DEFINITION
Carpal tunnel syndrome (CTS) is a compressive neuropathy of the median nerve at the wrist. CTS is the most common nerve compression condition in the upper extremity.Carpal tunnel release (CTR) is one of the most commonly performed procedures in the United States. Early stages of CTS are reversible with treatment.Later or more severe stages of CTS may not be (fully) reversible.
ANATOMY
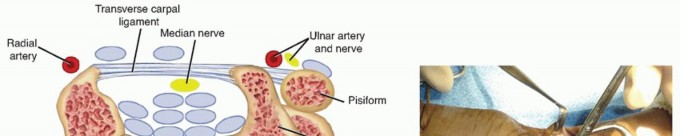
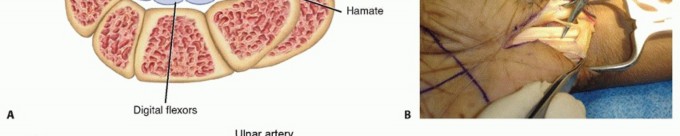
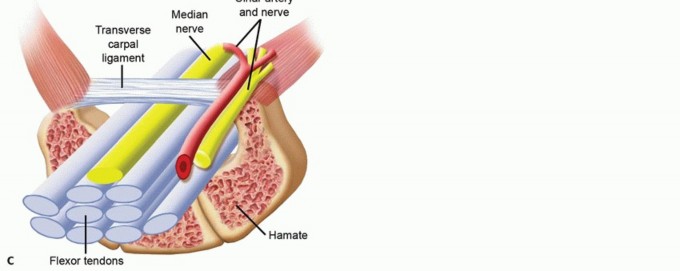
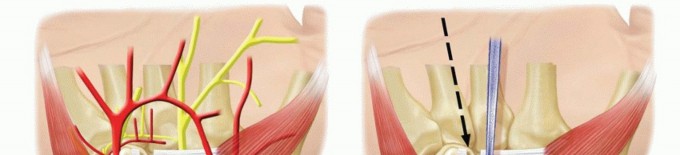
FIG 1 • A. Cross-section of the carpal tunnel. B. The carpal tunnel has been fully released, and the median nerve motor branch is seen branching from the nerve proximally and penetrating the radial portion of the TCL. C. Cross-section of the carpal tunnel with the ulnar artery and nerve superficial to the TCL.(continued)


FIG 1 •(continued)D. Traction on the median nerve secondary to significant displacement of a distal radius and ulna fracture. The nerve was displaced dorsal to the radius and ulna and remained dorsal following reduction. E. The nerve is shown after being removed from between the radius and ulna. (B: Copyright Thomas R. Hunt III, MD.)
PATHOGENESIS
Most cases of CTS are idiopathic.11Some cases are associated with systemic conditions, such as rheumatoid arthritis, diabetes, thyroid disease, chronic renal failure, and sarcoidosis.CTS is associated with pregnancy.There is an association of CTS with cumulative trauma and repetitive use.11 Increased pressure within the carpal canal is associated with CTS.2,7,14Peripheral neuropathy and CTS have also been associated with shear forces on the nerve, such as with atraction injury (FIG 1D,E).8
NATURAL HISTORY
CTS may have a variable course. It can improve, remain stable, or become more severe.Severity of compression, age, and patient comorbidities help predict natural history.Patients with severe CTS have motor and sensory changes and may have muscle weakness and atrophy.11Patients with extremely advanced CTS frequently have constant numbness, thenar weakness, and readily visible atrophy.
HISTORY AND PHYSICAL FINDINGS
Presenting symptoms can be variable: Some patients with mild CTS present with moderate to severe pain, numbness, and paresthesias, whereas other patients have minimal symptoms until their syndrome is severe.Symptoms are based in part on severity of disease.Mild diseaseIntermittent numbness and tinglingProvocative symptoms when driving, holding objects, and nocturnal waking Moderate diseaseNumbness and tingling become constant+/− provocative symptoms Severe diseaseDense constant numbnessFrequent absence of provocative symptomsThenar muscle atrophy with weakness and loss of dexterityObtain a full medical history to identify for risk factors for CTS such as hypothyroidism and diabetes.The surgeon must understand the patient's occupational and recreational hand activities and any antecedent trauma that might contribute to symptoms.It is helpful to inquire about activity(s) that trigger symptoms.Obtain a sense of symptom progression and severity.Questions should be asked about sensory and motor function, pain pattern, and nocturnal waking.The physical examination includes evaluation of the neck and shoulder girdle; the supraclavicular, infraclavicular, and axillary area; the humerus and elbow; the forearm; and the wrist and hand.It is important to generate a list of findings that may be responsible for the pain or paresthesiasotherthan CTS.In addition to the standard joint evaluation with range of motion and assessments of stability, it is important to palpate the course of the nerves and elicit the Tinel sign along the course of the paracervical, brachial plexus, median, ulnar, and radial nerves.The Tinel sign is mild, moderate, or severe based on subjective findings of radicular pain in an anatomic distribution. In a patient with peripheral neuropathy, the mechanical external stimulus threshold for nerve depolarization-repolarization is lowered.Phalen sign: Wrist flexion decreases the volume of the carpal canal and raises pressure in patients with CTS. The pattern of paresthesia is important.Carpal tunnel compression test: This is generally considered one of the most sensitive and specific tests for CTS.Two-point discrimination: In peripheral neuropathy, the ability to distinguish one or two points is often diminished.Decreased range of motion, crepitus, and palmar wrist swelling can be indirect indications of tenosynovium in the carpal canal or intra-articular wrist pathology.
IMAGING AND OTHER DIAGNOSTIC STUDIES
P.870Anteroposterior (AP), lateral, and oblique radiographs are not mandatory in the workup if the wrist examination is completely normal. If there is any possibility of wrist pathology, these studies should be obtained.Other imaging studies are generally not indicated in routine cases. However, in patients with recurrent CTS, magnetic resonance imaging (MRI) or ultrasound should be considered as a means to gain further information regarding a complete versus incomplete release of the TCL or evidence of median nerve compression,tenosynovitis, and scarring.1 Ultrasound has the advantage of providing a real time and dynamic analysis of the nerve and tendons in the carpal tunnel.10Electrodiagnostics: Nerve conduction studies (NCS) and electromyography (EMG) are important. CTS can be graded based on NCS and EMG findings:CTS mild: increased sensory or motor distal latency; may see decreased amplitude CTS moderate: increased nerve conduction velocityCTS severe: EMG shows signs of chronic denervation with positive fibrillations and sharp waves or unobtainable recordings from the electrodes to median innervated muscles.Although some experts believe the absence of any of the earlier electrodiagnostic findings means that there is no CTS, others believe that false-negatives exist due to sensitivity issues with NCS and EMG.5
DIFFERENTIAL DIAGNOSIS
Cervical radiculitisCervical pathology, joint disease, disc disease, facet disease with foramina stenosis Thoracic outlet syndromeBrachial plexopathySyringomyelia, motor neuron disease, myelopathy “Double crush syndrome”Shoulder pain related to instability, intra-articular pathology, subacromial impingement Acromioclavicular joint pathologyMedial epicondylitis Lateral epicondylitis Cubital tunnel syndrome Radial tunnel syndrome Pronator syndromeElbow pathology instability or contracture Forearm or wrist tenosynovitisWrist tenosynovitis, extensor, flexor, or de Quervain tenosynovitis Digital tenosynovitis (trigger finger)Guyon canal syndrome Hypothenar hammer syndrome Wrist or carpal fractureIntra-articular wrist pathology
NONOPERATIVE MANAGEMENT
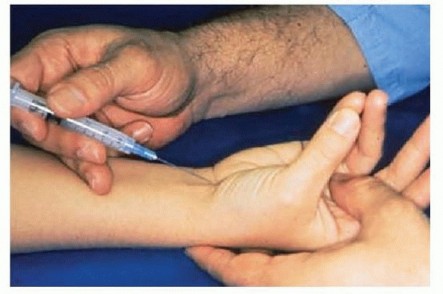
FIG 2 • CORTISONE INJECTION.
Wrist splints can be introduced.The physician can recommend or prescribe nonsteroidal anti-inflammatory drugs (NSAIDs). Corticosteroid injection into the carpal canal can be considered (FIG 2).Temporary relief from such an injection indicates that surgical decompression is likely to be successful.Hand therapy can be considered.Evidence suggests oral vitamin B12 or B6 treatments can be helpful.17,18
SURGICAL MANAGEMENT
The diagnosis of CTS is confirmed by either the presence of classic clinical symptoms and clinical signs or positive NCS or EMG studies.If the NCS or EMG findings are negative, at least one trial of corticosteroid injection should be considered to evaluate the clinical response. In addition to having a potential therapeutic benefit, it likely has prognostic value for surgery.It is important to confirm that a trial of conservative treatment has been undertaken without significant improvement or cure.The surgeon should confirm that differential diagnoses have been considered.Understanding that the presence of other diagnoses and conditions may affect the overall results of CTS treatment is critical; this needs to be discussed with the patient before, not after, surgery. In fact, one should strongly consider delaying CTS treatment to control or improve other conditions that may be amenable to nonoperative treatment.If the earlier conditions are met, CTR will likely provide good to excellent results in more than 90% of cases.19In the case of recurrent CTS, a key to success is patient selection. Although there are scant data to correlate the preoperative evaluation with results, the patient's clinical course, response to conservative treatment, and interpretation of electrodiagnostic studies and MRI or ultrasound should be carefully considered before revision surgery.
POSITIONING
CTR surgery is performed with the arm outstretched on a hand table.Pneumatic tourniquet use facilitates accurate identification of critical anatomic structures. Loupe magnification is recommended.Anesthesia can be by general anesthesia or regional anesthesia such as an axillary block or Bier block.P.871Experienced surgeons can perform CTS safely under wrist block or local infiltration with or without a light anesthetic.
APPROACH
TECHNIQUES
Open Carpal Tunnel Release
OPEN CARPAL TUNNEL RELEASE
EXPOSURE
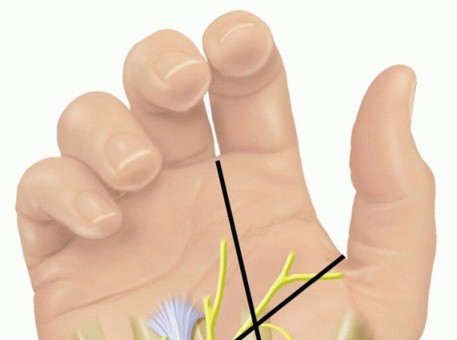
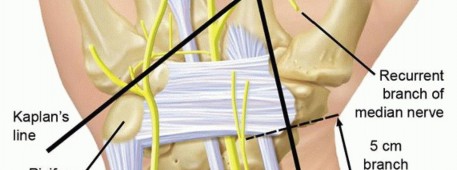
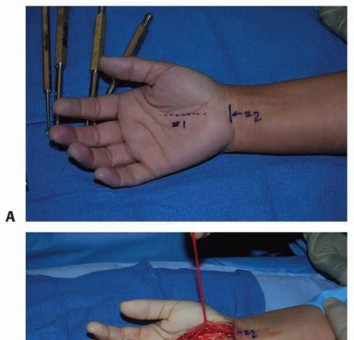
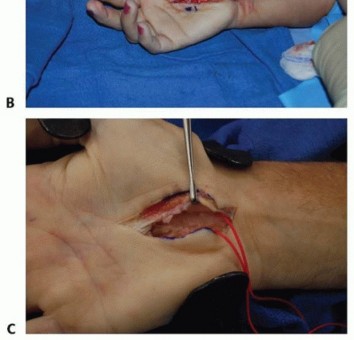
Mark the skin incision location, beginning at the intersection of the Kaplan cardinal line and a line drawn along the radial border of the fourth ray and ending at the wrist flexion crease (TECH FIG 1A).Use of a longitudinal hypothenar crease if available will likely yield a less obvious scar.The incision may be placed anywhere along this mark (TECH FIG 1B), depending on the surgeon's preference. I prefer the midpoint of the proximal third of the palm.The incision should be long enough to allow full access to the proximal and distal extents of the TCL in order to ensure full TCL division. This generally can be achieved without having the incision extendproximal to the wrist flexion crease.Dissect in line with the incision using a scalpel or scissors, through the subcutaneous fat and the palmar fascia down to the TCL (TECH FIG 1C).Frequently, the palmaris brevis muscle is encountered directly superficial to the TCL. It is incised and “feathered” from the ligament for adequate visualization of the TCL.Incise the TCL over a small segment, avoiding injury to deep structures (TECH FIG 1D).Contents of the carpal canal will have a characteristic appearance due to the tenosynovium.Place an instrument such as a mosquito clamp, Saint James, or Carroll elevator into the carpal canal, just deep to the TCL (TECH FIG 1E).This defines the undersurface of the TCL, the location of the hamate hook, and the proposed direction for release.Visualize the superficial surface of the TCL along its course and place a right angle retractor to protect the critical structures located between the skin and the ligament (TECH FIG 1F,G).
TRANSVERSE CARPAL LIGAMENT RELEASE


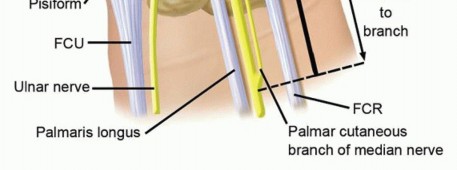
TECH FIG 1 • A. A longitudinal incision is marked for an open CTR. B. Either all or a limited portion of this incision may be used, depending on the surgeon's preference. C. The palmar fascia has been incised, the deep fat retracted ulnarly, and the palmaris brevis muscle fibers dissected, revealing the transverse fibers of the TCL. D. The distal portion of the TCL is carefully incised with a no. 15 knife blade. E. A mosquito clamp is placed deep to E the TCL in a distal to proximal direction.(continued)
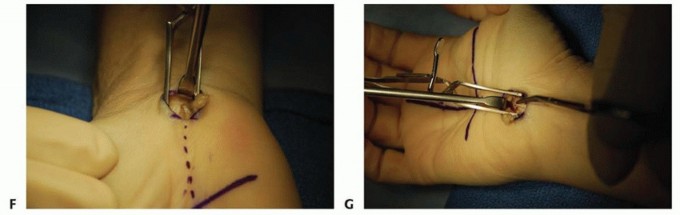
TECH FIG 1 •(continued)F. A right angle retractor is used to visualize the proximal TCL and the distal forearm fascia. G. The same retractor is then used to visualize the distal TCL to allow complete release. (B-G: Copyright Thomas R. Hunt, III, MD.)
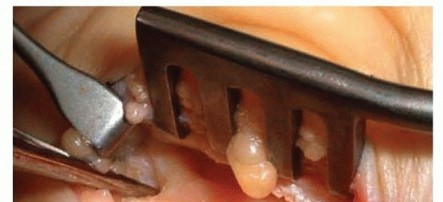

TECH FIG 2 • Open CTR with divided leaflets of the TCL retracted by the retractor jaws. The instrument is on the median nerve which is adherent to the undersurface of the TCL via tenosynovium. In primary CTR procedures without systemic disease, there is no role for internal neurolysis or tenosynovectomy (TECH FIG 2).4,9,12The wound is closed and sterile dressings are applied. My preference is interrupted 4-0 Prolene or nylon sutures.Use of a splint is based on the surgeon's preference.1. Single-Incision Endoscopic Carpal Tunnel Release (Modified Agee Technique)
EXPOSURE


DEVICE INSERTION


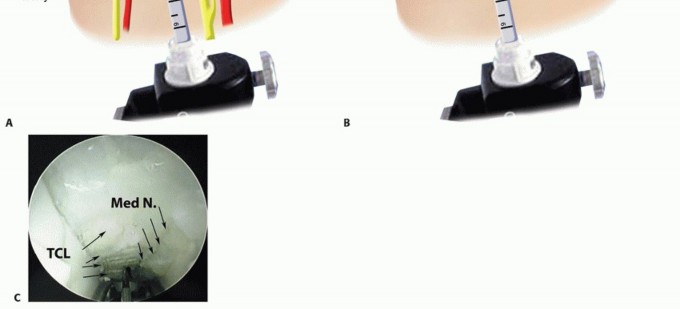
TECH FIG 4 • The surgeon's nondominant index and long digits palpate the tip of the ECTR device as it emerges into the subcutaneous space just distal to the transverse carpal tunnel ligament. The transillumination pattern from the device light source changes from underneath the TCL to the midpalmar fat.
TRANSVERSE CARPAL LIGAMENT RELEASE

HYPOTHENAR FAT PAD
When revision CTR reveals median nerve scarring, surgical tactics to improve the environment aroundthe nerve after the neurolysis to reduce rescarring are attractive. Strickland et al15 has described this technique in several publications. The tissue is readily available and has been shown to be of benefit. Ina 1996 article,15 62 patients were reviewed. Results were good based on pre- and postoperative patient satisfaction scores, with only three transient minor complications.Dissect the fat pad to the level of the ulnar nerve and artery, and advance the radial edge to cover the median nerve.Sew this edge to the radial flap of the TCL.
PALMARIS BREVIS FLAP
TECH FIG 6 • A,B. Revision of prior ECTR with open technique. C. Revision CTR with NeuraGen tube around scarred branch of median nerve. Poorpatient selection1. Perform a full history and physical examination and contemplate the entire list ofdifferential diagnoses.Incomplete ▪ Whatever technique is used, make sure it is performed in a technically proficientrelease of manner. Confirm complete TCL division, especially distally. TCLDamageto median nerve1. The surgeon must be able to identify the various anatomic structures anddistinguish them. The median nerve must be protected during CTR. In techniques where the median nerve is visualized, inspection should be performed after TCL release and before skin closure.
PEARLS AND PITFALLS
POSTOPERATIVE CARE
P.877Traditionally, CTR patients were managed in wrist splints for 1 to 3 weeks after surgery. However, multiple studies have shown that faster recovery occurs when the wrist is not splinted postoperatively.Temporary postoperative splints may still be indicated in specific clinical scenarios, such as open revision surgery.Hand therapy is helpful in the postoperative period, especially if the patient is having difficulty with full digital active and passive motion.Grip and pinch strengths, subjective symptom measures, and functional evaluations are helpful to manage the postoperative course.Some patients have prolonged periods of tenderness under the TCL, or pillar pain on the thenar or hypothenar side of the proximal palm, and require extended hand therapy and periods of time to gradually increase hand strength and endurance for hand activities.
OUTCOMES
There should be greater than 95% good or excellent results.19 This randomized, double-blinded multicenter study compared open and single portal ECTR and showed statistically significant improvements in the endoscopic group between 6 weeks and 3 months postoperatively in terms of pain and hand strength compared to that of the open group and equivalent good results in both groups at 1 year.Stütz et al16 reported on a retrospective series of 200 patients who underwent a secondary exploration during a 26-month period at a single institution for persistent or recurrent CTS symptoms after CTR. There were 108 cases of incomplete release of the TCL. Twelve patients had evidence of median nerve laceration during the index procedure. Forty-six patients had scarring of the nerve to surrounding tissues.In 13 patients, the cause of their problem could not be determined.Varitimidis et al20 reviewed 22 patients (24 wrists) who underwent revision open CTR after an initial ECTR and who had persistent CTS. Twenty-two patients had incomplete TCL release. One patient had a partial and another a complete median nerve transection. One patient had a Guyon canal release instead of a CTR. Twenty patients returned to work, 15 at the previous level and 5 at lighter duty. The 2 patients with nerve injuries continued to do poorly, 1 patient requiring a vein-wrapping procedure.
COMPLICATIONS
Incomplete TCL releaseMedian nerve scarring or damage (especially the common digital nerve to the third web space and the thenar motor branch)Ulnar nerve or artery damage Sympathetically mediated pain syndrome Damage to palmar arterial archFlexor tendon prolapse
REFERENCES
- Ablove RH, Peimer CA, Diao E, et al. Morphologic changes following endoscopic and two-portal subcutaneous carpal tunnel release. J Hand Surg Am 1994;19(5):821-826.
- Diao E, Shao F, Liebenberg E, et al. Carpal tunnel pressure alters median nerve function in a dose-dependent manner: a rabbit model for carpal tunnel syndrome. J Orthop Res 2005;23:218-223.
- Florack TM, Miller RJ, Pellegrini VD, et al. The prevalence of carpal tunnel syndrome in patients with basal joint arthritis of the thumb. J Hand Surg Am 1992;17(4):624-630.
- Gelberman RH, Pfeffer GB, Galbraith RT, et al. Results of treatment of severe carpal-tunnel syndrome without internal neurolysis of the median nerve. J Bone Joint Surg Am 1987;69(6):896-903.
- Grundberg AB. Carpal tunnel decompression in spite of normal electromyography. J Hand Surg Am 1983;8(3):348-349.
- Kaplan SJ, Glickel SZ, Eaton RG. Predictive factors in the non-surgical treatment of carpal tunnel syndrome. J Hand Surg Am 1990;15: 106-108.
- Lundborg G, Gelberman RH, Minteer-Convery M, et al. Median nerve compression in the carpal tunnel— functional response to experimentally induced controlled pressure. J Hand Surg Am 1982;7(3):252-259.
- Lundborg G, Rydevik B. Effects of stretching the tibial nerve of the rabbit. A preliminary study of the intraneural circulation and the barrier function of the perineurium. J Bone Joint Surg Br 1973;55(2): 390-401.
- Mackinnon SE, McCabe S, Murray JF, et al. Internal neurolysis fails to improve the results of primary carpal tunnel decompression. J Hand Surg Am 1991;16(2):211-218.
- Pinilla I, Martín-Hervás C, Sordo G, et al. The usefulness of ultrasound in the diagnosis of carpal tunnel syndrome. J Hand Surg Eur Vol 2008;33:435-439.
- Rempel DM, Diao E. Entrapment neuropathies: pathophysiology and pathogenesis. J Electromyogr Kinesiol 2004;14:71-75.
- Rhoades CE, Mowery CA, Gelberman RH. Results of internal neurolysis of the median nerve for severe carpal tunnel syndrome. J Bone Joint Surg Am 1985;67(2):253-256.
- Rose EH, Norris MS, Kowalski TA, et al. Palmaris brevis turnover flap as an adjunct to internal neurolysis of the chronically scarred median nerve in recurrent carpal tunnel syndrome. J Hand Surg Am 1991;16:191-201.
- Rydevik B, Lundborg G, Bagge U. Effects of graded compression on intraneural blood flow. An in vivo study on rabbit tibial nerve. J Hand Surg Am 1981;6(1):3-12.
- Strickland JW, Idler RS, Lourie GM, et al. The hypothenar fat pad flap for management of recalcitrant carpal tunnel syndrome. J Hand Surg Am 1996;21(5):840-848.
- Stütz N, Gohritz A, van Schoonhoven J, et al. Revision surgery after carpal tunnel release—analysis of the pathology in 200 cases during a 2-year period. J Hand Surg Br 2006;31(1):68-71.
- Talebi M, Andalib S, Bakhti S, et al. Effect of vitamin b6 on clinical symptoms and electrodiagnostic results of patients with carpal tunnel syndrome. Adv Pharm Bull 2013;3:283-288.
- Tanaka H. Old or new medicine? Vitamin B12 and peripheral nerve neuropathy [in Japanese]. Brain Nerve 2013;65:1077-1082.
- Trumble TE, Diao E, Abrams RA, et al. Single-portal endoscopic carpal tunnel release compared with open release: a prospective, randomized trial. J Bone Joint Surg Am 2002;84-A(7):1107-1115.
- Varitimidis SE, Herndon JH, Sotereanos DG. Failed endoscopic carpal tunnel release. Operative findings and results of open revision surgery. J Hand Surg Br 1999;24(4):465-467.
- Weiss AP, Sachar K, Gendreau M. Conservative management of carpal tunnel syndrome: a reexamination of steroid injection and splinting. J Hand Surg Am 1994;19(3):410-415.
