Biology and Surgical Management of Spinal Infections
Key Takeaway
Spinal infections primarily originate in the highly vascularized vertebral metaphyses and cartilaginous endplates rather than the avascular intervertebral disc. Pyogenic bacteria typically disseminate via arterial routes, while tuberculous infections often utilize the venous system, specifically Batson's plexus. Understanding this complex microvascular anatomy is critical for accurate diagnosis, determining surgical indications, and executing meticulous operative debridement and stabilization in affected patients.
Comprehensive Introduction and Patho-Epidemiology
Spinal infections represent a profoundly complex and increasingly prevalent spectrum of pathologies that challenge the diagnostic acumen and surgical proficiency of orthopedic spine surgeons. Encompassing pyogenic spondylodiscitis, vertebral osteomyelitis, and spinal epidural abscesses, these conditions threaten the structural integrity of the axial skeleton and the functional viability of the neural elements. Historically viewed as a rare clinical entity, the incidence of spinal infections has surged over the past two decades. This epidemiologic shift is multifactorial, driven by an aging population, the escalating prevalence of medical comorbidities such as diabetes mellitus and chronic kidney disease, the widespread use of immunosuppressive and biologic therapies, and the devastating systemic impact of the global opioid and intravenous drug use (IVDU) epidemics.
The patho-epidemiology of spinal infections is intrinsically linked to the microbiological profile of the invading organisms and the host's immune competence. Staphylococcus aureus, encompassing both methicillin-susceptible (MSSA) and methicillin-resistant (MRSA) strains, remains the undisputed primary pathogen, responsible for over 50% to 60% of all pyogenic spinal infections. The propensity of S. aureus to form robust, antibiotic-resistant biofilms on necrotic bone and avascular cartilaginous surfaces makes medical eradication exceedingly difficult without surgical debridement. Gram-negative bacilli, including Escherichia coli and Pseudomonas aeruginosa, are increasingly isolated, particularly in the elderly, immunocompromised hosts, and patients with concurrent genitourinary tract infections or indwelling catheters. Furthermore, the resurgence of Mycobacterium tuberculosis (Pott's disease) in endemic regions and among immigrant populations necessitates a high index of suspicion, as its indolent clinical presentation and predilection for profound anterior column destruction often lead to catastrophic kyphotic deformity before a definitive diagnosis is established.
Understanding the temporal progression of these infections is paramount for the operating surgeon. The classic triad of back pain, fever, and neurological deficit is present in a minority of patients, often leading to delayed diagnosis. The initial infectious nidus typically establishes itself in the subchondral bone of the vertebral body adjacent to the endplate. As the bacterial load exponentially increases, the localized inflammatory response generates microthrombosis and focal ischemia, leading to trabecular necrosis. The infection subsequently breaches the cartilaginous endplate, invading the avascular intervertebral disc space. In the adult spine, the avascularity of the nucleus pulposus creates an immunologically privileged sanctuary where bacteria proliferate unchecked by host macrophages or systemic antimicrobial agents. This relentless progression ultimately culminates in the destruction of the anterior load-bearing column, predisposing the patient to segmental instability, pathological fractures, and the contiguous spread of purulent material into the epidural space, directly threatening the spinal cord and cauda equina.
The Role of Biofilms in Spinal Sepsis
A critical concept in the contemporary understanding of spinal infections is the formation of bacterial biofilms. Once pathogenic bacteria adhere to devitalized bone, cartilaginous endplates, or iatrogenically introduced spinal instrumentation, they undergo a phenotypic shift, encasing themselves in a self-synthesized extracellular polymeric substance (EPS). This biofilm matrix acts as a formidable mechanical and biochemical barrier, rendering the embedded bacteria up to 1,000 times more resistant to systemic antibiotics compared to their planktonic counterparts. The presence of biofilms dictates the absolute necessity of radical surgical debridement; antibiotics alone cannot penetrate the EPS matrix sufficiently to achieve sterilization. The surgical objective, therefore, is not merely to decompress the neural elements, but to meticulously resect all biofilm-laden necrotic tissue until healthy, bleeding cancellous bone is encountered, thereby transforming a chronic, recalcitrant infection into an acute, biologically active surgical bed capable of supporting arthrodesis.
Detailed Surgical Anatomy and Biomechanics
A profound knowledge of the structure, composition, and microvasculature of the spinal elements is the absolute prerequisite for understanding the pathogenesis, progression, and surgical management of spinal infections. Historically, the intervertebral disc was erroneously identified as the primary nidus for spinal infections. However, contemporary evidence-based literature unequivocally points to the highly vascularized metaphyses and cartilaginous endplates as the primary starting areas for blood-borne (hematogenous) infections. Today, the intervertebral disc space is considered the primary starting area only in cases of direct inoculation, such as iatrogenic introduction during surgery or discography.
Microscopic Anatomy of the Intervertebral Disc and Endplate
In 1945, Coventry, Ghormley, and Kernohan provided a seminal description of the microscopic anatomy of the intervertebral disc and its contiguous structures. Their critical conclusion was that in adults older than 30 years, the intervertebral disc is essentially avascular; it receives its nutrition entirely from tissue fluid diffusion rather than from a direct blood supply.
They identified multiple perforations in the bony endplates of the vertebral bodies, which correspond directly with the marrow cavities. These perforations are arranged in three distinct anatomical zones:
1. The Central Zone: Characterized by numerous small perforations.
2. The Peripheral Zone: Characterized by fewer, but significantly larger, perforations.
3. The Epiphyseal Ring: A dense ring surrounding the endplate that overlaps the outer surface of the vertebral body, joining the more concave surface of the central and peripheral zones internally.
Adjacent to the bony endplate lies the cartilaginous plate, composed of hyaline cartilage, which forms the critical inner boundary between the osseous vertebral body and the fibrous intervertebral disc.
Clinical Pearl: The avascular nature of the adult intervertebral disc makes it an immunologically privileged site. Once bacteria breach the cartilaginous endplate and enter the disc space, the lack of direct blood supply severely limits the efficacy of the host immune response and systemic antibiotic penetration, often necessitating surgical debridement.
In 1981, Inoue further elucidated the biomechanical adherence of the disc to the vertebral endplate. He discovered that the disc is firmly adherent at its periphery, where two-thirds of its collagenous fibers insert perpendicularly into the endplate (Sharpey's fibers). Conversely, the central portion is less firmly attached, with fibers running parallel to the endplate. This specific architectural composition facilitates the diffusion of nutrients through the endplate perforations into the central nucleus pulposus without compromising the structural integrity of the motion segment under axial load.
Arterial Supply and Microvasculature
The arterial and venous supply to the vertebrae dictates the specific patterns of hematogenous bacterial seeding. In 1959, Wiley and Trueta demonstrated marked similarities in the arterial and venous supply across the cervical, thoracic, and lumbar levels. At each vertebral level, nutrient vessels derived from the vertebral, intercostal, or lumbar arteries enter the vertebral body.
Posterior spinal branch arteries enter the spinal canal through each neural foramen. These arteries bifurcate into ascending and descending branches that anastomose with corresponding branches at adjacent levels. This posterior network converges centrally to enter a large posterior nutrient foramen.
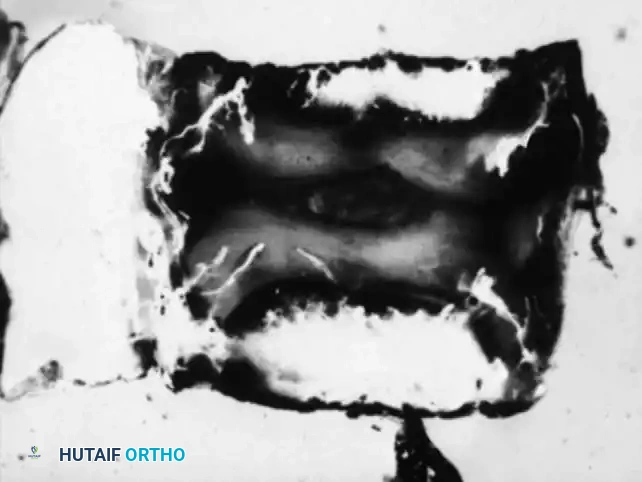
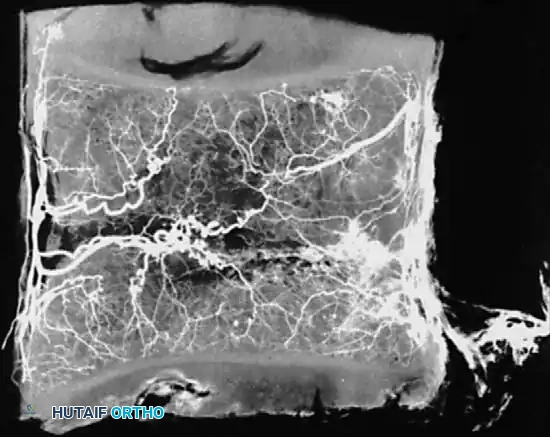
Whalen et al. investigated the microvasculature of the vertebral endplates, describing vessels oriented obliquely within the cartilage, directing toward the intervertebral disc. These vessels originate from circumferential vessels fed by the arterial plexus outside the perichondrium or from adjacent metaphyseal marrow vessels.
Crucially, Whalen's team concluded that the intervertebral disc is avascular even in infants, whereas the surrounding cartilaginous material is highly vascular. The cartilaginous endplate represents the anatomical terminus of the arterial supply, regardless of the patient's age. The sluggish flow at these terminal arterial capillary loops creates an ideal environment for blood-borne pathogens to precipitate and establish a primary focus of osteomyelitis.
Venous Drainage and Batson's Plexus
The venous drainage of the spine is equally critical to the pathophysiology of infection. First described by Breschet in 1819 and expanded by Batson in 1940, the valveless pelvic venous plexus drains directly into the spinal venous plexus (Batson's plexus). This valveless, bidirectional flow perfectly explains the frequent metastasis of pelvic tumors and the spread of genitourinary infections to the spine.
In 1976, Crock and Yoshizawa mapped the venous microcirculation of the vertebral endplate. The venous system begins exactly where the arterial circulation ends. Large subvenous channels run horizontally and parallel to the endplate. This horizontal system drains through small vertical veins that perforate the endplate, connecting with horizontal vessels in the adjacent cancellous bone.
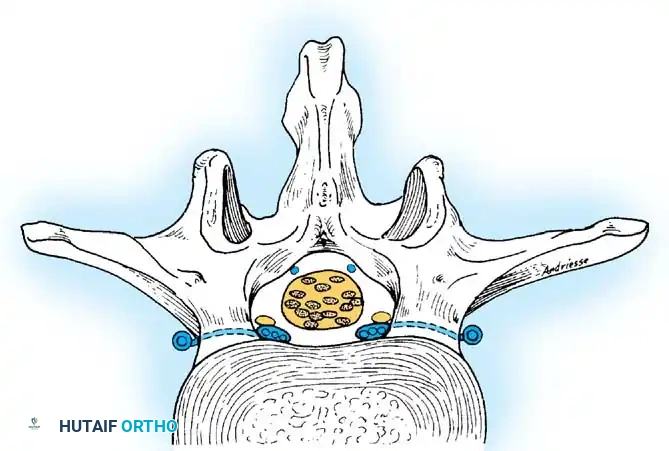
These vertical veins drain into the basivertebral system, converging to form the anterior internal venous plexus. Externally, these vessels anastomose with the anterior internal vertebral, posterior internal vertebral, and posterior radicular veins. The low-pressure, high-capacitance nature of the basivertebral venous system allows retrograde flow during periods of increased intra-abdominal pressure, facilitating the dissemination of pathogens from the pelvis directly into the vertebral bodies.
Exhaustive Indications and Contraindications
The management paradigm for spinal infections requires a delicate balance between conservative antimicrobial therapy and aggressive surgical intervention. While uncomplicated spondylodiscitis in a neurologically intact patient can often be managed with prolonged intravenous antibiotics and rigid immobilization, the threshold for surgical intervention must be strictly defined to prevent irreversible neurological catastrophe and severe biomechanical collapse. The decision-making process is highly individualized, factoring in the virulence of the organism, the degree of bony destruction, the patient's physiological reserve, and the presence of epidural extension.
Surgical intervention is definitively indicated when the structural integrity of the spinal column is compromised to the point of imminent or actual failure, or when the neural elements are subjected to mechanical compression. Epidural abscesses, particularly those located in the cervical or thoracic spine where the canal-to-cord ratio is minimal, warrant emergent surgical decompression. The presence of a progressive neurological deficit is an absolute, non-negotiable indication for immediate operative intervention. Furthermore, the failure of medical management—defined as persistent or worsening clinical symptoms, rising inflammatory markers (C-reactive protein [CRP] and erythrocyte sedimentation rate [ESR]), or progressive bony destruction on serial imaging despite 4 to 6 weeks of culture-directed, optimally dosed intravenous antibiotics—mandates a surgical approach for source control.
Conversely, absolute contraindications to surgery are rare but must be meticulously evaluated. Patients with profound physiological derangements, such as uncorrectable coagulopathy, severe multi-organ failure, or terminal medical illness precluding general anesthesia, may not survive the physiological insult of a major spinal reconstruction. In such scenarios, palliative decompression, minimally invasive drainage, or exclusively medical management must be considered. Relative contraindications include diffuse, multi-level non-contiguous osteomyelitis without focal instability or cord compression, where the morbidity of multi-level radical debridement outweighs the potential biomechanical benefits.
| Category | Specific Clinical Scenario | Surgical Rationale & Management Strategy |
|---|---|---|
| Absolute Indication | Progressive Neurological Deficit | Emergent anterior or posterior decompression to relieve mechanical pressure from epidural abscess, granulation tissue, or retropulsed bone. Time is critical for neurological recovery. |
| Absolute Indication | Spinal Instability / Kyphotic Deformity | Radical anterior debridement of necrotic bone, followed by structural grafting (titanium cage/autograft) and posterior instrumented stabilization to restore the load-bearing column. |
| Absolute Indication | Epidural Abscess with Cord Compression | Evacuation of purulence to prevent ischemic or compressive myelopathy. Requires laminectomy or anterior corpectomy depending on the ventral/dorsal location of the abscess. |
| Relative Indication | Failure of Medical Management | Source control is required when biofilms prevent antibiotic efficacy. Debridement removes the necrotic nidus, allowing systemic antibiotics to penetrate the surgical bed. |
| Relative Indication | Intractable Pain Limiting Mobilization | Severe mechanical back pain indicates micro-instability. Surgical stabilization eliminates pathological motion, providing immediate pain relief and facilitating early mobilization. |
| Contraindication | Medically Unfit for General Anesthesia | Severe cardiopulmonary compromise or uncorrectable coagulopathy. Consider CT-guided percutaneous drainage of paraspinal/epidural abscesses as a temporizing measure. |
| Contraindication | Diffuse Non-Contiguous Disease (No Compression) | Extensive surgical morbidity outweighs benefits. Manage with prolonged, targeted IV antimicrobial therapy and rigid orthotic bracing. |
Pre-Operative Planning, Templating, and Patient Positioning
The successful surgical execution of a complex spinal infection case is entirely predicated upon meticulous preoperative planning. The surgeon must synthesize a vast array of clinical, laboratory, and radiographic data to formulate a comprehensive surgical strategy that addresses decompression, debridement, and stabilization. The initial diagnostic workup must include a complete blood count with differential, comprehensive metabolic panel, blood cultures (ideally drawn during febrile spikes before antibiotic initiation), and baseline inflammatory markers (ESR, CRP, and Procalcitonin). If blood cultures are negative, a CT-guided percutaneous needle biopsy of the affected disc space or paraspinal fluid collection is mandatory to isolate the causative organism and guide targeted antimicrobial therapy.
Advanced neuroimaging is the cornerstone of preoperative templating. Gadolinium-enhanced Magnetic Resonance Imaging (MRI) is the gold standard modality. The surgeon must carefully evaluate T1-weighted, T2-weighted, and Short Tau Inversion Recovery (STIR) sequences. Active infection typically presents as T1 hypointensity and T2/STIR hyperintensity within the intervertebral disc and adjacent vertebral marrow, accompanied by loss of the normal intranuclear cleft. Following gadolinium administration, diffuse enhancement of the endplates, disc space, and epidural phlegmon or abscess is characteristic. The MRI dictates the required extent of neural decompression. Concurrently, a fine-cut, non-contrast Computed Tomography (CT) scan is indispensable for evaluating the true extent of osseous destruction, cortical bone loss, and the presence of pathological fractures. The CT scan allows the surgeon to template the size of the corpectomy defect, select appropriate structural grafts or titanium mesh cages, and meticulously plan pedicle screw trajectories, particularly in osteoporotic or anatomically distorted bone.
Patient positioning is a critical phase of the operation that directly impacts surgical exposure, intraoperative blood loss, and the prevention of perioperative complications. For a standard posterior approach (laminectomy, transforaminal debridement, and pedicle screw fixation), the patient is positioned prone on a radiolucent Jackson spinal table. Meticulous attention must be paid to padding all bony prominences (e.g., iliac crests, patellae, face) to prevent pressure necrosis. Crucially, the abdomen must hang completely free; any compression of the inferior vena cava will engorge the valveless Batson's venous plexus, leading to torrential epidural bleeding during the decompression phase.
For anterior approaches, positioning is dictated by the anatomical level of the pathology. For thoracic and thoracolumbar junction infections (T4-L1), the patient is placed in the lateral decubitus position for a transthoracic or thoracoabdominal approach. The right lateral decubitus position (left side up) is generally preferred to avoid mobilizing the liver and to access the aorta, which is structurally more resilient than the thin-walled inferior vena cava. For mid-to-lower lumbar infections (L2-L5), a supine or slightly oblique position is utilized for a retroperitoneal approach, allowing direct orthogonal access to the anterior column for radical corpectomy and cage placement.
Step-by-Step Surgical Approach and Fixation Technique
Because spinal infections predominantly destroy the anterior load-bearing column (the vertebral body and the intervertebral disc), the anterior approach is frequently considered the gold standard for radical debridement and structural reconstruction. This approach provides direct, unhindered access to the infected tissue, allowing the surgeon to perform a thorough corpectomy and place a load-sharing structural graft under direct visualization, thereby restoring sagittal alignment and biomechanical stability.
Anterior Debridement and Structural Grafting
-
Exposure and Vascular Mobilization: Depending on the spinal level, a left-sided retroperitoneal approach (lumbar) or a transthoracic approach (thoracic) is utilized. The left-sided approach is heavily favored in the lumbar spine to mobilize the robust aorta rather than the fragile, easily lacerated inferior vena cava. Once the prevertebral fascia is incised, the segmental vessels traversing the waist of the infected vertebral bodies are meticulously identified. These vessels must be doubly ligated and divided to allow safe, tension-free mobilization of the great vessels away from the operative corridor.
-
Radical Corpectomy and Debridement: The boundaries of the infection are identified using intraoperative fluoroscopy. The infected intervertebral discs above and below the involved vertebrae are excised using long-handled annulotomy knives and pituitary rongeurs. Using a high-speed burr, Leksell rongeurs, and angled curettes, the necrotic, purulent, and infected bone of the vertebral body is radically resected.
Surgical Warning: This is the most critical step of the operation. Debridement must be aggressive and relentless until healthy, bleeding cancellous bone is encountered at the superior and inferior vertebral endplates. Leaving behind avascular, necrotic bone or residual biofilm guarantees persistent infection, graft subsidence, and ultimate construct failure.
-
Epidural Decompression: If an epidural abscess or inflammatory phlegmon is present, the posterior longitudinal ligament (PLL) must be identified and carefully resected. This allows full visualization and decompression of the ventral dural sac. Epidural purulence is gently evacuated using suction and blunt nerve hooks, avoiding any manipulation of the fragile, inflamed neural elements.
-
Structural Reconstruction: Once the surgical bed is sterilized of gross purulence and all necrotic tissue is removed, the defect must be reconstructed. While autologous tricortical iliac crest bone graft remains the historical gold standard due to its osteogenic and immunologic properties, the morbidity of the harvest site and structural limitations in multi-level defects have led to a paradigm shift. Today, titanium mesh cages or expandable titanium implants, packed tightly with autograft or allograft, are increasingly preferred. Titanium is highly resistant to bacterial adherence and biofilm formation, providing immediate structural support and a high rate of successful arthrodesis even in the setting of active infection.
Posterior Instrumentation and Stabilization
In cases of significant anterior column destruction, multi-level debridement, or profound pre-operative instability, anterior column support alone is biomechanically insufficient. Supplemental posterior instrumentation is absolutely required to neutralize flexion-extension and rotational forces.
-
Pedicle Screw Fixation: Utilizing intraoperative fluoroscopy, robotic assistance, or stereotactic navigation, pedicle screws are placed at least one, and preferably two, intact vertebral levels above and below the infected segment. The trajectory must be precise to maximize cortical purchase, particularly as the adjacent bone may be osteoporotic due to regional hyperemia and disuse.
-
Avoidance of the Infected Zone: A critical biomechanical principle must be strictly adhered to: posterior laminectomy alone, without instrumented stabilization, is absolutely contraindicated in the presence of anterior column infection. Removing the posterior tension band in a spine that has already lost its anterior load-bearing capacity will inevitably lead to catastrophic kyphotic collapse, iatrogenic spinal cord compression, and severe deformity.
-
Irrigation and Closure: Following hardware placement, the surgical wound is subjected to copious, pulsatile irrigation with normal saline. Volumes exceeding 9 to 12 liters are routinely utilized to mechanically wash out planktonic bacteria and debris. Intrawound vancomycin powder (1 to 2 grams) may be applied locally to provide high bactericidal concentrations without systemic toxicity. Deep subfascial drains are placed to prevent postoperative epidural hematoma formation, followed by a meticulous, water-tight, multi-layer fascial closure to prevent dead space and subsequent seroma formation.
Complications, Incidence Rates, and Salvage Management
The surgical management of spinal infections is fraught with potential hazards. The combination of distorted anatomy, profound inflammatory hyperemia, friable tissues, and the physiological fragility of the patient cohort creates an environment where complications are not merely possible, but statistically probable. The operating surgeon must be intimately familiar with these risks and possess the technical repertoire to execute immediate salvage maneuvers.
Intraoperative complications largely revolve around the vascular and neural structures adjacent to the infected spine. The inflammatory process often obliterates normal anatomical planes, tethering the great vessels (aorta, inferior vena cava, common iliac veins) to the anterior longitudinal ligament. Aggressive retraction or inadvertent sharp dissection can result in life-threatening hemorrhage. Neural injuries, including incidental durotomies or direct trauma to the spinal cord or nerve roots, can occur during the evacuation of hardened epidural phlegmon or the resection of the posterior longitudinal ligament.
Postoperative complications are equally challenging. Despite radical debridement and appropriate antimicrobial therapy, persistent or recurrent infection remains a significant risk, particularly in immunocompromised hosts or those with retained hardware. Hardware failure, including pedicle screw pullout, cage subsidence, or rod fracture, occurs when the biological process of arthrodesis fails to outpace the mechanical fatigue life of the titanium implants. Pseudoarthrosis, the failure of solid bone fusion, necessitates revision surgery if accompanied by pain or progressive deformity.
| Complication | Estimated Incidence | Prevention Strategy & Salvage Management |
|---|---|---|
| Major Vascular Injury (Aorta/IVC) | 1% - 3% | Prevention: Meticulous blunt dissection; preoperative vascular surgery consult for severe prevertebral tethering. Salvage: Immediate packing, direct pressure, primary prolene suture repair, or emergent vascular surgery intervention. |
| Incidental Durotomy (Dural Tear) | 5% - 10% | Prevention: Avoid sharp dissection near the inflamed ventral dura; use blunt hooks for epidural phlegmon. Salvage: Primary 4-0 Nurolon repair if accessible. Use dural sealants, muscle patches, and maintain subfascial drains on low suction. |
| Cage Subsidence / Hardware Failure | 10% - 15% | Prevention: Ensure endplate preparation preserves the peripheral cortical ring; use endplate-spanning cages; robust posterior fixation. Salvage: Revision surgery to extend posterior instrumentation and potentially exchange the anterior cage. |
| Persistent / Recurrent Infection | 8% - 12% | Prevention: Radical debridement to bleeding bone; copious irrigation; strict adherence to infectious disease antibiotic protocols. Salvage: Return to the operating room for repeat irrigation and debridement (I&D); optimization of host nutrition and immunity. |
| Postoperative Epidural Hematoma | 2% - 4% | Prevention: Meticulous bipolar hemostasis of epidural veins; use of hemostatic matrices (Gelfoam/Thrombin); routine use of subfascial drains. Salvage: Emergent MRI followed by immediate return to the OR for surgical evacuation if causing neurological deficit. |
| Pseudoarthrosis (Non-union) | 10% - 20% | Prevention: Aggressive decortication; use of high-quality structural autograft or viable allograft; rigid immobilization. Salvage: Posterior revision with extension of fusion, robust decortication, and application of bone morphogenetic protein (BMP) off-label. |
Phased Post-Operative Rehabilitation Protocols
The surgical intervention, regardless of its technical perfection, represents merely the first phase in the comprehensive management of a spinal infection. The postoperative period requires a highly coordinated, multidisciplinary approach involving the orthopedic spine surgeon, infectious disease specialists, physical medicine and rehabilitation physicians, and dedicated physical therapists. The ultimate goals of the rehabilitation protocol are the complete eradication of the pathogen, the achievement of solid osseous arthrodesis, and the restoration of the patient's baseline functional mobility.
Phase 1: Acute Inpatient Management (Weeks 0-2)
Immediately following surgery, the primary focus is on hemodynamic stability, pain control, and the initiation of targeted antimicrobial therapy. Intravenous antibiotics are continued postoperatively, with the empirical regimen rapidly adjusted and strictly tailored based on the final intraoperative deep tissue cultures and sensitivity profiles. Early mobilization is paramount; patients are encouraged to sit on the edge of the bed and ambulate with physical therapy as early as postoperative day one. This aggressive early mobilization is critical to mitigate the risks of deep vein thrombosis, pulmonary atelectasis, and rapid muscular deconditioning. Depending on the rigidity of the internal fixation and the quality of the patient's bone, a rigid cervicothoracic or thoracolumbosacral orthosis (TLSO) may be prescribed. The orthosis serves to restrict micromotion at the operative site, reducing mechanical pain and promoting the biological environment necessary for arthrodesis.
Phase 2: Subacute Recovery and Eradication (Weeks 2-6)
Upon discharge to a rehabilitation facility or home, the patient transitions to the subacute phase. The standard of care dictates a minimum of 6 weeks of continuous, culture-directed intravenous antibiotics, typically administered via a Peripherally Inserted Central Catheter (PICC). During this period, the patient undergoes weekly serological monitoring of C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR). The CRP is a highly sensitive, acute-phase reactant; a steady, logarithmic decline in CRP is the most reliable clinical indicator of successful infection eradication. Conversely, a plateau or secondary rise in CRP warrants immediate clinical re-evaluation and potential advanced imaging to rule out recurrent abscess formation. Physical therapy focuses on isometric core strengthening, gait training, and progressive endurance exercises, strictly avoiding heavy lifting, deep bending, or extreme twisting maneuvers.
Phase 3: Consolidation and Long-Term Follow-Up (Weeks 6-12 and Beyond)
At the 6-week mark, a critical clinical inflection point is reached. If the patient is afebrile, clinically improving, and the inflammatory markers have normalized, the intravenous antibiotics may be discontinued. In cases involving highly virulent organisms (e.g., MRSA, Pseudomonas) or retained hardware, a prolonged course of oral suppressive antibiotic therapy may be instituted for an additional 3 to 6 months, guided by the infectious disease team. Upright plain radiographs (anteroposterior and lateral) are obtained at 6 weeks, 12 weeks, and 6 months to assess spinal alignment, hardware integrity, and the progressive incorporation of the structural graft. Routine postoperative MRI is generally contraindicated in the early phases unless there is a new, unexplained neurological deficit, as postoperative edema, surgical artifact, and normal granulation tissue can easily mimic persistent infection, leading to unnecessary diagnostic confusion.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of spinal infections is heavily guided by historical precedent and evolving clinical guidelines. A thorough understanding of the landmark literature is essential for the academic orthopedic surgeon to justify clinical decision-making and optimize patient outcomes.
The seminal work by Coventry, Ghormley, and Kernohan in 1945 established the foundational understanding of the avascular nature of the adult intervertebral disc, fundamentally shifting the paradigm of how spine surgeons conceptualize the pathogenesis of discitis. By proving that the disc relies on diffusion rather than direct vascularity, they provided the anatomical rationale for why systemic antibiotics fail to penetrate the disc space, thereby cementing the role of surgical debridement in advanced infections.
In the realm of tuberculous spondylitis, the pioneering work of Hodgson and Stock in the 1950s and 1960s revolutionized the treatment of Pott's disease. Prior to their contributions, tuberculous spine infections were managed with prolonged immobilization in plaster beds, often resulting in catastrophic kyphosis and paraplegia. Hodgson advocated for the "Hong Kong procedure," which involved radical anterior debridement of the caseous necrotic tissue and immediate structural strut grafting. This aggressive anterior approach dramatically improved neurological recovery rates and prevented severe deformity, establishing the anterior corpectomy as the gold standard for destructive spinal infections.
More recently, the Infectious Diseases Society of America (IDSA) and the North American Spine Society (NASS) have published comprehensive clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adults. These guidelines emphasize the critical importance of obtaining a definitive microbiological diagnosis prior to the initiation of empirical antibiotics, provided the patient is hemodynamically stable and neurologically intact. Furthermore, recent randomized controlled trials, such as
