Predictors of Hip Fracture Fixation Failure: Etiology, Biomechanics, & Prevention

Key Takeaway
Fixation failure in hip fractures is predicted by patient factors like osteoporosis, fracture biomechanics (e.g., high Pauwels angle, comminution), surgical technique (e.g., implant placement, load sharing), and vascular disruption. Understanding proximal femoral anatomy, bone quality, and fracture pattern stability is crucial for prevention and optimizing internal fixation outcomes.
An 82-year-old female presents following a mechanical fall. Radiographs reveal a displaced intertrochanteric hip fracture. What are the key radiographic parameters you must assess in the pre-operative plan to determine the optimal implant choice, and what do they signify?
Candidate: I would look at the lateral wall integrity and the degree of comminution, specifically the posteromedial calcar support. If the lateral wall is compromised or there is significant reverse obliquity, I would choose a cephalomedullary nail rather than a sliding hip screw to prevent lateral wall fracture and construct failure.
Candidates often fail to quantify the lateral wall thickness. Simply saying "it looks broken" is insufficient. Failing to mention the 'anterior bow' of the femur, which is critical when selecting a nail to avoid anterior cortical perforation, is a common oversight.
A structured response includes: 1) Lateral wall thickness: Less than 20.5mm is an indication for a cephalomedullary nail. 2) Calcar stability: Assessment of the posteromedial cortex integrity to predict varus collapse. 3) Fracture pattern: Identifying reverse obliquity patterns that mandate an intramedullary device due to shear forces. 4) Femoral anatomy: Measuring the anterior bow on the lateral radiograph to ensure the selected nail radius of curvature matches the patient's anatomy to prevent distal anterior cortical impingement.
You have performed an internal fixation for a hip fracture. Post-operatively, the patient is experiencing persistent pain. Looking at this radiograph, what is the most likely cause of the failure, and what is the specific technical metric you should have optimized to prevent it?
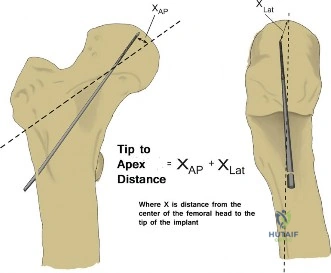
Candidate: The image shows hardware cutout through the superior femoral head. The most likely cause is a suboptimal Tip Apex Distance (TAD). I should have ensured the TAD was less than 25mm by placing the lag screw in a center-center position.
Stating only that the screw is in the "wrong place." Candidates must explicitly define the Tip Apex Distance (TAD) and note that it is the sum of the distances from the screw tip to the apex of the head on both AP and lateral views, corrected for magnification.
The patient has experienced implant cutout. The primary technical failure is a TAD > 25mm. The Gold Standard approach is to emphasize that TAD is the most critical surgeon-controlled variable. I would also mention that varus malreduction further exacerbates the shear forces, contributing to the cutout, and that salvage requires conversion to arthroplasty, noting the increased complexity due to hardware removal and proximal bone loss.
