehabilitation
- Phase I (0 to 2 weeks): The patient is placed in a simple sling for comfort. Pendulum exercises and active range of motion (ROM) of the elbow, wrist, and hand are initiated immediately. Active shoulder elevation is restricted to 90 degrees.
- Phase II (2 to 6 weeks): The sling is weaned. Active and active-assisted ROM of the shoulder is progressed as tolerated. Lifting is restricted to less than 5 pounds.
- Phase III (6 to 12 weeks): Isotonic strengthening is initiated once radiographic evidence of bridging callus is observed.
- Return to Sport: Return to contact sports or heavy manual labor is typically permitted at 3 to 4 months, contingent upon clinical absence of pain and radiographic confirmation of solid bony union.
COMPLICATIONS
While operative intervention significantly reduces the risk of nonunion and malunion, surgeons must be prepared to manage surgical complications:
- Hardware Irritation: The most common complication, particularly with superior plates. Up to 15-20% of patients may request plate removal after fracture consolidation (typically after 12-18 months).
- Incisional Numbness: Injury to the supraclavicular nerves results in an area of anesthesia inferior to the incision. Patients must be counseled preoperatively that this is highly likely, though the area of numbness typically shrinks over 6 to 12 months.
- Infection: Superficial and deep infections occur in 2-4% of cases. Prophylactic intravenous antibiotics and meticulous soft tissue handling are essential.
- Nonunion: Occurs in approximately 2% of operatively treated fractures. It is usually the result of inadequate fixation (e.g., using a weak reconstruction plate), excessive periosteal stripping, or patient non-compliance. Treatment requires revision ORIF with autologous bone grafting.
- Neurovascular Injury: Rare but potentially catastrophic. Strict adherence to safe drilling techniques and the use of protective retractors are non-negotiable.
By adhering to strict biomechanical principles, respecting the soft tissue envelope, and selecting the appropriate fixation strategy, orthopedic surgeons can reliably restore shoulder girdle anatomy and function following displaced clavicular fractures.
