Introduction to the Biomechanics of Knee Arthroplasty
The ultimate goal of Total Knee Arthroplasty (TKA) is the relief of pain and the restoration of native joint function. Achieving this requires a profound understanding of the biomechanics of knee arthroplasty. The human knee is not a simple hinge; it is a complex, dynamic joint governed by intricate articular geometry and a sophisticated network of ligamentous restraints. Modern prosthetic designs attempt to reproduce these normal knee kinematics closely, balancing the need for functional range of motion with the tribological demands of minimizing polyethylene contact stresses.
This comprehensive guide explores the kinematics of the native knee, the biomechanical rationale behind posterior cruciate ligament (PCL) retention versus substitution, principles of axial and rotational alignment, and the step-by-step surgical execution required to achieve a biomechanically optimized TKA.
Native Knee Kinematics and Triaxial Motion
Knee motion during normal gait has been extensively studied and is recognized to be vastly more complex than simple flexion and extension. Motion occurs simultaneously in three separate planes during the normal gait cycle, a phenomenon referred to as "triaxial motion."
The Helical Axis and the Screw-Home Mechanism
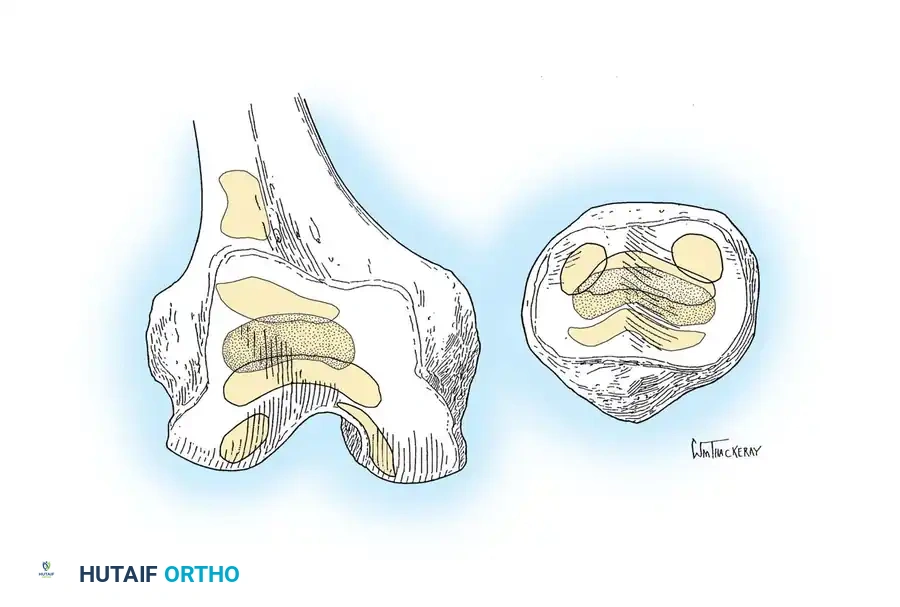
Knee flexion occurs around a constantly varying transverse axis, which describes a J-shaped curve around the femoral condyles rather than a fixed center of rotation.
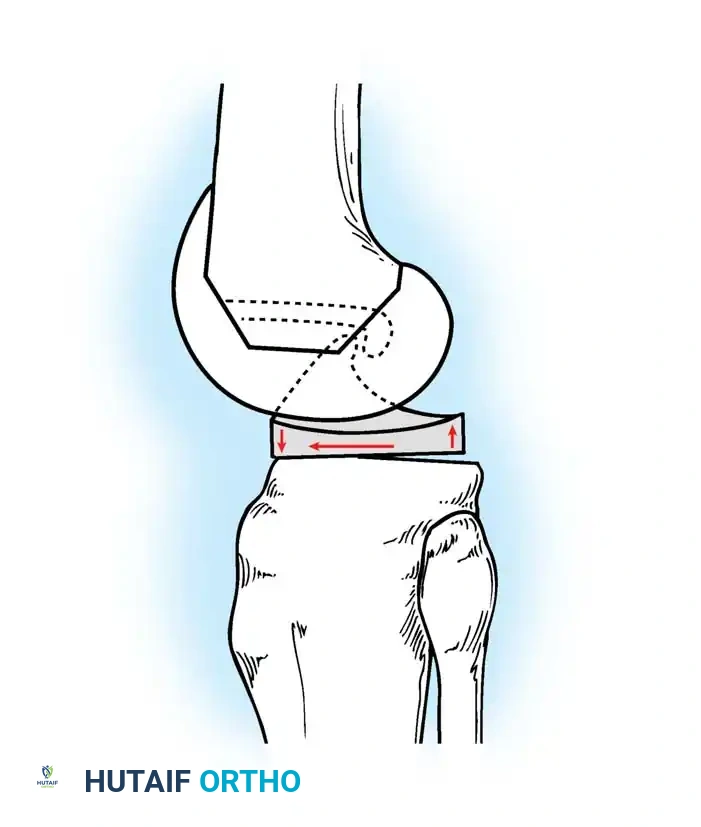
Dennis et al. utilized dynamic fluoroscopy coupled with three-dimensional CT scans to demonstrate that the flexion axis varies in a helical fashion. In the normal knee, there is an asymmetric posterior translation (rollback) of the femoral condyles on the tibia during flexion:
* Medial Femoral Condyle: Averages only 2 mm of posterior translation.
* Lateral Femoral Condyle: Averages 21 mm of posterior translation.
This medially based pivoting pattern explains the obligatory external rotation of the tibia on the femur during terminal extension—classically known as the "screw-home mechanism"—and the corresponding internal rotation of the tibia during knee flexion.
Clinical Pearl: The inability of early hinge-type knee prosthesis designs to accommodate this complex triaxial motion and its attendant torsional stresses led to catastrophic early aseptic loosening. Modern designs must account for this rotational freedom.
Gait Cycle Kinematics
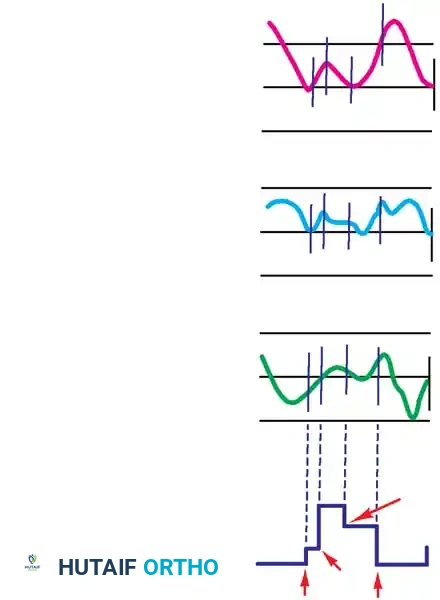
The use of gait laboratories has become an indispensable tool in prosthesis design. Electrogoniometric measurements of the triaxial motion of the normal knee during walking reveal distinct functional requirements.
According to Kettlekamp's kinematic studies of activities of daily living, the knee requires specific degrees of flexion to function optimally:
* Swing phase of normal gait: 67 degrees
* Stair climbing: 83 degrees
* Descending stairs: 90 degrees
* Rising from a standard chair: 93 degrees
Prosthetic Design: PCL-Retaining vs. PCL-Substituting
Since the concurrent development of PCL-retaining (Cruciate Retaining, CR) and PCL-substituting (Posterior Stabilized, PS) prostheses, the relative biomechanical merits of each have been fiercely debated. Both designs boast excellent 10- to 15-year survivorship, yet they achieve femoral rollback and stability through entirely different mechanisms.
Biomechanics of PCL Retention (CR)
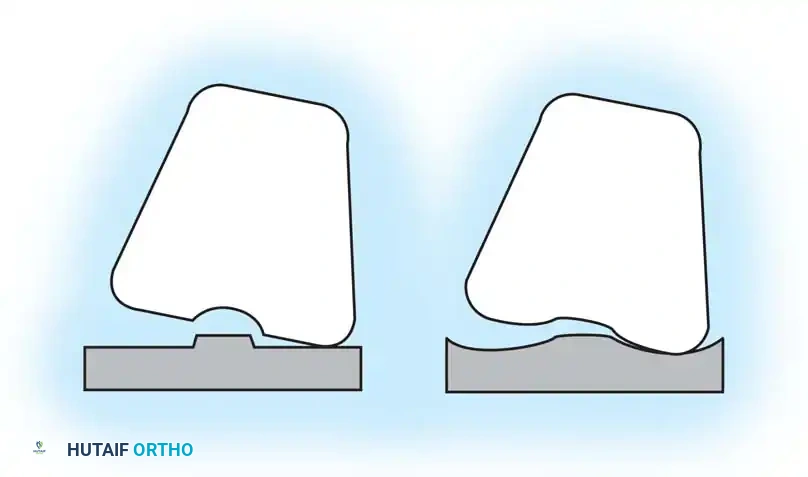
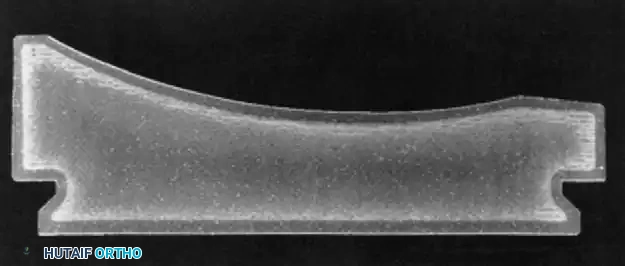
PCL retention relies on the native ligament to achieve effective femoral rollback. To accommodate this, the tibial articular surface of a CR prosthesis is typically flatter (less conforming) in the sagittal plane.
While retaining the PCL preserves native proprioception and theoretically provides a more symmetrical gait (especially during stair climbing, as noted by Andriacchi and Galante), it presents significant surgical challenges. The PCL must be perfectly balanced. A PCL that is too tight in flexion will cause excessive femoral rollback, driving the femoral condyles to override the posterior edge of the tibial polyethylene, leading to accelerated posterior wear. Conversely, an incompetent PCL leads to paradoxical anterior tibial translation during flexion, severely limiting range of motion and increasing anterior polyethylene wear.
Biomechanics of PCL Substitution (PS)
In PCL-substituting designs, the native PCL is resected. Posterior displacement (rollback) in flexion is mechanically forced by a tibial post contacting a femoral cam.
This cam-post mechanism ensures uniform and reproducible femoral rollback. Originally, critics argued that the added prosthetic constraint would transfer excessive shear stress to the prosthesis-bone interface, leading to early aseptic loosening. However, long-term data has proven the loosening rates between CR and PS designs to be statistically similar.
Surgical Warning: The tibial post in PS designs is a known site of wear and potential breakage. This risk is exponentially increased if the femoral component is implanted in a flexed position, if the tibial slope is excessive, or if the knee is allowed to hyperextend, causing anterior impingement of the femoral box against the post.
Patellofemoral Mechanics and Joint Line Elevation
The patellofemoral joint functions with a larger extensor lever arm when femoral rollback moves the tibial tubercle more anteriorly relative to the femur.
Patellofemoral mechanics are highly sensitive to joint line elevation. CR designs do not tolerate significant alteration of the preoperative joint line. PS designs are slightly more forgiving of mild joint line elevation; however, elevating the joint line alters the relationship of the patella to the trochlear groove.
In PS designs, the femoral component features an intercondylar box to accommodate the cam mechanism. If hypertrophic synovium or a prominent quadriceps tendon nodule catches in this box during extension, it results in "patellar clunk syndrome," a painful complication unique to posterior-stabilized knees.
Surgical Technique: Positioning, Approach, and Alignment
Achieving the biomechanical goals of TKA requires meticulous surgical execution, beginning with patient positioning and culminating in precise bone resection.
Patient Positioning and Preparation
- Anesthesia & Tourniquet: The patient is placed supine. Regional anesthesia (spinal) is preferred to reduce blood loss and DVT risk. A pneumatic tourniquet is applied to the proximal thigh.
- Leg Positioning: The leg is placed in a specialized leg holder (e.g., morph board or standard post) that allows for hyperflexion (at least 120 degrees) and stable positioning during bone cuts.
- Draping: Standard sterile orthopedic draping is utilized, ensuring the hip is free to assess overall limb alignment.
Surgical Approach
The standard medial parapatellar approach remains the workhorse of TKA.
* A midline longitudinal skin incision is made.
* The arthrotomy begins proximally in the quadriceps tendon, skirts the medial border of the patella, and extends distally to the medial side of the tibial tubercle.
* The patella is everted (or subluxated laterally, depending on surgeon preference and tissue tension).
* The deep infrapatellar fat pad is partially excised to visualize the lateral tibial plateau, taking care not to damage the patellar tendon insertion.
Axial and Rotational Alignment Principles
Numerous studies correlate the long-term success of TKA with the restoration of a neutral mechanical axis. Malalignment leads to tibiofemoral instability, patellar maltracking, stiffness, and catastrophic polyethylene failure.
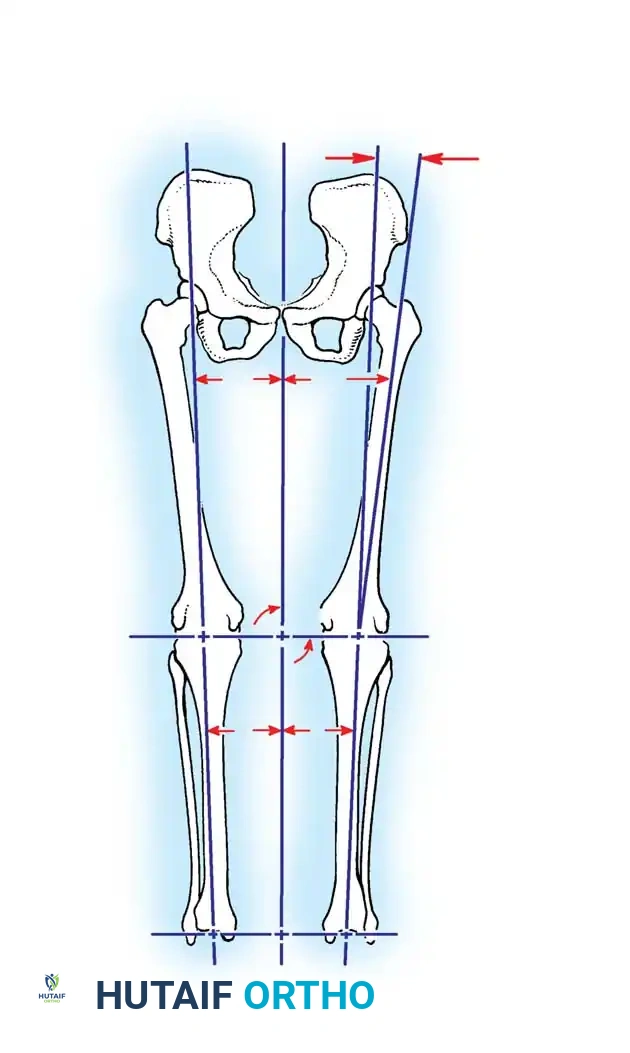
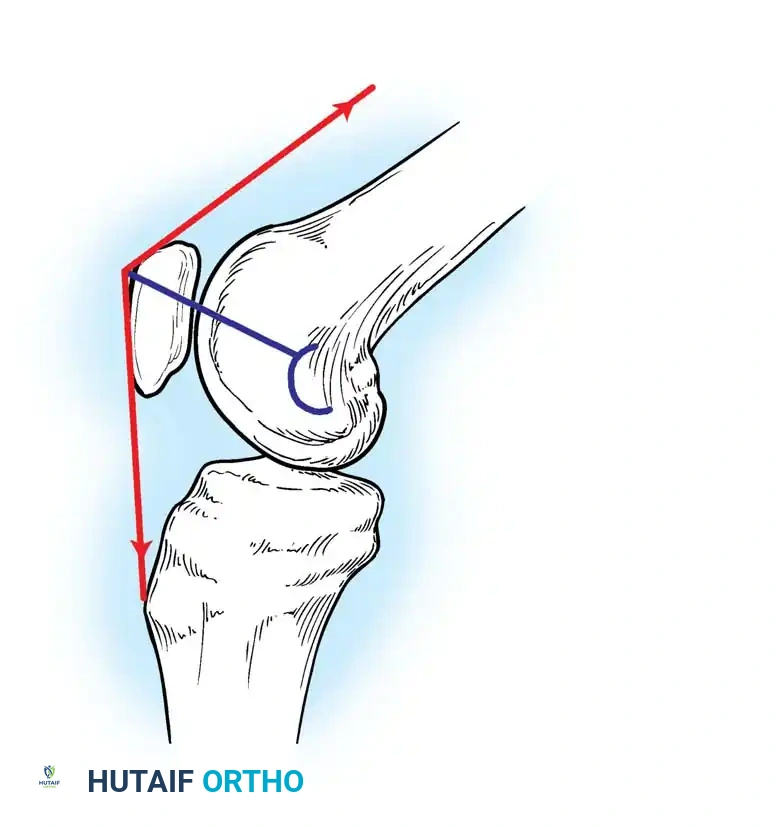
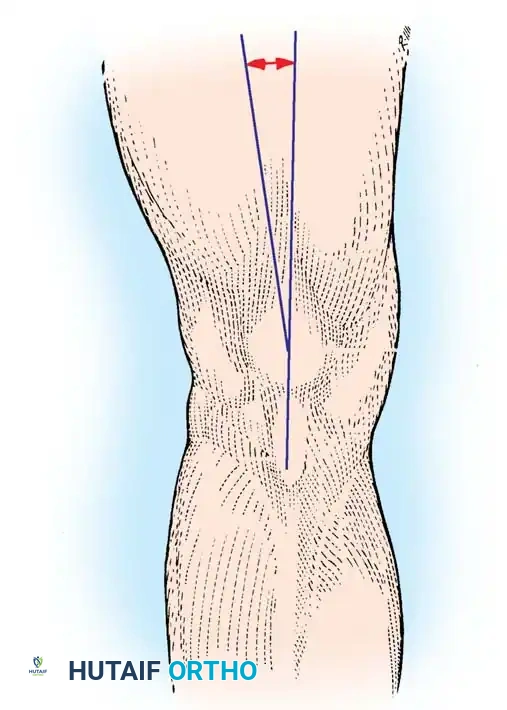
- Mechanical Axis: Defined as a line drawn from the center of the femoral head to the center of the talar dome. In a well-aligned TKA, this axis should pass directly through the center of the knee joint.
- Anatomical Axis: The anatomical axes of the femur and tibia normally form a valgus angle of 6 ± 2 degrees.
Rotational Alignment of the Femoral Component:
Proper femoral rotation is critical for balancing the flexion gap and ensuring central patellar tracking. The femoral component is typically externally rotated 3 degrees relative to the posterior condylar axis. This can be cross-referenced using:
1. The Surgical Transepicondylar Axis (TEA): From the lateral epicondylar prominence to the medial epicondylar sulcus.
2. Whiteside’s Line (Anteroposterior Axis): A line drawn from the deepest part of the trochlear groove to the center of the intercondylar notch.
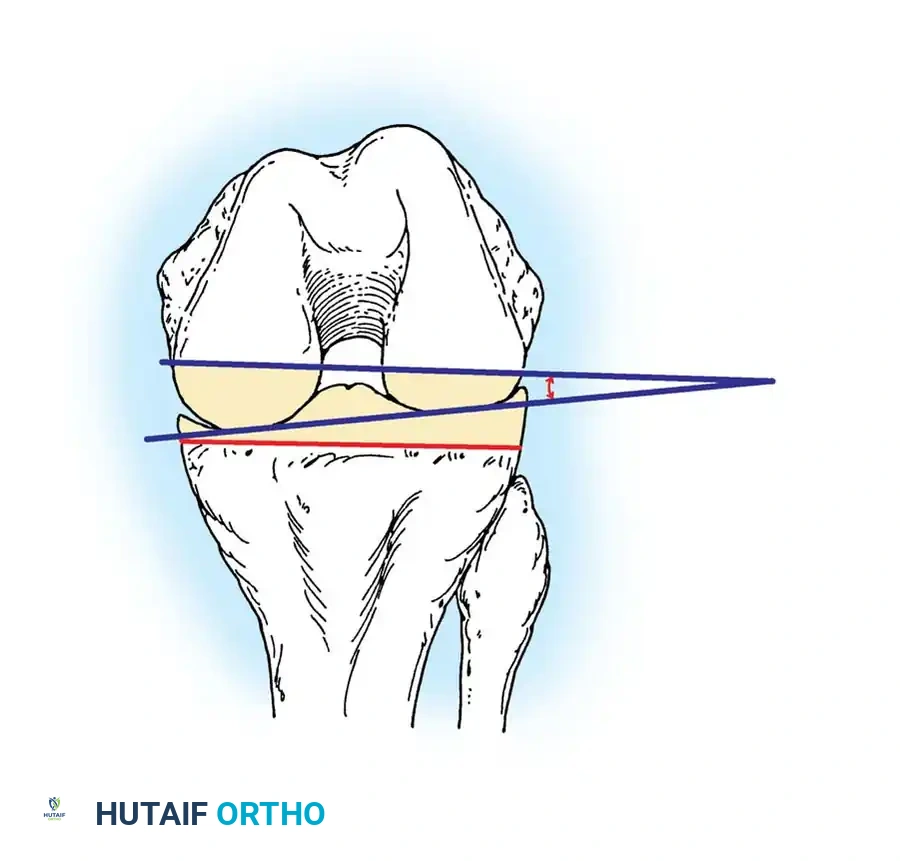
Intraoperative Gap Balancing and Soft Tissue Management
The essence of a biomechanically sound TKA lies in creating equal, rectangular flexion and extension gaps.

Managing the Flexion and Extension Gaps
- Extension Gap: Governed by the distal femoral cut and the proximal tibial cut, tensioned by the posterior capsule and collateral ligaments.
- Flexion Gap: Governed by the posterior femoral cut and the proximal tibial cut, tensioned by the collateral ligaments and the PCL (in CR knees).
If the PCL is retained, it frequently requires partial release (recession) off the tibia to allow adequate flexion and prevent the flexion gap from becoming too tight. Mahoney et al. demonstrated that to achieve near-normal strain, a retained PCL must be balanced to an accuracy of approximately 1 mm—a highly demanding surgical feat.
Deformity Correction
For severe fixed deformities, PCL substitution is often biomechanically superior. Laskin et al. reported that in patients with fixed varus or valgus deformities >15 degrees associated with flexion contractures, attempting to retain the PCL resulted in lesser postoperative flexion and residual contractures. The contracted PCL acts as a tether on the concave side of the deformity; resecting it allows for more profound and reliable soft tissue balancing.
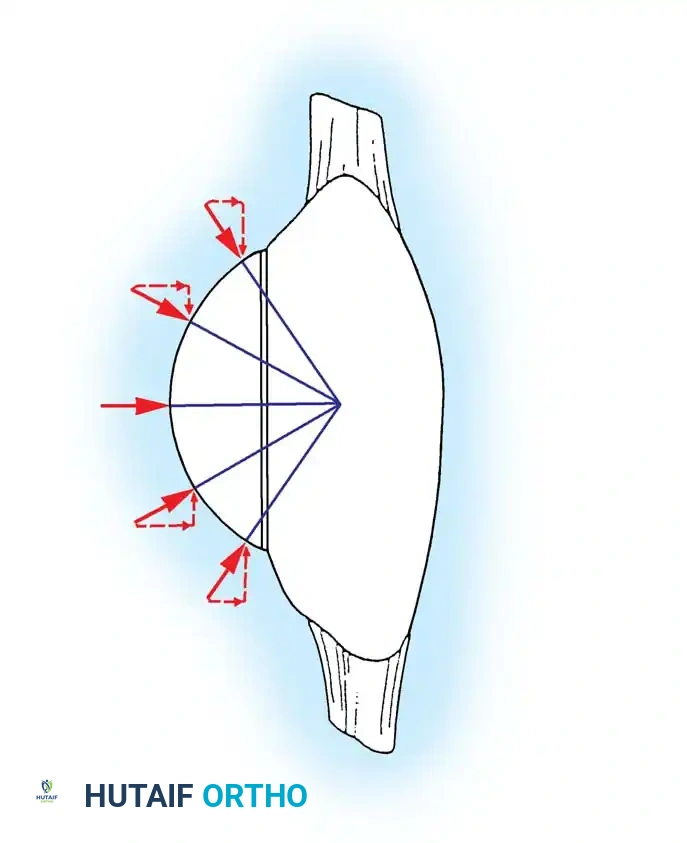
Tribology and Polyethylene Wear Mechanisms
Polyethylene wear is a primary limiting factor in the longevity of a TKA. Wear is dictated by prosthesis design, material properties (e.g., highly cross-linked polyethylene), and in vivo kinematics.

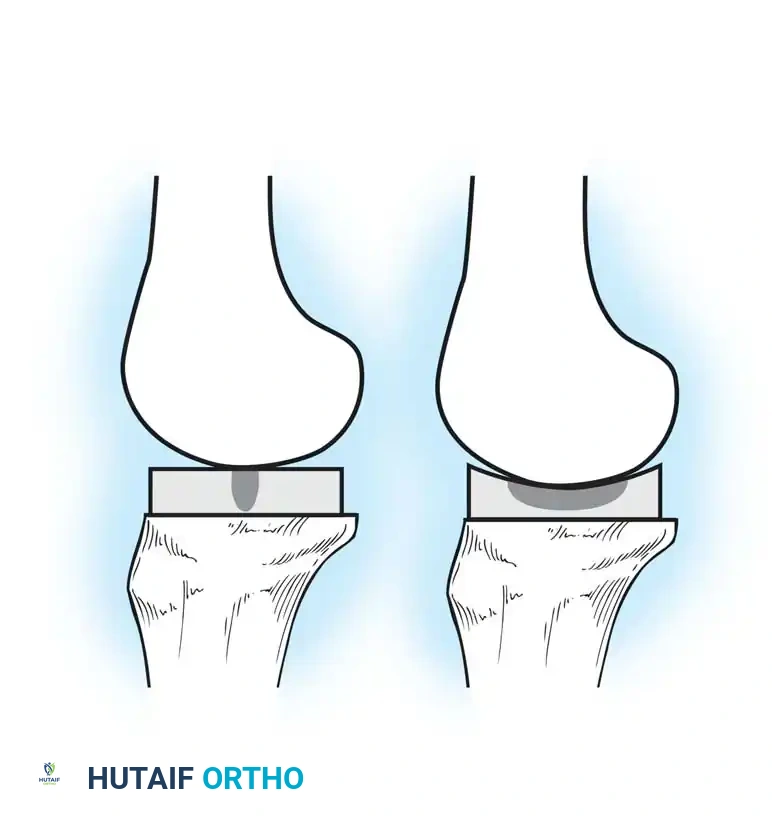
Because CR prostheses utilize a flatter tibial articular surface to permit femoral rollback, the contact area between the femur and tibia is reduced. This decreased conformity results in significantly higher polyethylene contact stresses.

If the PCL is excessively tight, it acts as a fulcrum during flexion, driving the femoral condyles into the posterior lip of the tibial insert. This edge-loading dramatically amplifies contact stress, leading to delamination, pitting, and accelerated posterior wear.
Conversely, while PS designs offer higher conformity and lower articular contact stresses, they introduce a new wear interface: the cam-post articulation. Aseptic loosening secondary to osteolysis from post-generated polyethylene debris remains a recognized failure mode in PS knees.
Postoperative Protocols and Rehabilitation
A biomechanically perfect surgery can be compromised by inadequate postoperative care. Modern TKA rehabilitation emphasizes rapid mobilization to prevent stiffness and thromboembolic events.
Immediate Postoperative Phase (Days 0-2)
- Weight-Bearing: Weight-bearing as tolerated (WBAT) immediately post-surgery with an assistive device (walker or crutches).
- Range of Motion (ROM): Continuous Passive Motion (CPM) machines are largely obsolete. Active and active-assisted ROM exercises are initiated on postoperative day 0. The goal is to achieve 0 to 90 degrees of flexion prior to hospital discharge.
- VTE Prophylaxis: Strict adherence to AAOS guidelines for venous thromboembolism prophylaxis. Depending on patient risk stratification, this may include early ambulation, mechanical prophylaxis (SCDs), and pharmacological agents (e.g., Aspirin, LMWH, or direct oral anticoagulants) for 14 to 35 days.
Intermediate to Late Rehabilitation (Weeks 2-12)
- Strengthening: Focus shifts to quadriceps activation and strengthening to overcome arthrogenic muscle inhibition. Closed kinetic chain exercises are prioritized to protect the patellofemoral joint.
- Proprioception: Balance and proprioceptive training are critical, particularly in PS knees where native cruciate mechanoreceptors have been excised.
- Milestones: By 6 weeks, patients should achieve full extension (0 degrees) and at least 110-120 degrees of flexion, allowing them to perform all activities of daily living, including stair climbing and rising from a chair without upper extremity assistance.
By meticulously respecting the biomechanics of knee arthroplasty—from understanding native kinematics to executing precise surgical alignment and gap balancing—the orthopedic surgeon can reliably deliver a stable, durable, and highly functional joint reconstruction.
