Proximal Femur Fractures: Cephalomedullary Nailing Explained
Key Takeaway
Your ultimate guide to Proximal Femur Fractures: Cephalomedullary Nailing Explained starts here. Proximal femur fractures are grouped into four major types: femoral head, intracapsular femoral neck, pertrochanteric, and subtrochanteric. Cephalomedullary nailing is the surgical stabilization of these fractures using an intramedullary device, typically inserted via the piriformis fossa. It is most commonly indicated for extracapsular peritrochanteric and subtrochanteric proximal femur fractures.
Introduction and Epidemiology
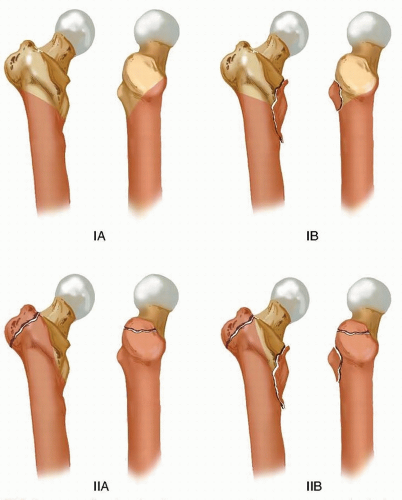
Fractures of the proximal femur represent a massive epidemiological burden and a critical challenge in orthopedic trauma surgery. These fractures are broadly grouped into four major anatomic types reflecting distinct differences in structural anatomy, vascularity, and physiological character. The four regions include femoral head fractures, intracapsular femoral neck fractures, pertrochanteric fractures (encompassing intertrochanteric and peritrochanteric patterns extending from the extracapsular neck to the lesser trochanter), and subtrochanteric fractures.
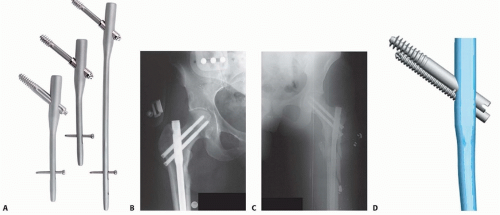
Cephalomedullary nailing is defined as the surgical stabilization of a proximal femur fracture utilizing an intramedullary load-sharing device. The implant is typically inserted antegrade through the piriformis fossa, the tip of the greater trochanter, or slightly medial to the greater trochanter. The cephalic (or femoral head) portion of the construct consists of one or more screws or helical blades that interlock with the intramedullary nail, providing rigid fixation of the proximal segment while allowing controlled sliding and impaction. Cephalomedullary nails are primarily indicated in extracapsular peritrochanteric and subtrochanteric fractures.
The pathogenesis of proximal femur fractures generally falls into three mechanistic categories. The vast majority occur as low energy same level falls in the geriatric population (typically 65 to 90 years of age), intimately associated with osteopenia, osteoporosis, and sarcopenia. A secondary peak occurs in the 18 to 45 year age group, resulting from high energy trauma such as motor vehicle collisions or falls from significant heights. These high energy injuries often present with severe comminution, marked displacement, and associated polytrauma. Finally, pathologic fractures frequently occur in the proximal femur due to high biomechanical stresses, often serving as the initial clinical presentation of a metastatic neoplastic process or primary bone tumor.
The natural history of nonoperatively treated proximal femur fractures is exceedingly poor. To obtain any realistic probability of ambulatory recovery and to mitigate the profound systemic complications of prolonged immobility, surgical treatment is mandatory for complete fractures. Nonoperative management of displaced proximal femur fractures invariably results in significant shortening, varus deformity, chronic pain, and an unacceptably high mortality rate secondary to decubitus ulcers, deep vein thrombosis, pulmonary embolism, and nosocomial pneumonia.
Surgical Anatomy and Biomechanics
The transitional anatomy from the spherical femoral head to the tubular subtrochanteric region dictates the diverse fracture pathogeneses and profoundly influences the surgical approach for osteosynthesis.
Intracapsular fractures of the femoral neck are critically dependent on the tenuous vascular supply derived primarily from the medial femoral circumflex artery. The retinacular vessels traverse the femoral neck to supply the head; disruption of these vessels during fracture displacement or iatrogenic injury during surgical fixation significantly increases the risk of avascular necrosis and nonunion.
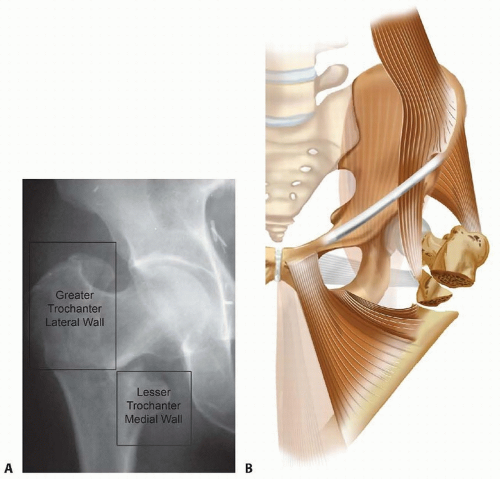
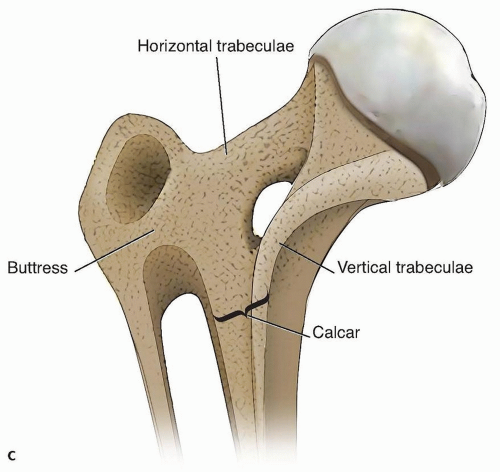
Conversely, the pertrochanteric region is highly vascularized and relies heavily on the structural integrity of a dense cancellous bone network. The primary weight bearing trabeculae form a solid cancellous block extending from the femoral head inferiorly along Ward triangle to the calcar femorale (Adam’s arch). At the level of the lesser trochanter, this dense cancellous architecture transitions into the thick cortical diaphysis, marking the origin of the medullary canal.
Subtrochanteric fractures incur the highest biomechanical stresses in the human skeleton. The medial cortex of the proximal femur is subjected to massive compressive forces, while the lateral cortex experiences significant tensile forces. The moment arm generated by the offset of the femoral head relative to the anatomic axis of the femoral shaft places extraordinary stress on any implant used for fixation.
The muscular attachments surrounding the proximal femur act as powerful deforming forces, complicating fracture reduction and maintenance of alignment. In subtrochanteric fractures, the proximal fragment is classically displaced into flexion, abduction, and external rotation. Flexion is driven by the iliopsoas inserting on the lesser trochanter; abduction is driven by the gluteus medius and minimus inserting on the greater trochanter; and external rotation is driven by the short external rotators inserting in the trochanteric fossa. Simultaneously, the distal fragment is pulled proximally and into adduction by the massive adductor musculature and the hamstrings.
Biomechanically, a cephalomedullary nail acts as a load-sharing device. Because the intramedullary nail is located closer to the mechanical axis of the lower extremity than an extramedullary plate (such as a sliding hip screw), the bending moment exerted on the implant is significantly reduced. This biomechanical advantage makes cephalomedullary nailing the implant of choice for unstable fracture patterns, reverse obliquity fractures, and subtrochanteric fractures where extramedullary devices have an unacceptably high rate of fatigue failure.
Indications and Contraindications
The selection of a cephalomedullary nail over an extramedullary sliding hip screw or arthroplasty depends heavily on the specific fracture pattern, the integrity of the lateral trochanteric wall, and the patient's baseline physiological status. Cephalomedullary nailing has become the gold standard for unstable pertrochanteric fractures, reverse obliquity patterns, and subtrochanteric extensions.
The integrity of the lateral wall is a critical determinant. In fractures where the lateral wall is fractured, thin, or at high risk of iatrogenic fracture during lag screw insertion, a sliding hip screw provides inadequate buttressing, leading to excessive sliding, medialization of the femoral shaft, and construct failure. An intramedullary nail bypasses the lateral wall, providing a rigid medial buttress against which the cephalic screw can slide in a controlled manner.
| Parameter | Operative Indications for Cephalomedullary Nailing | Non Operative Management or Alternative Fixation |
|---|---|---|
| Fracture Pattern | Unstable intertrochanteric, reverse obliquity, subtrochanteric, lateral wall incompetence. | Stable intertrochanteric (Sliding Hip Screw is acceptable), displaced femoral neck (Arthroplasty). |
| Hemodynamic Status | Stable patient optimized for surgical intervention within 24 to 48 hours. | Moribund patient, active myocardial infarction, uncorrectable coagulopathy (Non-operative/palliative). |
| Bone Quality | Osteoporotic bone requiring load-sharing biomechanics. | Severe osteoarthritis of the hip joint with concurrent fracture (Consider Total Hip Arthroplasty). |
| Pathologic Lesions | Impending or complete pathologic fractures of the proximal femur requiring prophylactic stabilization. | Active local infection or osteomyelitis at the surgical site (Contraindication for internal fixation). |
Relative contraindications to cephalomedullary nailing include narrow medullary canals that preclude safe reaming, severe preexisting femoral deformities (such as excessive anterior bowing or malunion from prior trauma), and active local soft tissue infections. In cases of severe osteoarthritis combined with an intertrochanteric fracture, a calcar-replacing total hip arthroplasty may be considered as an alternative to internal fixation to address both the fracture and the degenerative joint disease simultaneously.
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is essential for successful cephalomedullary nailing. High quality orthogonal radiographs, including an anteroposterior view of the pelvis and a cross-table lateral of the affected hip, are mandatory. Full length femur radiographs are required to assess the medullary canal diameter, the anterior radius of curvature of the femur, and the presence of any distal lesions or deformities.
Templating should be performed to estimate the appropriate nail diameter, nail length, and the neck-shaft angle. The contralateral intact proximal femur is typically used as a template to determine the patient's native neck-shaft angle, which typically ranges from 125 to 135 degrees. Restoring this angle is critical to optimizing the biomechanics of the hip abductors and equalizing leg length. The surgeon must also anticipate the need for a short versus long cephalomedullary nail. While short nails are generally sufficient for standard intertrochanteric fractures, long nails are indicated for subtrochanteric fractures, pathologic fractures, or when the fracture extends distally into the diaphysis.
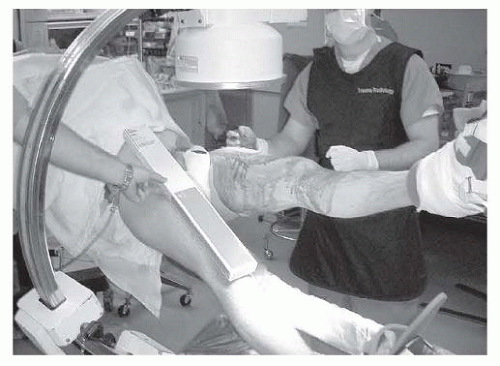
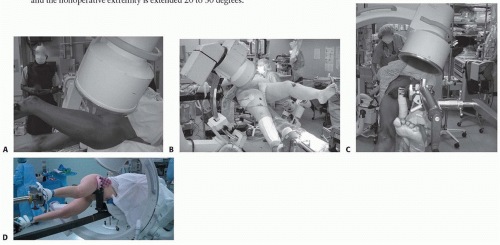
Patient positioning is a critical step that dictates the ease of reduction and fluoroscopic imaging. The procedure is most commonly performed with the patient supine on a fracture table. The bilateral lower extremities are secured in traction boots. The operative leg is placed in traction, adduction, and slight internal rotation to overcome the deforming forces and restore length and alignment. The contralateral leg is typically placed in a hemilithotomy position or extended downward (scissor position) to allow unobstructed access for the C-arm fluoroscopy unit to obtain true lateral views of the proximal femur.
Alternatively, some surgeons prefer positioning the patient supine on a flat radiolucent table. This technique requires manual traction or the use of a femoral distractor but avoids the complications associated with the perineal post of the fracture table, such as pudendal nerve palsy. Flat table positioning is particularly advantageous in polytrauma patients who have multiple extremity injuries or pelvic ring disruptions that contraindicate the use of a fracture table.
Regardless of the table utilized, the C-arm must be positioned to provide crisp, orthogonal views of the femoral head, neck, and shaft. The surgeon must verify that a perfect lateral view can be obtained before prepping and draping. A perfect lateral view is confirmed when the femoral head, neck, and greater trochanter are collinear, and the anterior and posterior cortices of the femoral shaft are distinct and parallel.
Detailed Surgical Approach and Technique
The surgical technique for cephalomedullary nailing requires strict adherence to biomechanical principles, beginning with an anatomic or near-anatomic closed reduction. The surgeon must never attempt to compensate for a poor reduction with implant placement. If closed reduction maneuvers (traction, internal rotation, and adduction) fail to restore the medial cortical buttress and correct varus or apex anterior angulation, percutaneous or formal open reduction techniques must be employed. Percutaneous techniques include the use of a ball-spike pusher, bone hooks, or strategically placed collinear reduction clamps.
Incision and Entry Point Selection
Once reduction is achieved and confirmed fluoroscopically, a 3 to 5 centimeter longitudinal incision is made proximal to the greater trochanter. The fascia lata is incised in line with the skin incision. The gluteus medius muscle fibers are split bluntly to access the proximal femur.
The selection of the entry point is arguably the most critical step of the operation. An improper entry point will dictate a malaligned trajectory for the nail, leading to varus malreduction, iatrogenic fracture of the medial or lateral cortex, or eccentric reaming.
There are two primary entry points utilized for cephalomedullary nailing: the piriformis fossa and the tip of the greater trochanter. The piriformis fossa entry point is collinear with the anatomic axis of the femoral medullary canal, allowing for the use of a straight nail. However, accessing the piriformis fossa is technically demanding, particularly in obese patients, and carries a higher risk of iatrogenic injury to the medial femoral circumflex artery.
Modern cephalomedullary nails are predominantly designed for a trochanteric entry point. These nails feature a proximal valgus bend (typically 4 to 6 degrees) to accommodate the lateral offset of the greater trochanter. The ideal starting point for a trochanteric entry nail is at the exact tip of the greater trochanter or slightly medial to the tip, at the junction of the anterior third and posterior two-thirds of the trochanter in the sagittal plane. A starting point that is too lateral will force the nail into varus, while a starting point that is too anterior may result in anterior cortical perforation during insertion.
Guide Wire Placement and Reaming
A rigid guide pin is advanced through the selected entry point under biplanar fluoroscopic guidance. Once the starting pin is confirmed to be centrally located within the medullary canal on both AP and lateral views, an opening reamer is utilized to breach the proximal cortex and prepare the proximal femur for the bulky proximal portion of the nail.
A ball-tipped guide wire is then passed down the medullary canal, crossing the fracture site and advancing to the level of the physeal scar in the distal femur. The surgeon must ensure the guide wire remains centrally located within the canal to avoid eccentric reaming. Sequential flexible reaming is performed over the ball-tipped guide wire. The canal is typically reamed to a diameter 1.0 to 1.5 millimeters larger than the selected nail diameter to prevent excessive hoop stresses during nail insertion, which could cause iatrogenic diaphyseal fractures.
Nail Insertion and Cephalic Fixation
The selected cephalomedullary nail is assembled to the targeting jig and advanced manually over the guide wire. The nail should be inserted with gentle twisting motions; excessive force or heavy mallet strikes must be avoided. The depth of insertion is determined by the intended placement of the cephalic screw within the femoral head.
Once the nail is appropriately seated, a guide pin for the cephalic screw or helical blade is inserted through the targeting jig. The placement of this guide pin is critical for the long-term success of the construct. The goal is to place the cephalic implant perfectly in the center of the femoral head on the AP view and perfectly in the center of the femoral head on the lateral view (the "center-center" position).
The concept of Tip-Apex Distance (TAD), originally described by Baumgaertner, is the most important predictor of cephalic screw cut-out. The TAD is the sum of the distance from the tip of the lag screw to the apex of the femoral head on the AP radiograph and the corresponding distance on the lateral radiograph, after correcting for radiographic magnification. A TAD of less than 25 millimeters is strongly associated with successful fixation, whereas a TAD exceeding 25 millimeters exponentially increases the risk of cut-out.
After the guide pin is placed optimally, the lateral cortex is opened, and the femoral head is reamed over the pin. The cephalic screw or blade is then inserted. The surgeon must decide whether to engage the locking mechanism to allow controlled dynamic sliding of the screw within the nail, which promotes secondary bone healing through fracture impaction.
Distal Interlocking
Following cephalic fixation, distal interlocking screws are placed to control rotation and maintain femoral length. For short nails, distal locking is typically performed through the targeting jig. For long nails, freehand fluoroscopic techniques (the "perfect circle" technique) are utilized. Depending on the fracture pattern, the distal screws can be placed in a static mode (preventing any shortening) or a dynamic mode (allowing controlled axial dynamization).
Complications and Management
Despite advances in implant design and surgical technique, cephalomedullary nailing of proximal femur fractures carries a distinct profile of postoperative complications. The surgeon must be vigilant in preoperative planning and execution to minimize these risks.
The most devastating mechanical complication is cut-out of the cephalic screw through the superior articular surface of the femoral head. Cut-out is almost exclusively a result of technical error, specifically varus malreduction, superior/anterior placement of the cephalic screw, or a Tip-Apex Distance greater than 25 millimeters. Once cut-out occurs, the joint is destroyed, and the patient typically requires salvage with a total hip arthroplasty or hemiarthroplasty.
In constructs utilizing dual cephalic screws, the "Z-effect" and "reverse Z-effect" are recognized phenomena. The Z-effect occurs when the inferior lag screw migrates laterally while the superior anti-rotation screw migrates medially through the femoral head. The reverse Z-effect is the opposite, with the inferior screw migrating medially and the superior screw backing out laterally. These complications are driven by differential load-bearing and toggling of the implants in osteoporotic bone.
| Complication | Incidence | Etiology and Risk Factors | Salvage Strategy |
|---|---|---|---|
| Cephalic Screw Cut-Out | 2% to 6% | TAD > 25mm, varus malreduction, superior screw placement, severe osteoporosis. | Conversion to Total Hip Arthroplasty or Hemiarthroplasty. |
| Peri-Implant Fracture | 1% to 3% | Eccentric reaming, excessive mallet force during insertion, anterior cortical impingement (radius of curvature mismatch). | Revision to a longer intramedullary nail bypassing the fracture, or open reduction with plate and cable constructs. |
| Nonunion / Delayed Union | 1% to 5% | Distraction at the fracture site, devascularization of fragments, inadequate mechanical stability. | Dynamization (removal of static locking screws), exchange nailing, bone grafting, or revision fixation. |
| Anterior Thigh Pain | 5% to 10% | Mismatch between the straight nail design and the native anterior bow of the femur, causing distal tip impingement on the anterior cortex. | Implant removal after solid radiographic union, or use of newer generation nails with anatomic radii of curvature. |
| Infection | 1% to 2% | Prolonged operative time, open fractures, severe medical comorbidities, hematoma formation. | Irrigation and debridement, suppressive antibiotics. If hardware is loose or fracture is unhealed, radical debridement and staged reconstruction. |
Another significant complication is iatrogenic fracture of the lateral wall or greater trochanter during reaming or nail insertion. This converts a stable fracture into an unstable pattern. To mitigate this, surgeons must ensure the entry point is precise and that the opening reamer is advanced fully to clear the lateral cortex.
Post Operative Rehabilitation Protocols
The primary goal of surgical stabilization is to allow immediate, safe mobilization of the patient to prevent the lethal complications of prolonged bed rest. In the vast majority of intertrochanteric fractures treated with a cephalomedullary nail, patients are permitted to bear weight as tolerated (WBAT) immediately postoperatively. The load-sharing biomechanics of the intramedullary device combined with a stable cephalic construct typically withstand the forces of early ambulation.
However, in cases of highly unstable subtrochanteric fractures, severe comminution with lack of medial cortical continuity, or extremely poor bone quality, the surgeon may elect to restrict weight-bearing (e.g., toe-touch weight-bearing or flat-foot weight-bearing) for 6 to 8 weeks until early radiographic callus is visible.
Deep vein thrombosis (DVT) prophylaxis is mandatory. Proximal femur fractures carry one of the highest risks for venous thromboembolism in orthopedic surgery. Chemical prophylaxis (such as low molecular weight heparin, direct oral anticoagulants, or adjusted-dose warfarin) should be initiated postoperatively and continued for a minimum of 28 to 35 days, in conjunction with mechanical sequential compression devices.
Furthermore, a proximal femur fracture in a geriatric patient is a sentinel event for severe osteoporosis. Postoperative protocols must include a comprehensive metabolic bone health evaluation. Initiation of anti-resorptive medications (bisphosphonates, RANKL inhibitors) or anabolic agents (teriparatide, abaloparatide), along with calcium and vitamin D supplementation, is critical to reducing the risk of a subsequent contralateral hip fracture or vertebral compression fracture.
Summary of Key Literature and Guidelines
The academic literature surrounding the treatment of proximal femur fractures is extensive and continually evolving. The American Academy of Orthopaedic Surgeons (AAOS) clinical practice guidelines strongly recommend the use of cephalomedullary nails for unstable intertrochanteric fractures and subtrochanteric fractures.
Historically, the debate between utilizing a sliding hip screw (extramedullary) versus a cephalomedullary nail (intramedullary) for stable intertrochanteric fractures heavily favored the sliding hip screw due to lower complication rates and reduced cost. However, modern iterations of cephalomedullary nails have minimized historical complications such as anterior thigh pain and iatrogenic femoral shaft fractures. Consequently, contemporary literature demonstrates equivalent outcomes between the two devices for stable patterns, with many surgeons defaulting to cephalomedullary nailing due to its minimally invasive insertion technique and superior biomechanical profile.
The concept of Tip-Apex Distance (TAD), introduced by Baumgaertner et al. in 1995, remains the most universally cited and validated metric in proximal femoral fracture surgery. The literature unequivocally supports that strict adherence to a TAD of less than 25 millimeters is the single most controllable intraoperative variable to prevent construct failure.
Recent literature has also heavily scrutinized the choice between short and long cephalomedullary nails for intertrochanteric fractures. Large registry data and randomized controlled trials indicate that for standard, extracapsular intertrochanteric fractures without subtrochanteric extension, short nails offer decreased operative time, reduced blood loss, and lower costs without an increased risk of peri-implant fractures compared to long nails. Long nails remain strictly indicated for subtrochanteric fractures, pathologic lesions, and cases where the distal fracture extension compromises the isthmus of the femur.
