Ankle Fracture Case: Expert Guide to This Complex Case
Patient Presentation & History
A 48-year-old male, a construction worker, presented to the emergency department following a fall from a height of approximately 10 feet. He landed directly on his left foot. He reported immediate, severe pain in his left ankle, inability to bear weight, and rapid swelling. He denied any head injury, loss of consciousness, or other significant trauma.
His past medical history included well-controlled Type 2 Diabetes Mellitus diagnosed 5 years prior, managed with oral hypoglycemics, and a 20-pack-year smoking history, currently smoking half a pack per day. He had no prior surgeries and no known allergies. His social history included living independently, active employment, and regular alcohol consumption (2-3 beers daily). His comorbidities, particularly diabetes and smoking, are critical considerations for wound healing, infection risk, and overall prognosis.
Clinical Examination
Upon arrival, the patient was alert and oriented. Vital signs were stable.
Inspection:
The left ankle was markedly swollen with significant ecchymosis extending from the midfoot to the distal leg. The skin was taut, exhibiting early blistering over the malleoli. There was no gross deformity, open wounds, or evidence of skin tenting, but the integrity of the soft tissue envelope was clearly compromised by the edema.
Palpation:
Diffuse tenderness was elicited circumferentially around the ankle joint, particularly over the lateral, medial, and posterior malleoli. Crepitus was appreciated with gentle manipulation. Palpation proximally revealed no tenderness over the fibular head or proximal tibia, ruling out a Maisonneuve fracture component or associated tibial shaft fracture. The foot was stable, with no tenderness over the midfoot or forefoot suggestive of concomitant injuries.
Range of Motion (ROM):
Due to severe pain and swelling, active and passive range of motion of the ankle was extremely limited and resisted. Dorsiflexion, plantarflexion, inversion, and eversion were all severely restricted.
Neurological Assessment:
Sensory examination revealed intact sensation to light touch in the distribution of the superficial peroneal, deep peroneal, sural, saphenous, and tibial nerves. Motor function was assessed indirectly due to pain but the patient was able to weakly wiggle his toes. No motor deficits were overtly identified.
Vascular Assessment:
Distal pulses (dorsalis pedis and posterior tibial arteries) were palpable and strong bilaterally, 2+ on a 0-4+ scale. Capillary refill in the toes was less than 2 seconds. The foot was warm and well-perfused. No compartment syndrome was suspected at this stage, but the tight skin envelope warranted close monitoring.
Imaging & Diagnostics
Initial radiographic evaluation included standard weight-bearing (when possible, but not in acute trauma), anteroposterior (AP), mortise, and lateral views of the left ankle.
X-ray Findings:
- AP View: Demonstrated widening of the medial clear space and an oblique fracture of the distal fibula.
- Mortise View: Confirmed the widening of the medial clear space (>4mm), suggesting deltoid ligament rupture or medial malleolar fracture. There was clear syndesmotic diastasis with overlap loss between the tibia and fibula. The fibular fracture was observed to be proximal to the syndesmosis.
- Lateral View: Revealed significant posterior subluxation of the talus, a large posterior malleolar fracture fragment involving approximately 30-35% of the articular surface, and distal displacement of the fibula relative to the tibia.
Based on these findings, specifically the high fibular fracture, syndesmotic disruption, medial clear space widening, and a large posterior malleolar fragment, a Lauge-Hansen classification of pronation-external rotation (PER) Stage IV was considered, or an AO/OTA 44-C3 variant. The presence of a significant posterior malleolus fragment (greater than 25-30% of the articular surface) confirmed the instability and the need for fixation of this fragment.
CT Imaging:
Given the complexity of the fracture pattern, particularly the posterior malleolar involvement, significant comminution of the fibula, and suspected syndesmotic injury, a CT scan of the ankle was ordered. This was crucial for:
1.
Precise assessment of posterior malleolar fragment:
Size, comminution, articular involvement, and extension into the tibial plafond.
2.
Evaluation of syndesmotic reduction:
Identifying subtle displacement or rotation not fully appreciated on plain radiographs.
3.
Assessment of plafond involvement:
Detecting occult impaction or chondral damage.
4.
Templating:
The CT scan allowed for detailed pre-operative planning, including the trajectory for posterior malleolar screw fixation, optimal plate contour for the fibula, and determination of syndesmotic screw length and position. It also allowed for assessing the quality of bone for implant purchase.
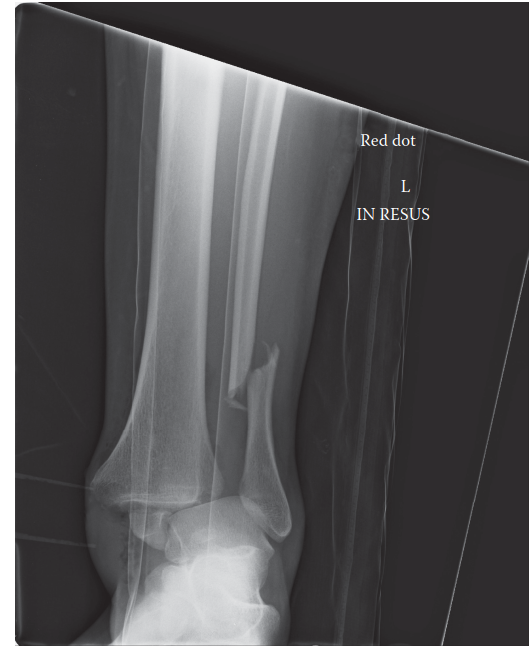
Figure: Axial CT image demonstrating significant comminution of the distal fibula, widening of the tibiofibular clear space, and a substantial posterior malleolar fragment with articular involvement, consistent with a complex ankle fracture dislocation. Note the displacement and rotation of the fibular shaft.
MRI Indications:
While not routinely indicated for acute ankle fractures prior to surgical fixation, MRI might be considered in specific circumstances such as:
* Suspected osteochondral lesions of the talus or plafond not clearly delineated on CT.
* Evaluation of chronic ligamentous instability after fracture healing, if symptomatic.
* Assessment of tendinous injuries (e.g., peroneal tendon subluxation/tear) if clinically indicated and not visible on other modalities.
* However, for this acute, unstable fracture requiring immediate fixation, MRI was deferred.
Templating:
Pre-operative templating using the CT images was performed. This involved selecting appropriate plate and screw sizes for the fibula (e.g., 1/3 tubular, locking plate), planning the number and trajectory of screws for the medial malleolus, and crucially, determining the optimal approach and fixation strategy for the posterior malleolus, considering whether an anteroposterior or posteroposterior approach would be necessary. Syndesmotic screw length was estimated based on bicortical fixation requirements and the width of the tibia and fibula at the appropriate level (typically 2-3 cm proximal to the ankle joint line).
Differential Diagnosis
While the imaging clearly confirmed a complex ankle fracture, a comprehensive approach requires considering other diagnoses, especially prior to definitive imaging or in cases with atypical presentations.
| Feature / Condition | Complex Ankle Fracture (e.g., PER IV / AO 44-C3) | High Ankle Sprain (Syndesmotic Injury) | Pilon Fracture (Distal Tibia) | Severe Ankle Sprain (Lateral Ligament) |
|---|---|---|---|---|
| Mechanism of Injury | Rotational (e.g., pronation-external rotation), often high energy, direct impact | Forced external rotation of foot on fixed tibia, dorsiflexion | Axial load with rotational component, high energy, fall from height | Inversion injury, plantarflexion with inversion, low to moderate energy |
| Pain Location | Diffuse ankle pain, specific malleolar tenderness, deep ankle pain | Anterolateral ankle, pain above syndesmosis on palpation (AITFL) | Diffuse, severe pain in distal tibia and ankle joint | Lateral ankle, pain over anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) |
| Swelling / Ecchymosis | Marked, diffuse, rapid onset | Variable, often localized anterolaterally, delayed onset | Severe, rapid, often extending proximally, blistering common | Variable, localized lateral, often delayed |
| Deformity | Often gross deformity, joint instability, subluxation | Typically no gross deformity | Gross deformity common, significant articular disruption | Rarely gross deformity, may have slight varus position |
| Weight-Bearing | Unable to bear weight (NWB) | Painful and difficult (PWB), sometimes NWB | Unable to bear weight (NWB) | Painful and difficult (PWB), sometimes NWB |
| Physical Exam Findings | Malleolar tenderness, crepitus, positive squeeze test (proximal fibula), external rotation stress test positive | Tenderness over AITFL, positive squeeze test, positive external rotation stress test (pain) | Extreme tenderness, crepitus, skin compromise, palpable step-off | Tenderness ATFL/CFL, anterior drawer/talar tilt positive (if severe) |
| X-ray Findings | Fibular fracture (often high), medial malleolus or wide medial clear space, posterior malleolus fx, syndesmotic diastasis | Normal or subtle widening of syndesmosis, often no fracture | Tibial plafond comminution, articular impaction, metaphysis fx, +/- fibular fx | Normal or small avulsion fx (e.g., lateral malleolus tip) |
| CT Scan Utility | Essential for detailed fracture morphology, articular involvement, syndesmosis | Useful for subtle syndesmotic avulsions or osteochondral lesions | Essential for 3D assessment of articular comminution and impaction | Rarely indicated, unless suspecting occult fracture or osteochondral injury |
| Treatment Implications | Surgical fixation almost always required (ORIF) | Often conservative (immobilization, rehab), but surgical fixation of syndesmosis if unstable | Surgical fixation (ORIF) - complex, high complication rate | Conservative (RICE, bracing, rehab), rarely surgical |
Surgical Decision Making & Classification
This patient’s fracture pattern – a Lauge-Hansen pronation-external rotation (PER) Stage IV with a large posterior malleolar fragment, clear syndesmotic diastasis, and medial clear space widening – unequivocally mandated operative fixation. Non-operative management for such an unstable, displaced ankle fracture would invariably lead to malunion, persistent instability, and rapid development of debilitating post-traumatic arthritis.
Indications for Operative Fixation:
- Displaced bimalleolar or trimalleolar fracture: Any displacement >2mm.
- Syndesmotic instability: Demonstrated by widening of the tibiofibular clear space, decreased tibiofibular overlap on mortise view, or positive external rotation stress test (if applicable).
- Large posterior malleolar fragment: Generally >25-30% of the articular surface, especially if displaced >2mm or leading to posterior talar subluxation. This fragment contributes significantly to joint stability and congruity.
- Irreducible fracture-dislocation: Even after closed reduction attempts.
- Open ankle fracture: (Not present in this case).
Classification Systems Guiding Decision Making:
-
Lauge-Hansen Classification: While controversial for its reproducibility, it helps understand the mechanism of injury and predict the sequence of ligamentous and osseous disruptions. In this case, the PER IV pattern (medial clear space widening or medial malleolus fracture, anterior inferior tibiofibular ligament disruption, fibula fracture proximal to syndesmosis, posterior inferior tibiofibular ligament disruption or posterior malleolus fracture) directly points to significant instability involving all three columns of the ankle. This informed the need for repair of all disrupted elements.
-
Danis-Weber / AO/OTA Classification:
- Weber B: Fibular fracture at the level of the syndesmosis.
- Weber C: Fibular fracture proximal to the syndesmosis. This patient's fibular fracture was proximal to the syndesmosis, classifying it as a Weber C fracture . Weber C fractures are inherently unstable and are almost always associated with syndesmotic disruption, necessitating syndesmotic fixation. The AO/OTA equivalent would be 44-C, signifying a complex fracture involving both malleoli and potentially the posterior malleolus and syndesmosis. This classification emphasizes the extent of osseous injury and indirectly, soft tissue involvement.
-
Herscovici Classification (for posterior malleolus): This system further characterizes posterior malleolar fractures, primarily by size and morphology. A fragment involving >25-30% of the articular surface significantly impacts ankle stability and contact pressures, mandating direct reduction and fixation. Our patient's fragment (30-35%) falls into this category.
Pre-operative Considerations:
- Soft Tissue Envelope: Given the significant swelling and early blistering, surgical timing was critical. The "wrinkle test" was performed daily. Surgery was deferred until the soft tissue swelling subsided sufficiently to allow safe surgical access and closure, typically 5-7 days post-injury. During this period, the ankle was immobilized in a splint, elevated, and ice packs applied.
- Comorbidities: Strict glycemic control was initiated for the patient's diabetes. His smoking cessation was strongly advised, given the increased risk of non-union, infection, and wound healing complications. Prophylactic antibiotics and DVT prophylaxis were initiated.
Surgical Technique / Intervention
The patient underwent Open Reduction Internal Fixation (ORIF) of the left ankle fracture 6 days after injury, once the soft tissue envelope had improved.
Anesthesia & Positioning:
General endotracheal anesthesia was administered. The patient was positioned supine on a radiolucent operating table, with a tourniquet applied to the proximal thigh. A bump was placed under the ipsilateral buttock to internally rotate the leg slightly, improving access to the lateral malleolus. The foot was draped free to allow full range of motion and intraoperative fluoroscopy in multiple planes (AP, mortise, lateral).
Surgical Approaches:
-
Posterolateral Approach for Posterior Malleolus: This approach was chosen given the large posterior malleolar fragment and its posterior subluxation. A curvilinear incision was made between the peroneal tendons and the Achilles tendon. The sural nerve was identified and protected. The interval between the peroneals (laterally) and the flexor hallucis longus (FHL) (medially) was developed. The posterior malleolar fragment was directly visualized, reduced anatomically using direct manipulation, and provisionally stabilized with K-wires. Fixation was achieved with two 3.5mm anterior-to-posterior lag screws, ensuring they were well subchondral and did not violate the articular surface. Fluoroscopy confirmed anatomical reduction and screw placement.
-
Lateral Approach for Fibula: A standard curvilinear incision centered over the distal fibula was made. Full-thickness flaps were raised to expose the fracture. The fracture was comminuted and spiraling. Indirect reduction was first attempted using ligamentotaxis and traction. Direct reduction using reduction clamps was then performed, restoring length, rotation, and alignment. Provisional fixation was achieved with K-wires. A 1/3 tubular plate was contoured and applied to the lateral aspect of the fibula, acting as a neutralization plate. Initial fixation involved a lag screw placed through the plate across the fibula fracture for interfragmentary compression. This was followed by bicortical screws proximal and distal to the fracture, ensuring adequate purchase in healthy bone.
-
Medial Approach for Medial Malleolus/Syndesmosis: A separate anteromedial incision was made. The deltoid ligament was found to be completely ruptured. The medial clear space was assessed. Once the fibula and posterior malleolus were provisionally stable, the ankle mortise was assessed for congruity. Any residual medial clear space widening would indicate inadequate syndesmotic reduction or persistent deltoid interposition, which was explored and cleared. The medial clear space was reduced indirectly by the fixation of the fibula and posterior malleolus.
-
Syndesmotic Fixation: After achieving anatomical reduction of the fibula and posterior malleolus, and ensuring mortise congruity under fluoroscopy, the stability of the syndesmosis was re-evaluated using a manual external rotation stress test and a cotton test. With the ankle positioned in neutral dorsiflexion, the syndesmosis was reduced directly using a reduction clamp compressing the fibula into the incisura fibularis of the tibia. A syndesmotic screw (4.5mm cortical, tricortical engagement for primary fixation) was then inserted 2-3 cm proximal to the ankle joint line, angled approximately 30 degrees posteriorly and 30 degrees anteriorly (depending on specific anatomy and surgeon preference) from the fibula into the tibia. Intraoperative fluoroscopy confirmed satisfactory reduction of the syndesmosis on AP, mortise, and lateral views. The use of a suture button device was considered as an alternative for dynamic syndesmotic fixation but was deferred in favor of traditional screw fixation given the surgeon's preference and the comminuted fibular fracture.
Wound Closure:
After thorough irrigation, hemostasis, and final fluoroscopic checks to confirm implant position and reduction quality, the incisions were closed in layers. A sterile dressing was applied, and a well-padded posterior splint was placed with the ankle in neutral dorsiflexion.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Day 0-14):
*
Immobilization:
Short leg posterior splint, non-weight-bearing (NWB) on the operative extremity.
*
Elevation:
Strict elevation of the limb above heart level to minimize swelling.
*
Pain Management:
Multimodal analgesia including opioids, NSAIDs (if no contraindications), and acetaminophen.
*
DVT Prophylaxis:
Low molecular weight heparin (LMWH) or aspirin per institutional protocol, continued for 4-6 weeks.
*
Wound Care:
Daily dressing changes as per protocol, monitor for signs of infection or wound dehiscence.
*
Diabetic Control:
Close monitoring and adjustment of blood glucose levels.
*
Smoking Cessation:
Continued strong encouragement for cessation.
Early Rehabilitation (Week 2-6):
*
Immobilization:
Transition to a removable controlled ankle motion (CAM) boot or short leg cast.
*
Weight-Bearing:
Continued NWB for 6 weeks, or until radiographic signs of early healing are evident (callus formation).
*
Range of Motion (ROM):
* Initiate gentle active and passive ankle dorsiflexion/plantarflexion, inversion/eversion
out of the boot/cast
at 2 weeks, focusing on pain-free motion.
* Strict avoidance of resisted external rotation to protect syndesmotic fixation.
*
Edema Control:
Compression stocking, continued elevation when resting.
Mid-Stage Rehabilitation (Week 6-12):
*
Weight-Bearing:
Gradually progress to partial weight-bearing (PWB) in the CAM boot, typically starting with 25% body weight at week 6, advancing by 25% each week as tolerated, based on pain and radiographic healing.
*
ROM:
Continue with active and passive ROM exercises.
*
Strengthening:
Introduce gentle isometric exercises for ankle musculature (e.g., dorsiflexors, plantarflexors, invertors, evertors) within pain limits.
*
Proprioception:
Begin non-weight-bearing balance exercises.
*
Syndesmotic Screw Removal:
The syndesmotic screw will be assessed at 12 weeks. If symptomatic or if significant hardware prominence is noted, removal may be considered, particularly if the fibular fracture is well-healed. Routine removal is debated, but often performed in active individuals to prevent breakage and allow physiological syndesmotic motion.
Late Rehabilitation (Week 12+):
*
Weight-Bearing:
Progress to full weight-bearing (FWB) out of the boot/cast as tolerated, once radiographic healing is confirmed and pain allows.
*
Strengthening:
Advance to progressive resistance exercises, focusing on functional strength.
*
Proprioception:
Advanced balance and agility drills.
*
Functional Training:
Begin sport-specific or work-specific activities.
*
Return to Activity:
Gradual return to light duty work or low-impact activities at 4-6 months, with full return to strenuous activity or sport typically at 6-12 months, depending on patient progress and fracture healing.
Monitoring for Complications:
Close follow-up is essential to monitor for post-operative complications such as infection, wound healing issues (especially with diabetes and smoking), malunion, non-union, hardware irritation, stiffness, complex regional pain syndrome (CRPS), and post-traumatic arthritis.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- Timing is Everything: Respect the soft tissue envelope. Delaying surgery for 5-10 days to allow swelling to subside (positive "wrinkle test") significantly reduces the risk of wound complications, infection, and skin necrosis.
-
Syndesmotic Reduction is Paramount:
The syndesmosis must be anatomically reduced. Malreduction by even 1-2mm can lead to significant pain and early post-traumatic arthritis.
- Intraoperative check: Direct visualization if possible, fluoroscopic images (AP, mortise, lateral), stress tests (hook test, external rotation stress test). Ensure the fibula is neither displaced laterally, medially, nor rotated.
- Positioning for fixation: Ankle in neutral dorsiflexion (NOT full dorsiflexion, which can over-compress the syndesmosis).
-
Posterior Malleolus: Don't Forget It:
If it's >25-30% of the articular surface, displaced, or causes talar subluxation, fix it. It restores stability and congruity.
- Approach: Consider posterolateral or posteromedial approaches for direct reduction. Anteroposterior lag screws are often effective.
- Restore Fibular Length, Rotation, and Alignment: The fibula dictates the mortise width. Accurate reduction of the fibula is key to anatomical reduction of the talus within the mortise.
- Multi-Planar Fluoroscopy: Always check reduction and hardware placement in AP, mortise, and lateral views. Don't rely solely on one view.
- Bone Quality: For osteoporotic patients, consider locking plates, cement augmentation, or increased number of screws to improve fixation strength.
- Comorbidity Management: Aggressive blood glucose control for diabetics, smoking cessation counseling for smokers are vital for healing and preventing complications.
- Post-Op Analgesia & DVT Prophylaxis: Essential for patient comfort and safety.
Pitfalls:
- Rushing Surgery: Operating through a swollen, blistered soft tissue envelope dramatically increases the risk of infection, wound dehiscence, and skin necrosis. This is a common exam pitfall – prioritize soft tissue healing.
- Inadequate Syndesmotic Reduction: The most common cause of poor outcomes after ankle fracture fixation. Often missed on single-plane fluoroscopy. Be vigilant with the external rotation stress test and tibiofibular overlap/clear space measurements.
- Ignoring the Posterior Malleolus: Leaving a large, displaced posterior malleolus unaddressed leads to posterior talar subluxation, joint incongruity, and post-traumatic arthritis.
- Malreduction of the Fibula: Failure to restore fibular length or rotation, or failure to reduce comminuted fragments, results in a widened mortise and poor outcomes.
-
Iatrogenic Injury:
- Sural Nerve Injury: Common with lateral/posterolateral approaches, requires careful dissection and retraction.
- Superficial Peroneal Nerve Injury: Risk with lateral approaches, especially with extensive subcutaneous dissection.
- Peroneal Tendon Impingement/Damage: During posterolateral approach or if hardware is prominent.
-
Hardware Placement Issues:
- Syndesmotic Screw Errors: Too many cortices (e.g., 4), inappropriate angle, placement too distal or too proximal. Over-tightening can cause iatrogenic diastasis of the distal fibula.
- Intra-articular Screws: Always ensure screws are subchondral and do not violate the joint space.
- Prominent Hardware: Can cause chronic irritation, necessitating removal.
- Early Weight-Bearing: Premature weight-bearing can lead to loss of reduction or implant failure, particularly before adequate fracture healing.
- Failure to Address Medial Side Pathology: Even if there's no medial malleolus fracture, a wide medial clear space signifies deltoid ligament rupture. While often addressed by fibular reduction, persistent instability or interposition may require direct repair.
This comprehensive approach, focusing on meticulous surgical technique, understanding the biomechanics, and diligent post-operative care, is essential for optimizing outcomes in complex ankle fracture management.
