Brachial Plexus Injuries: Comprehensive Surgical Anatomy and Management
Key Takeaway
The brachial plexus is a complex neural network essential for upper extremity motor and sensory function. Managing its injuries requires profound anatomical knowledge to differentiate between preganglionic root avulsions and postganglionic ruptures. This comprehensive guide details the surgical anatomy, advanced diagnostic modalities including CT myelography, and step-by-step operative approaches. It provides orthopaedic surgeons with evidence-based strategies for nerve grafting, neurotization, and postoperative rehabilitation to optimize functional recovery.
INTRODUCTION TO THE BRACHIAL PLEXUS
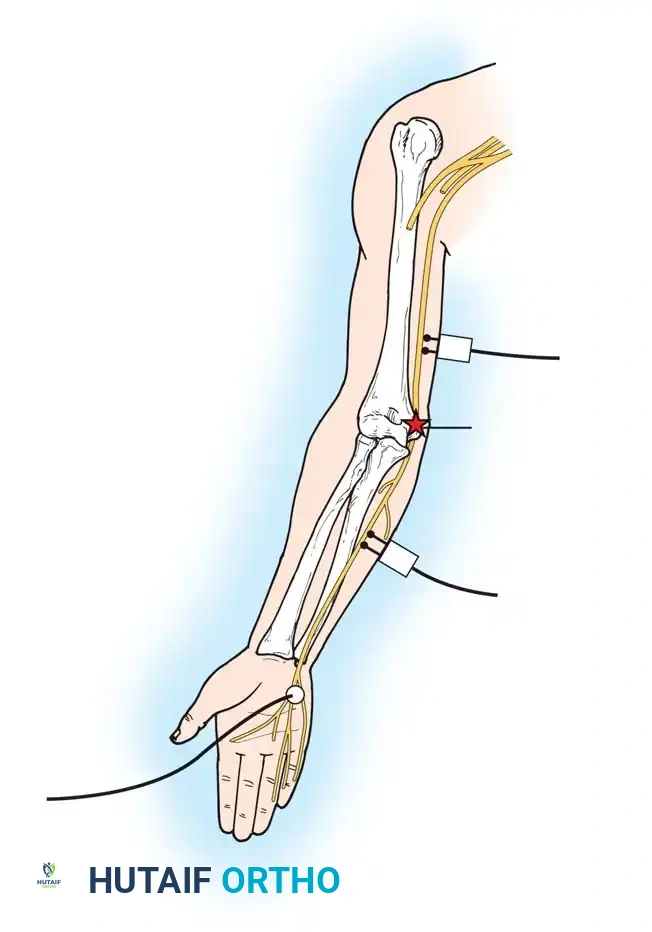
The management of brachial plexus injuries represents one of the most formidable challenges in operative orthopaedics and peripheral nerve surgery. A profound, three-dimensional understanding of the brachial plexus is mandatory for the orthopaedic surgeon, not only to accurately diagnose the level and severity of the injury but also to execute complex reconstructive procedures such as neurolysis, nerve grafting, and neurotization (nerve transfers).
Lesions of the brachial plexus can result in devastating functional impairment of the upper extremity. The clinical presentation is dictated entirely by the specific pathoanatomy of the injury—specifically, whether the lesion is preganglionic (root avulsion from the spinal cord) or postganglionic (rupture distal to the dorsal root ganglion). This distinction is the cornerstone of surgical decision-making, as preganglionic injuries are irreparable by direct grafting and necessitate nerve transfer techniques.
SURGICAL ANATOMY AND BIOMECHANICS
Formation of the Roots and Trunks
The brachial plexus is formed by the union of the anterior rami of the lower four cervical nerves (C5, C6, C7, C8) and the first thoracic nerve (T1). Anatomical variations are common: a "prefixed" plexus receives significant contribution from C4, while a "postfixed" plexus receives substantial fibers from T2.
Shortly after exiting the intervertebral foramen, each nerve root receives its sympathetic component via a gray ramus communicans. The cervical roots receive their sympathetic components from the lower cervical sympathetic ganglia. Crucially, the T1 root receives its sympathetic contribution from its own ganglion only after contributing a white ramus communicans to it.
Clinical Pearl: Injury to the T1 root proximal to the white ramus communicans disrupts the sympathetic pathway to the head and neck, resulting in ipsilateral Horner’s syndrome (ptosis, miosis, anhidrosis, and enophthalmos). The presence of Horner's syndrome is a pathognomonic clinical sign of a T1 preganglionic root avulsion.
The formation of the plexus begins just distal to the scalene muscles within the interscalene triangle (bordered by the anterior scalene, middle scalene, and first rib).
* Upper Trunk: Formed by the union of the C5 and C6 roots.
* Middle Trunk: Formed by the continuation of the C7 root alone.
* Lower Trunk: Formed by the union of the C8 and T1 roots.
Divisions, Cords, and Terminal Branches
As the trunks pass posterior to the clavicle, each divides into an anterior and a posterior division, reflecting the evolutionary separation of flexor and extensor muscle group innervation. These divisions unite to form three cords, named according to their anatomical relationship to the axillary artery:
- Lateral Cord: Formed by the anterior divisions of the upper and middle trunks (C5, C6, C7). It gives rise to the lateral pectoral nerve, which innervates the clavicular head of the pectoralis major. The lateral cord then terminates by dividing into the musculocutaneous nerve and the lateral contribution to the median nerve.
- Medial Cord: Formed by the anterior division of the lower trunk (C8, T1). It gives rise to the medial pectoral nerve (which forms an anastomotic loop with the lateral pectoral nerve to innervate both the pectoralis minor and the sternocostal head of the pectoralis major), the medial brachial cutaneous nerve, and the medial antebrachial cutaneous nerve. It terminates as the ulnar nerve and the medial contribution to the median nerve.
- Posterior Cord: Formed by the posterior divisions of all three trunks (C5-T1). It gives rise to the upper and lower subscapular nerves (innervating the subscapularis and teres major) and the thoracodorsal nerve (innervating the latissimus dorsi). It terminates by dividing into the axillary nerve (innervating the deltoid, teres minor, and overlying skin) and the radial nerve, which continues distally to supply the extensor compartments of the arm and forearm.
CLINICAL EVALUATION AND PATHOANATOMY
Upper Plexus Injury (Erb-Duchenne Palsy)
An injury to the upper trunk (C5, C6, and sometimes C7) typically results from a forceful downward traction on the shoulder combined with lateral flexion of the neck away from the affected side.
The biomechanical consequence of this specific denervation is the classic "waiter's tip" posture. The limb is typically extended at the elbow, flaccid at the side of the trunk, adducted, and internally rotated.
* Abduction and External Rotation Loss: Abduction is impossible due to paralysis of the deltoid and supraspinatus muscles. External rotation is absent due to paralysis of the infraspinatus and teres minor muscles.
* Elbow Flexion and Supination Loss: Active flexion of the elbow is impossible because of paralysis of the biceps brachii, brachialis, and brachioradialis muscles. Paralysis of the supinator muscle, unopposed by the intact pronators (innervated by lower roots), causes a fixed pronation deformity of the forearm.
* Sensory Deficits: Sensation is absent or severely diminished over the deltoid muscle and the lateral aspect of the forearm and hand (C5 and C6 dermatomes).
Differentiating Preganglionic Avulsions from Postganglionic Ruptures
Identifying an injury in which the roots of the plexus are avulsed from the spinal cord (preganglionic) is critical because direct surgical repair or grafting of an avulsed root is impossible.
Surgical Warning: A preganglionic avulsion must be recognized early. Attempting to graft an avulsed root will result in inevitable failure, as the motor neuron cell bodies located in the anterior horn of the spinal cord have been disconnected from the peripheral nerve.
Avulsions can be diagnosed clinically by identifying segmental motor and sensory deficits involving specific roots alongside paralysis of proximally innervated muscles. For example, paralysis of the serratus anterior (long thoracic nerve, C5-C7), the levator scapulae, and the rhomboids (dorsal scapular nerve, C5) indicates that the lesion is medial to the emergence of these nerves—confirming a root avulsion. Furthermore, long tract signs (e.g., hyperreflexia, spasticity in the lower extremities) may be present if the spinal cord itself was damaged during the avulsion.
ADVANCED DIAGNOSTIC MODALITIES
Electrodiagnostic Studies (EMG/NCS)
Electromyography (EMG) and Nerve Conduction Studies (NCS) are indispensable. The diagnosis of a root avulsion is often confirmed by demonstrating denervation potentials (fibrillations and positive sharp waves) in the segmental paraspinous musculature. Because these muscles are innervated by the posterior primary rami—which branch off just distal to the spinal nerve emergence—denervation here confirms a lesion at or proximal to the intervertebral foramen. Electrodiagnostic studies should be delayed for 3 to 4 weeks post-injury to allow for Wallerian degeneration to occur, preventing false-negative results.
Neuroimaging: CT Myelography and MRI
Historically, standard myelography was utilized to identify pseudomeningoceles (extravasation of cerebrospinal fluid through dural tears) or the complete absence of root shadows at the level of the avulsion.
Today, Computed Tomography (CT) myelography with enhancement is the gold standard, greatly improving diagnostic accuracy (demonstrating a 75% to 85% correlation with intraoperative findings).
Pitfall: CT myelography has a tendency to overestimate root avulsion and dye extravasation if used too early after the injury. Clotted blood may occlude the opening into a pseudomeningocele, leading to false negatives, or early dural tears without true root avulsion may lead to false positives. A delay of 6 to 12 weeks is strictly recommended before a CT myelogram is performed.
Magnetic Resonance Neurography (MRN) is increasingly utilized as a non-invasive adjunct. High-resolution 3T MRI can visualize neuroma formation, root continuity, and secondary signs of denervation in the target musculature (e.g., muscle edema in the acute phase, fatty infiltration in the chronic phase).
SURGICAL INDICATIONS AND TIMING
The timing of surgical intervention is dictated by the mechanism of injury:
1. Open Injuries (Sharp Transection): Immediate surgical exploration and primary end-to-end repair (or acute grafting) within 72 hours is indicated.
2. Closed Traction Injuries: A period of clinical and electrodiagnostic observation is warranted. If there is no evidence of spontaneous recovery (clinical or EMG) by 3 to 6 months, surgical exploration is indicated. Delaying surgery beyond 6 to 9 months significantly degrades the potential for motor endplate reinnervation, leading to irreversible muscle atrophy.
OPERATIVE APPROACHES AND SURGICAL TECHNIQUES
Positioning and Preparation
The patient is positioned supine with a bump under the ipsilateral scapula. The head is turned to the contralateral side, and the neck is slightly extended. The entire upper extremity, hemithorax, neck, and both lower extremities (for potential sural nerve graft harvest) are prepped and draped free. No paralytic agents should be used by anesthesia, as intraoperative nerve stimulation is critical.
The Supraclavicular Approach
This approach provides access to the roots, trunks, and the origin of the divisions.
1. Incision: A zigzag or L-shaped incision is made starting from the posterior border of the sternocleidomastoid (SCM) muscle, extending inferiorly to the clavicle, and continuing laterally along the superior border of the clavicle.
2. Superficial Dissection: The platysma is divided. The external jugular vein is identified and either retracted or ligated. The supraclavicular nerves are preserved if possible.
3. Deep Dissection: The omohyoid muscle is identified and divided. The transverse cervical and suprascapular vessels are ligated if they impede access.
4. Identifying the Phrenic Nerve: The anterior scalene muscle is exposed. The phrenic nerve must be identified coursing from lateral to medial across the anterior surface of the anterior scalene. It is carefully mobilized and protected.
5. Plexus Exposure: The anterior scalene is divided (sparing the phrenic nerve) to expose the underlying roots (C5, C6, C7) and the upper and middle trunks. The C8 and T1 roots are located deeper and inferiorly, often requiring careful retraction of the subclavian artery.
The Infraclavicular Approach
This approach is utilized for access to the divisions, cords, and terminal branches.
1. Incision: The incision extends from the coracoid process distally along the deltopectoral groove.
2. Dissection: The cephalic vein is identified and retracted (usually laterally with the deltoid). The deltopectoral interval is developed.
3. Deep Exposure: The pectoralis minor tendon is identified at its insertion on the coracoid process. For extensive exposure, the pectoralis minor is tenotomized or a coracoid osteotomy is performed.
4. Cord Identification: The clavipectoral fascia is incised. The axillary artery is the central landmark. The lateral cord is found lateral to the artery, the medial cord medial to it, and the posterior cord directly posterior to the artery.
Reconstruction Strategies: Grafting vs. Neurotization
Nerve Grafting:
If a postganglionic rupture is identified, the neuroma is resected back to healthy fascicles (confirmed by "mushrooming" of the axoplasm and frozen section if necessary). Sural nerve cable grafts are interposed between the proximal and distal stumps using 8-0 or 9-0 epineurial nylon sutures and fibrin glue.
Nerve Transfers (Neurotization):
For preganglionic avulsions, extra-plexus or intra-plexus nerve transfers are required to bypass the avulsed roots. The goal is to restore function in a prioritized order: (1) Elbow flexion, (2) Shoulder abduction/external rotation, (3) Hand sensation, (4) Wrist/finger flexion.
- Restoring Elbow Flexion (The Oberlin Transfer): In cases of upper trunk avulsion (C5/C6) with an intact lower trunk (C8/T1), redundant fascicles from the intact ulnar nerve (usually those supplying the flexor carpi ulnaris) are transferred directly to the motor branch of the biceps (musculocutaneous nerve). A double fascicular transfer (adding median nerve fascicles to the brachialis branch) provides even more robust elbow flexion.
- Restoring Shoulder Function: The spinal accessory nerve (CN XI) is frequently transferred to the suprascapular nerve to restore shoulder abduction and external rotation. The nerve to the long head of the triceps can also be transferred to the axillary nerve to reinnervate the deltoid.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Meticulous postoperative care is essential to protect the delicate neurorrhaphies and optimize functional outcomes.
- Immobilization: The patient is placed in a sling and swathe or a custom orthosis for 3 to 4 weeks to prevent any tension on the nerve repairs or grafts.
- Early Rehabilitation (Weeks 4-12): Passive range of motion (ROM) exercises are initiated to prevent joint contractures. Joint suppleness must be maintained, as a reinnervated muscle cannot move a stiff joint.
- Late Rehabilitation and Cortical Re-education: Nerve regeneration occurs at a rate of approximately 1 mm per day. Advancing Tinel's sign is monitored clinically. Once early motor reinnervation is detected (often 6 to 12 months postoperatively), active-assisted ROM and biofeedback are initiated. For nerve transfers (e.g., Oberlin transfer), cortical re-education is critical; the patient must initially think about flexing their wrist (ulnar nerve function) to activate their biceps, until neuroplasticity allows for spontaneous elbow flexion.
The management of brachial plexus injuries is a marathon, not a sprint. It requires precise anatomical knowledge, flawless microsurgical technique, and dedicated, long-term multidisciplinary rehabilitation to achieve meaningful functional restoration for the patient.
📚 Medical References
- brachial plexus surgery in obstetrical palsy, Hand Clin 11:583, 1995.
- Gilbert A, Razabone R, Amar-Khodja S: Indications and results of brachial plexus surgery in obstetrical palsy, Orthop Clin North Am 19:91, 1988.
- Gilbert A, Tassin JL: Surgical repair of the brachial plexus in obstetric paralysis, Chirurgie 110:70, 1984.
- Goddard NJ, Fixsen JA: Rotation osteotomy of the humerus for birth injuries of the brachial plexus, J Bone Joint Surg 66B:257, 1984.
- Green WT, Tachdjian MO: Correction of residual deformity of the shoulder from obstetrical palsy, J Bone Joint Surg 45A:1544, 1963.
- Greenwald AG, Schute PC, Shiveley JL: Brachial plexus birth palsy: a 10-year report on the incidence and prognosis, J Pediatr Orthop 4:689, 1984.
- Grossman JAI, Ditaranto P, Yaylali I, et al: Shoulder function following late neurolysis and bypass grafting for upper brachial birth injuries, J Hand Surg 29B:356, 2004.
- Grossman JAI, Price AE, Tidwell MA, et al: Outcome after later combined brachial plexus and shoulder surgery after birth trauma, J Bone Joint Surg 85B:1166, 2003.
- Hardy AE: Birth injuries of the brachial plexus: incidence and prognosis, J Bone Joint Surg 63B:98, 1981.
- Hentz V, Meyer R: Brachial plexus microsurgery in children, Microsurgery 12:175, 1991.
- Hoffer MM, Phipps GJ: Closed reduction and tendon transfer for treatment of dislocation of the glenohumeral joint secondary to brachial plexus birth palsy, J Bone Joint Surg 80A:997, 1998.
- Hoffer MM, Wickenden R, Roper R: Brachial plexus birth palsies: results of tendon transfers to the rotator cuff, J Bone Joint Surg 60A:691, 1978.
- Hui JHP, Torodoe IP: Changing glenoid version after open reduction of shoulders in children with obstetric brachial plexus palsy, J Pediatr Orthop 23:109, 2003.
- Jackson ST, Hoffer MM, Parrish N: Brachial plexus palsy in the newborn, J Bone Joint Surg 70A:1217, 1988.
- Jones SJ: Diagnostic value of peripheral and spinal somatosensory evoked potential in traction lesions of the brachial plexus, Clin Plast Surg 2:167, 1984.
- Kawabata H, Masada K, Tsuyuguchi Y, et al: Early microsurgical reconstruction in birth palsy, Clin Orthop Relat Res 215:233, 1987.
- Kirkos JM, Papadopoulos IA: Late treatment of brachial plexus palsy secondary to birth injuries: rotational osteotomy of the proximal part of the humerus, J Bone Joint Surg 80A:1477, 1998.
- Klumpke A: Paralysies radiculaires du plexus brachial; paralysies radiculaires totales; paralysies radiculaires inferieures; de la partipation des fi lets sympathiques oculopupillaires dan ces paralysies, Rev Med 5:739, 1885.
- Leffert RD: Clinical diagnosis, testing, and electromyographic study in brachial plexus traction injuries, Orthop Clin North Am 237:24, 1988.
- McDaid PJ, Kozin SH, Thoder JJ, et al: Upper extremity limblength discrepancy in brachial plexus palsy, J Pediatr Orthop 22:364, 2002.
- Meyer RD: Treatment of adult and obstetrical
You Might Also Like