Introduction and Epidemiology
Ankle pathologies represent a significant burden on healthcare systems, frequently necessitating surgical intervention. Conditions ranging from acute traumatic injuries, such as fractures and ligamentous disruptions, to chronic degenerative processes like osteoarthritis and tendinopathy, often culminate in operative management. The ankle joint, a complex articulation involving the distal tibia, fibula, and talus, bears substantial load during locomotion, making it vulnerable to a wide spectrum of injuries and degenerative changes. Epidemiologically, ankle fractures are among the most common lower extremity fractures, with incidence rates varying by age and activity level but consistently ranking high. Ankle sprains, while often managed non-operatively, can lead to chronic instability in a significant percentage of patients, prompting surgical stabilization. Similarly, advanced ankle arthritis, regardless of etiology (post-traumatic, inflammatory, primary), can severely impair quality of life, with arthrodesis or arthroplasty as definitive surgical solutions. Mastery of ankle surgical anatomy is paramount for all orthopedic surgeons, residents, and medical students contemplating surgical intervention. A precise understanding of osteology, ligamentous structures, musculotendinous units, and neurovascular pathways is not merely academic; it directly translates into surgical proficiency, minimizing iatrogenic injury, optimizing outcomes, and facilitating efficient dissection through established internervous and intermuscular planes. This comprehensive review aims to delineate the essential anatomical considerations and surgical principles required for safe and effective approaches to the ankle.
Surgical Anatomy and Biomechanics
The ankle joint, or talocrural joint, is a highly congruent hinge joint crucial for sagittal plane motion (dorsiflexion and plantarflexion). Its stability is conferred by the bony mortise formed by the distal tibia and fibula, reinforced by a robust ligamentous complex. A thorough understanding of the anatomical relationships is critical for surgical planning and execution.
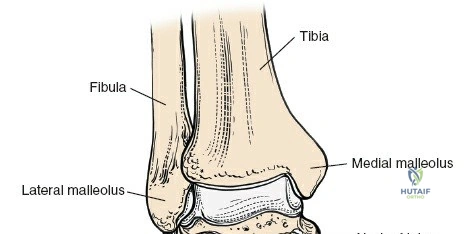
Osteology of the Ankle
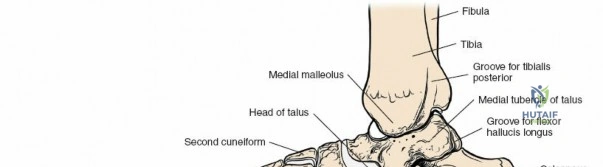
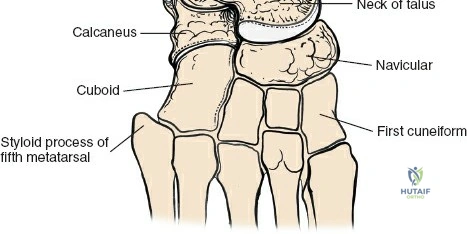
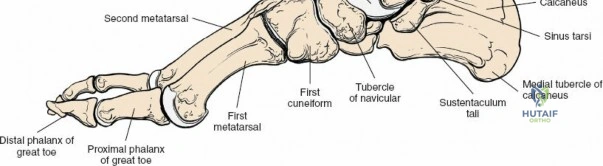
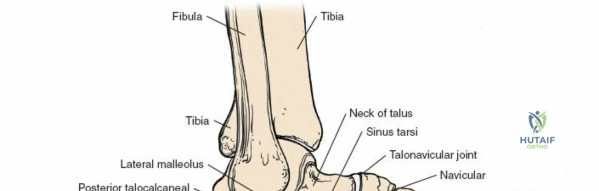
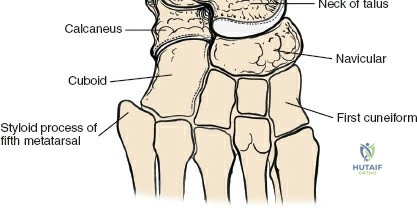
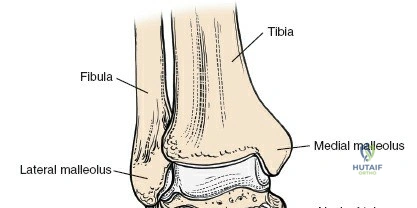
The ankle mortise consists of the distal tibia (plafond, medial malleolus), distal fibula (lateral malleolus), and the body of the talus. The tibial plafond articulates with the trochlea of the talus, allowing for primary dorsiflexion and plantarflexion. The medial and lateral malleoli provide bony buttressing and serve as critical attachment points for the collateral ligaments. The fibula plays a vital role in maintaining the integrity of the mortise; its length, rotation, and translation directly affect talar position and overall ankle stability. Subtle shifts in fibular position, even millimeters, can significantly alter tibio-talar contact areas and load distribution.
Tendons and Retinacula of the Ankle
The key structures that cross the ankle joint fall into specific groups, each encased by retinacula to prevent bowstringing and maintain mechanical advantage.
Medial Tendon Compartment
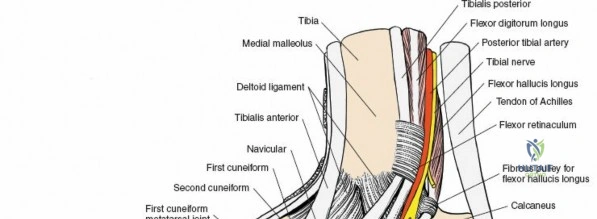
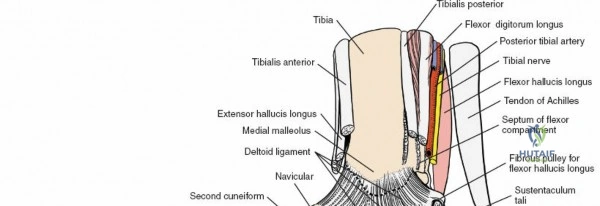
The flexor tendons, often remembered by the mnemonic "Tom, Dick, And Nervous Harry" (Tibialis Posterior, flexor Digitorum Longus, posterior tibial Artery, tibial Nerve, flexor Hallucis Longus), pass behind the medial malleolus. These tendons are supplied by the tibial nerve.
* Tibialis Posterior: Inserts primarily on the navicular tuberosity and cuneiforms. A primary invertor and plantarflexor of the foot.
* Flexor Digitorum Longus: Courses distally to insert on the plantar surfaces of the distal phalanges of the lateral four toes. Functions in toe flexion and weak plantarflexion.
* Flexor Hallucis Longus: Most posterior of the three, passes through a groove on the posterior talus and then under the sustentaculum tali before inserting on the distal phalanx of the hallux. A powerful hallux flexor and secondary plantarflexor.
These tendons are held in place by the flexor retinaculum, forming the roof of the tarsal tunnel.

Anterior Tendon Compartment
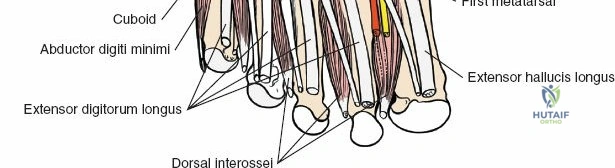
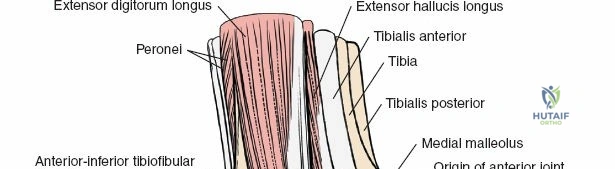
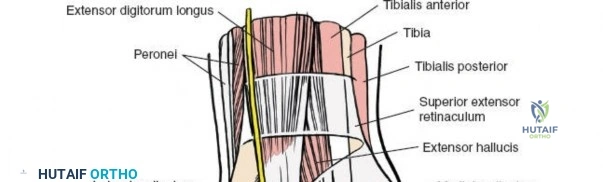
The extensor tendons pass in front of the ankle joint and are supplied by the deep peroneal nerve.
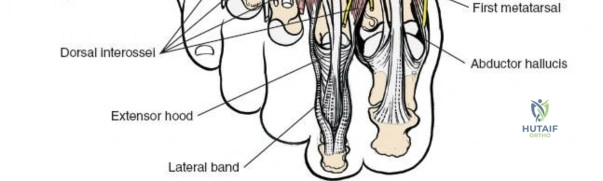
* Tibialis Anterior: Inserts on the medial cuneiform and base of the first metatarsal. Primary dorsiflexor and invertor.
* Extensor Hallucis Longus: Inserts on the dorsal aspect of the distal phalanx of the great toe. Extends the hallux and assists in dorsiflexion.
* Extensor Digitorum Longus: Divides into four slips to insert on the middle and distal phalanges of the lateral four toes. Extends the lateral four toes and assists in dorsiflexion.
* Peroneus Tertius: A small, inconsistent muscle often considered part of the EDL, inserting on the dorsal aspect of the base of the fifth metatarsal. Functions as a weak dorsiflexor and evertor.
The extensor retinaculum secures these tendons anteriorly.


Lateral Tendon Compartment
The evertor tendons pass behind the lateral malleolus and are supplied by the superficial peroneal nerve.
* Peroneus Longus: Courses inferiorly, hooks around the cuboid, and crosses the sole of the foot to insert on the medial cuneiform and base of the first metatarsal. Primary evertor and plantarflexor of the first ray.
* Peroneus Brevis: Inserts on the tuberosity of the fifth metatarsal. Primary evertor.
The peroneal retinacula (superior and inferior) prevent bowstringing of these tendons.

Posterior Tendons
- Achilles Tendon: The largest and strongest tendon in the body, formed by the gastrocnemius and soleus muscles, inserting onto the calcaneal tuberosity. Primary plantarflexor.
- Plantaris Tendon: Small, often absent, courses medial to the Achilles.
Neurovascular Bundles
Two major neurovascular bundles cross the ankle joint and supply the foot, representing critical structures to protect during any approach.
Anterior Neurovascular Bundle
The anterior neurovascular bundle crosses the front of the ankle, roughly halfway between the malleoli. It lies between the tibialis anterior and extensor hallucis longus muscles proximally, and between the tendons of the extensor hallucis longus and extensor digitorum longus muscles distally. This bundle comprises:
* Deep Peroneal Nerve: Supplies motor innervation to the anterior compartment muscles and provides sensation to the first web space.
* Anterior Tibial Artery (Dorsalis Pedis Artery distally): Provides arterial supply to the anterior leg and dorsum of the foot.
* Deep Peroneal Veins: Accompany the artery.
Injury to this bundle can result in foot drop, sensory deficits, or compromise of distal perfusion.

 (Note: Image with
(Note: Image with 17b2fb94 does not exist in the provided list, using 17b2fb95 instead, assuming a typo or similar image reference)

Posterior Neurovascular Bundle
The posterior neurovascular bundle, often referred to as the "tarsal tunnel contents," passes behind the medial malleolus, deep to the flexor retinaculum. It contains:
* Tibial Nerve: Supplies motor innervation to the posterior compartment muscles and intrinsic foot muscles, and provides sensation to the plantar aspect of the foot.
* Posterior Tibial Artery: Primary arterial supply to the plantar foot.
* Posterior Tibial Veins: Accompany the artery.
This bundle is located between the flexor digitorum longus and flexor hallucis longus tendons, with the tibial nerve being the most superficial structure within the tunnel.

Other Nerves
- Sural Nerve: Lies subcutaneously posterior to the lateral malleolus. Supplies sensation to the posterolateral leg and lateral aspect of the foot. Highly vulnerable during lateral and posterior approaches.
- Superficial Peroneal Nerve: Courses anterolaterally in the leg, becoming subcutaneous in the distal leg. Divides into medial and intermediate dorsal cutaneous nerves to supply sensation to the dorsum of the foot (excluding the first web space). Vulnerable during anterolateral approaches.
- Saphenous Nerve: Lies subcutaneously anteromedial to the medial malleolus, providing sensation to the medial leg and ankle. Vulnerable during medial approaches.
Ligamentous Structures
The ligamentous stability of the ankle is critical.
Medial Ligamentous Complex (Deltoid Ligament)
A strong, fan-shaped ligament originating from the medial malleolus. It consists of superficial and deep components:
* Superficial Layer: Tibionavicular, tibiocalcaneal, superficial posterior tibiotalar. Prevents excessive eversion and limits abduction.
* Deep Layer: Anterior tibiotalar and posterior tibiotalar. More isometric and stronger, providing primary restraint to talar external rotation and lateral displacement.

Lateral Ligamentous Complex
Consists of three distinct ligaments originating from the lateral malleolus:
* Anterior Talofibular Ligament (ATFL): Weakest of the three, runs from the anterior aspect of the lateral malleolus to the talar neck. Primary restraint to anterior drawer and internal rotation of the talus. Most commonly injured ligament in ankle sprains.
* Calcaneofibular Ligament (CFL): Courses from the tip of the lateral malleolus to the lateral aspect of the calcaneus. Resists inversion.
* Posterior Talofibular Ligament (PTFL): Strongest of the three, runs horizontally from the posterior aspect of the lateral malleolus to the posterior process of the talus. Provides posterior stability and resists extreme dorsiflexion.

Syndesmotic Ligaments
These ligaments bind the distal tibia and fibula, maintaining the integrity of the ankle mortise.
* Anterior Inferior Tibiofibular Ligament (AITFL): Connects the anterior distal tibia to the fibula.
* Posterior Inferior Tibiofibular Ligament (PITFL): Connects the posterior distal tibia to the fibula.
* Interosseous Ligament: A continuation of the interosseous membrane, providing significant stability.
* Inferior Transverse Ligament: A deep portion of the PITFL.
Disruption of the syndesmosis (high ankle sprain or fracture-dislocation) leads to widening of the ankle mortise, instability, and requires surgical reduction and fixation.
Internervous Planes
The different nerve supplies of the tendon groups offer distinct internervous planes, which are surgically advantageous as they allow dissection without directly incising muscle bellies or transecting major nerves.
* Medial Approach: Between the flexors (tibialis posterior, supplied by tibial nerve) and extensors (tibialis anterior, supplied by deep peroneal nerve). This plane is more accurately described as an interval between the tibialis anterior and saphenous vein/nerve anteriorly, and the tibialis posterior and posterior tibial neurovascular bundle posteriorly.
* Posterolateral Approach: Between the flexors (flexor hallucis longus, supplied by tibial nerve) and evertors (peroneus brevis, supplied by superficial peroneal nerve).
* Lateral Approach: Between extensors (peroneus tertius/EDL, supplied by deep peroneal nerve) and evertors (peroneus brevis/longus, supplied by superficial peroneal nerve). This involves splitting the peroneal muscles or retracting them.
* Anteromedial Approach: Between the tibialis anterior (deep peroneal nerve) and the saphenous nerve and vein.
* Anterolateral Approach: Between the extensor digitorum longus (deep peroneal nerve) and the peroneus tertius/brevis (superficial peroneal nerve).
Understanding these planes minimizes muscle damage, reduces bleeding, and preserves nerve and vascular structures, leading to less postoperative pain and faster recovery.
Indications and Contraindications
Surgical intervention for ankle pathologies is considered when conservative management fails, or when the nature of the injury necessitates operative stabilization to restore anatomical alignment and function.
Indications for Ankle Surgery
The indications for ankle surgery are broad, encompassing acute trauma, chronic instability, degenerative conditions, and complex deformities.
Acute Traumatic Injuries
- Ankle Fractures: Unstable ankle fractures (e.g., bimalleolar, trimalleolar, syndesmotic disruption, displaced unimalleolar fractures), open fractures, pilon fractures, and talar fractures with displacement.
- Ligamentous Injuries: Chronic ankle instability following failed non-operative management of lateral ligament ruptures; syndesmotic injuries (diastasis).
- Tendon Ruptures: Acute Achilles tendon rupture, tibialis posterior tendon rupture, peroneal tendon ruptures.
Chronic Conditions
- Ankle Arthritis: End-stage osteoarthritis (post-traumatic, inflammatory, primary) refractory to conservative treatment, requiring arthrodesis or total ankle arthroplasty.
- Ankle Instability: Persistent symptomatic instability after non-operative management, often necessitating ligament reconstruction or repair.
- Tendon Pathologies: Chronic tendinopathy with recalcitrant symptoms (e.g., Achilles tendinopathy, peroneal tendinopathy) requiring debridement, repair, or reconstruction.
- Deformity Correction: Correction of hindfoot malalignment, cavovarus, or planovalgus deformities that compromise ankle mechanics.
- Osteochondral Lesions of the Talus (OLT): Symptomatic OLTs that have failed non-operative management, often requiring débridement, microfracture, osteochondral autograft transplantation (OAT), or allograft.
- Nerve Entrapment: Tarsal tunnel syndrome refractory to conservative measures.
Contraindications for Ankle Surgery
Contraindications can be absolute or relative, depending on the patient's overall health, local tissue conditions, and the specific pathology.
Absolute Contraindications
- Active Infection: Osteomyelitis or active cellulitis at the surgical site.
- Severe Peripheral Vascular Disease: Compromised vascularity that precludes adequate wound healing.
- Uncontrolled Systemic Sepsis: Patient too unstable for anesthesia and surgery.
- Extensive Soft Tissue Compromise: Irreparable skin or soft tissue loss making wound closure impossible or highly prone to failure.
Relative Contraindications
- Poorly Controlled Comorbidities: Uncontrolled diabetes, severe peripheral neuropathy, significant cardiovascular or pulmonary disease, chronic kidney disease, severe malnutrition. These factors increase surgical risk and complication rates.
- Smoking/Nicotine Use: Significantly impairs wound healing and increases risk of infection and nonunion. Cessation is strongly advised preoperatively.
- Patient Non-Compliance: Inability or unwillingness to adhere to postoperative protocols.
- Local Skin Conditions: Severe dermatological conditions, fragile skin, or prior radiation in the surgical field.
- Advanced Osteoporosis: Compromised bone quality may limit fixation strength, although not a strict contraindication for all procedures.
- Severe Edema or Blistering: Requires delay until soft tissue envelope is optimized.
Operative vs Non-Operative Indications
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Ankle Fractures | Displaced/unstable unimalleolar, bimalleolar, trimalleolar, syndesmotic disruption, pilon, open fractures, displaced talar fractures. | Stable unimalleolar (e.g., non-displaced lateral malleolus), stress fractures, selected avulsion fractures. |
| Ankle Ligamentous Injury | Chronic lateral ankle instability unresponsive to rehab, syndesmotic injury with diastasis, acute deltoid rupture with instability. | Acute lateral ankle sprains (Grade I-III) with bracing/rehabilitation, stable medial sprains. |
| Ankle Arthritis | End-stage symptomatic arthritis refractory to conservative care (arthrodesis, arthroplasty). | Early to moderate arthritis with NSAIDs, activity modification, bracing, injections, physical therapy. |
| Tendon Pathology | Acute Achilles tendon rupture, chronic tibialis posterior insufficiency with deformity, recalcitrant peroneal tendinopathy/rupture. | Acute tendinitis/tendinosis (RICE, NSAIDs, PT, orthotics), partial Achilles tears (casting/boot). |
| Osteochondral Lesions | Symptomatic lesions >1 cm², deep lesions, failed conservative treatment. | Small (<1 cm²) asymptomatic or minimally symptomatic lesions, initial conservative management. |
| Nerve Entrapment | Tarsal tunnel syndrome unresponsive to conservative therapy. | Mild tarsal tunnel symptoms, activity modification, orthotics, injections. |
| Deformity Correction | Significant hindfoot malalignment causing pain/dysfunction and affecting gait mechanics. | Minor deformities, asymptomatic deformities, early stage flexible deformities with orthotics. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is fundamental to achieving successful surgical outcomes in ankle surgery. This involves detailed patient assessment, meticulous imaging review, strategic selection of the surgical approach, and precise intraoperative patient positioning.
Patient Assessment and Medical Optimization
A comprehensive medical history, physical examination, and review of comorbidities are essential. Optimization of systemic conditions (e.g., glycemic control in diabetics, nutritional status, smoking cessation) is critical to minimize perioperative risks. Assessment of the soft tissue envelope, including swelling, blistering, and skin integrity, dictates the timing of surgery, especially in acute trauma. A period of elevation, ice, and compression may be required to allow the soft tissues to recover, often referred to as "waiting for the wrinkle sign."
Imaging Review
High-quality imaging is indispensable.
* Plain Radiographs: Anteroposterior, lateral, and mortise views of the ankle are standard. Weight-bearing views are crucial for assessing joint space narrowing and alignment in degenerative conditions. Specific views such as Broden's or Canale's may be required for talar injuries.
* Computed Tomography (CT): Essential for complex fractures (pilon, talar), assessing articular step-off, comminution, and fragment displacement. It also aids in identifying syndesmotic pathology and osteochondral lesions. 3D reconstructions are particularly helpful for visualizing complex fracture patterns and planning hardware placement.
* Magnetic Resonance Imaging (MRI): Primarily used for evaluating soft tissue injuries, including ligament ruptures (e.g., ATFL, CFL, deltoid), tendon pathologies (e.g., Achilles, tibialis posterior, peroneal), nerve impingement, and detailed characterization of osteochondral lesions.
* Angiography: In cases of suspected vascular compromise or severe peripheral vascular disease, arteriography may be indicated to map vascular supply.
Surgical Approach Selection
The choice of surgical approach is dictated by the specific pathology, its location, and the need for optimal exposure while minimizing iatrogenic injury. Consideration of internervous planes, neurovascular bundle locations, and soft tissue health are paramount.
* Medial Approach: For medial malleolus fractures, deltoid ligament repair, subtalar arthrodesis.
* Lateral Approach: For lateral malleolus fractures, peroneal tendon pathologies, lateral ligament repair/reconstruction.
* Anterior Approach: For anterior ankle arthroscopy, anterior impingement, OLTs, total ankle arthroplasty.
* Anteromedial Approach: For medial malleolus fixation, anterior tibiotalar exostectomy, deltoid ligament work.
* Anterolateral Approach: For fibular fracture fixation, lateral ligament repair, osteochondral lesion access.
* Posterior Approach (Posteromedial/Posterolateral): For posterior malleolus fractures, Achilles repair, FHL transfer, posterior ankle arthroscopy, posterior ankle fusion, osteoid osteoma excision.
Patient Positioning and Preparation
Proper positioning is critical for optimal exposure, surgeon comfort, and prevention of iatrogenic injury.
* Supine Position: Most common for anterior, medial, and lateral approaches. A bump under the ipsilateral hip may be used to internally rotate the limb for better lateral access. A radiolucent table is often required for intraoperative fluoroscopy.
* Lateral Decubitus Position: Useful for posterolateral approaches to the ankle and hindfoot, allowing good access to the posterior aspect of the fibula and tibia.
* Prone Position: Indicated for direct posterior approaches, such as Achilles tendon repair or posterior ankle arthroscopy. A tourniquet is typically applied to the proximal thigh, and a thigh holder or well-padded leg rest is used to elevate the limb.
* Regional Anesthesia: A popliteal nerve block or spinal anesthesia is often used in conjunction with general anesthesia to provide excellent postoperative analgesia.
* Sterile Prep and Drape: Standard sterile preparation extends from the mid-calf to the toes. A clear plastic adhesive drape may be applied after prepping to isolate the operative field and protect sterile drapes.
* Fluoroscopy: Readily available and draped for sterile use to confirm reduction and hardware placement.
Detailed Surgical Approach and Technique
A detailed understanding of specific surgical approaches is crucial for safe and effective ankle surgery. Each approach offers advantages for accessing particular anatomical regions while minimizing damage to critical structures. The following section outlines common approaches, emphasizing anatomical landmarks, internervous planes, and general principles of dissection, reduction, and fixation.
Anteromedial Approach to the Ankle
This approach provides access to the medial aspect of the talocrural joint, medial malleolus, and structures of the medial gutter.
* Indications: Medial malleolus fractures, deltoid ligament repair, medial osteochondral lesions, anterior tibiotalar impingement, medial arthrodesis.
* Patient Positioning: Supine with a bolster under the ipsilateral hip for slight external rotation.
* Incision: A longitudinal incision centered over the medial malleolus, extending proximally along the anterior border of the tibia and distally towards the navicular.
* Dissection:
* Skin and Subcutaneous Tissue: Carefully incise, identify and protect the saphenous vein and nerve, which run anteromedial to the medial malleolus. The saphenous nerve provides sensation to the medial aspect of the foot and ankle.
* Deep Fascia: Incise the deep fascia.
* Internervous Plane: The interval is typically between the tibialis anterior tendon (anteriorly, innervated by deep peroneal nerve) and the tibialis posterior tendon (posteriorly, innervated by tibial nerve). However, for direct access to the medial malleolus, the dissection proceeds deep to the tibialis anterior tendon, but superficial to the neurovascular bundle of the tarsal tunnel.
* Exposure: Retract the tibialis anterior tendon anteriorly. The medial capsule of the ankle joint and the medial malleolus are now exposed. The deltoid ligament origin is visualized.
* Protection: Continually protect the saphenous neurovascular structures and avoid excessive retraction on the posterior tibial neurovascular bundle in the tarsal tunnel.
Anterolateral Approach to the Ankle
This approach is versatile, offering access to the lateral aspect of the ankle joint, distal fibula, and anterior syndesmosis.
* Indications: Lateral malleolus fractures, syndesmotic injury (AITFL repair/debridement), lateral ankle ligament repair/reconstruction (ATFL, CFL), osteochondral lesions of the lateral talus, anterior ankle arthroscopy portals.
* Patient Positioning: Supine with a bolster under the ipsilateral hip for slight internal rotation.
* Incision: A longitudinal incision centered over the distal fibula, extending proximally along the fibular shaft and distally towards the base of the fifth metatarsal.
* Dissection:
* Skin and Subcutaneous Tissue: Careful incision to identify and protect branches of the superficial peroneal nerve. These nerves are highly variable and vulnerable; blunt dissection or precise identification and retraction are crucial. The sural nerve lies more posterior.
* Deep Fascia: Incise the deep fascia along the fibular shaft.
* Internervous Plane: The interval is between the extensor digitorum longus (and peroneus tertius, supplied by deep peroneal nerve) anteriorly and the peroneal tendons (peroneus brevis and longus, supplied by superficial peroneal nerve) posteriorly. The deep peroneal nerve and anterior tibial artery run more medially.
* Exposure: Retract the extensor digitorum longus and peroneus tertius anteriorly. Retract the peroneal tendons posteriorly. This exposes the anterior surface of the distal fibula, the anterior syndesmosis (AITFL), and the lateral ankle capsule. The ATFL and CFL can be visualized.
* Protection: Meticulous protection of the superficial peroneal nerve branches is paramount to prevent postoperative dysesthesias.
Direct Lateral Approach to the Fibula
Primarily used for fixation of lateral malleolus fractures.
* Indications: Lateral malleolus fractures (Weber B, C).
* Patient Positioning: Supine with internal rotation of the limb.
* Incision: Longitudinal incision directly over the lateral malleolus, curving slightly anteriorly or posteriorly depending on the fracture pattern and hardware requirements.
* Dissection:
* Skin and Subcutaneous Tissue: Identify and protect the sural nerve (posteriorly) and superficial peroneal nerve branches (anteriorly).
* Deep Fascia: Incise the deep fascia over the fibula.
* Exposure: Subperiosteal dissection exposes the lateral malleolus. The peroneal tendons are typically retracted posteriorly or anteriorly as needed, depending on the fracture and extent of exposure required.

* Syndesmotic Assessment: After fracture fixation, the stability of the syndesmosis is assessed. If unstable, syndesmotic fixation (e.g., screw or suture button) is performed.

 (Note: Image with
(Note: Image with 0e0f0683a does not exist in the provided list, using 0e0d02f0683a instead, assuming a typo or similar image reference)

Anterior Approach to the Ankle (Extensile)
This approach provides broad access to the anterior aspect of the ankle joint and tibiotalar articulation.
* Indications: Total ankle arthroplasty, severe anterior impingement, large osteochondral lesions, anterior ankle arthrodesis, pilon fracture reconstruction.
* Patient Positioning: Supine.
* Incision: A longitudinal incision, typically 8-12 cm, centered over the anterior aspect of the ankle joint, midway between the malleoli.

* Dissection:
* Skin and Subcutaneous Tissue: Careful dissection to avoid injury to the superficial peroneal nerve branches (lateral) and saphenous nerve (medial).
* Deep Fascia/Extensor Retinaculum: Incise the deep fascia. The anterior neurovascular bundle (deep peroneal nerve and anterior tibial artery) lies between the tibialis anterior and extensor hallucis longus tendons proximally, and between the extensor hallucis longus and extensor digitorum longus tendons distally.
* Internervous Plane: The approach utilizes the interval between the tibialis anterior tendon (medially) and the extensor hallucis longus tendon (laterally).
* Exposure: Retract the tibialis anterior tendon medially, and the extensor hallucis longus, extensor digitorum longus, and anterior neurovascular bundle laterally. The ankle capsule and anterior tibia and talus are exposed.


* Protection: Meticulous care to protect the anterior neurovascular bundle and superficial peroneal nerve branches. Subperiosteal dissection is often used on the tibia and talus.
Posteromedial Approach to the Ankle
This approach provides access to the posterior aspect of the medial malleolus, posterior subtalar joint, and the structures of the tarsal tunnel.
* Indications: Posterior malleolus fractures (medial fragment), flexor hallucis longus pathology, tarsal tunnel release, posterior ankle arthrodesis, transfer of tibialis posterior.
* Patient Positioning: Prone or lateral decubitus.
* Incision: Longitudinal incision 1-2 cm posterior to the medial malleolus, curving slightly anteriorly distally.
* Dissection:
* Skin and Subcutaneous Tissue: Carefully incise. The lesser saphenous vein (if present) and medial calcaneal nerve branches may be encountered.
* Deep Fascia: Incise the deep fascia.
* Exposure: The flexor retinaculum is identified. The posterior tibial neurovascular bundle (tibial nerve, posterior tibial artery and veins) lies deep to this retinaculum, between the flexor digitorum longus and flexor hallucis longus tendons. The tibialis posterior tendon is the most anterior of the deep compartment tendons.
* Protection: The posterior tibial neurovascular bundle is the primary concern. It must be identified and carefully protected, often retracted anteriorly or posteriorly depending on the target anatomy.
Posterolateral Approach to the Ankle (Trimalleolar Fractures, Pilon Fractures, Posterior Ankle Arthroscopy)
This approach offers access to the posterior aspect of the fibula, posterior malleolus, and posterior ankle capsule. It is particularly useful for reducing and fixing posterior malleolus fragments in trimalleolar fractures or pilon fractures.
* Indications: Posterior malleolus fractures, posterior ankle arthroscopy, posterior ankle fusion, peroneal tendon repair.
* Patient Positioning: Prone or lateral decubitus.
* Incision: A longitudinal incision along the posterior border of the fibula, extending proximally along the Achilles tendon and distally along the lateral aspect of the calcaneus.
* Dissection:
* Skin and Subcutaneous Tissue: Identify and protect the sural nerve, which is superficial and courses along the posterior border of the fibula.
* Deep Fascia: Incise the deep fascia.
* Internervous Plane: The interval is typically between the peroneal tendons (lateral, supplied by superficial peroneal nerve) and the flexor hallucis longus tendon (medial, supplied by tibial nerve).
* Exposure: Retract the peroneal tendons anteriorly. Retract the Achilles tendon and flexor hallucis longus posteriorly/medially. This exposes the posterior aspect of the distal fibula, the posterior syndesmotic ligaments (PITFL), and the posterior malleolus.
* Protection: Meticulous protection of the sural nerve. The posterior tibial neurovascular bundle is located more medially and anteriorly in relation to the FHL and generally not directly in the field unless dissection is extended medially.
Reduction and Fixation Principles
Regardless of the approach, the principles of reduction and internal fixation remain consistent:
1. Anatomical Reduction: Restore articular congruity and overall alignment. Direct visualization and fluoroscopic guidance are crucial.
2. Stable Fixation: Provide rigid internal fixation to allow for early motion and rehabilitation. Implants include screws (cortical, cancellous, lag), plates (locking, non-locking, antiglide, neutralization), and syndesmotic screws or suture buttons.
3. Soft Tissue Preservation: Minimize soft tissue stripping to maintain vascularity and reduce wound complications.
4. Neurovascular Protection: Constant vigilance to identify and protect all nerves and vessels.
5. Biomechanical Considerations: Ensure fixation addresses specific fracture patterns and biomechanical forces. For example, in ankle fractures, restoring fibular length, rotation, and translation is paramount for mortise stability.
Specific Fixation Examples
- Lateral Malleolus: Typically fixed with a one-third tubular plate (neutralization or antiglide) or a pre-contoured locking plate. Lag screws are often used for interfragmentary compression.

- Medial Malleolus: Can be fixed with two cancellous lag screws, K-wires, or a tension band wire construct.
- Posterior Malleolus: Direct anterior-to-posterior screws (posterior to anterior if approached posteriorly) or small fragment plate fixation.
- Syndesmosis: Assessed intraoperatively; if unstable, fixed with one or two tricortical screws (typically 3.5mm or 4.0mm) or a suture button device. The foot should be positioned in dorsiflexion during fixation to prevent overtightening.
 (Note: Image with
(Note: Image with f3e7877b7does not exist in the provided list, usingf3eb563f-4143-4e4d-b55e-d0dfa55281ea.jpgand75c1a608-abc5-4a29-84f5-b42e883d8e05.jpgas general fixation examples for context)





Complications and Management
Despite meticulous surgical technique and comprehensive preoperative planning, complications can arise following ankle surgery. These can be broadly categorized into general surgical complications and those specific to the ankle and foot. Proactive management and a thorough understanding of potential pitfalls are crucial.
General Surgical Complications
- Infection: Superficial or deep surgical site infection. Incidence varies from 1-5% but can be significantly higher in open fractures, pilon fractures, or patients with comorbidities. Management includes antibiotics, irrigation and debridement, and potentially hardware removal.
- Wound Healing Issues: Dehiscence, necrosis, skin blistering. More common in patients with diabetes, peripheral vascular disease, smokers, or in cases with significant soft tissue injury. Requires meticulous soft tissue handling, delayed closure if necessary, local wound care, or reconstructive procedures (e.g., skin grafts, flaps).
- Thromboembolic Events: Deep vein thrombosis (DVT) and pulmonary embolism (PE). Prophylaxis (mechanical, pharmacological) is standard, especially in higher-risk patients or prolonged immobilization.
- Nerve Injury: Transient neuropraxia or permanent damage. Can be due to direct trauma, traction, or compression. Most commonly involves the superficial peroneal, sural, or saphenous nerves around the ankle. Management ranges from observation to neurolysis or nerve grafting.
- Vascular Injury: Rare but severe, particularly to the anterior or posterior tibial arteries. Requires immediate vascular consultation and repair.
Ankle-Specific Complications
- Nonunion or Malunion: Failure of bone healing or healing in an unacceptable anatomical position.
- Nonunion: Occurs in 5-10% of ankle fractures, higher in open fractures or pilon fractures. May require revision surgery with bone grafting, stable fixation, and possibly biological adjuncts.
- Malunion: Can lead to altered ankle biomechanics, pain, and accelerated arthritis. May necessitate corrective osteotomies.
- Post-Traumatic Arthritis: A common sequela, particularly after intra-articular fractures (pilon, talar). Severity correlates with articular incongruity. Managed with conservative measures initially, but often progresses to arthrodesis or total ankle arthroplasty.
- Hardware Complications: Prominent hardware requiring removal (common with lateral malleolus plates/screws), screw breakage, loss of fixation.
- Stiffness/Arthrofibrosis: Restricted range of motion due to capsular scarring or heterotopic ossification. Managed with aggressive physical therapy, dynamic splinting, or arthroscopic/open arthrolysis.
- Chronic Pain: Multifactorial, can be due to nerve injury, residual instability, arthritis, or psychosocial factors.
- Complex Regional Pain Syndrome (CRPS): A challenging condition characterized by disproportionate pain, swelling, and autonomic dysfunction. Early diagnosis and multidisciplinary management are crucial.
- Syndesmotic Overtightening: Can cause pain, loss of dorsiflexion, and accelerated arthritis. Requires removal of syndesmotic screws, sometimes with re-reduction.
Complications and Management Table
| Complication | Incidence (Approx.) | Salvage/Management Strategies |
|---|---|---|
| Surgical Site Infection | 1-5% (higher in open fractures) | Local wound care, IV antibiotics (culture-directed), surgical irrigation and debridement, hardware removal (if infected and fracture stable), flap coverage for severe cases. |
| Wound Dehiscence/Necrosis | 2-10% | Conservative wound care, debridement of necrotic tissue, secondary closure, skin grafting, local or free flap reconstruction. Optimize patient comorbidities (e.g., smoking cessation, glycemic control). |
| Nerve Injury | 5-15% (sensory branches) | Observation for neuropraxia (most resolve), neurolysis, nerve grafting, tendon transfer for motor deficits. Patient education regarding dysesthesia. |
| Nonunion | 5-10% | Revision internal fixation with stable construct, bone grafting (autograft, allograft, DBM), electrical stimulation, biological adjuncts (e.g., PRP, BMP). |
| Malunion | Varies, dependent on fracture | Corrective osteotomy (supramalleolar, calcaneal, subtalar) to restore alignment and joint congruity; potentially arthrodesis or arthroplasty if severe degenerative changes. |
| Post-Traumatic Arthritis | 10-50% (intra-articular) | Conservative management (NSAIDs, injections, bracing, PT), arthroscopic debridement, osteotomies, eventually arthrodesis (fusion) or total ankle arthroplasty. |
| Hardware Prominence/Pain | 10-30% | Hardware removal after fracture healing (typically 6-12 months post-op). |
| Ankle Stiffness | 10-20% | Aggressive physical therapy, dynamic splinting, manipulation under anesthesia, arthroscopic or open arthrolysis for severe cases of arthrofibrosis or heterotopic ossification. |
| Complex Regional Pain Syndrome (CRPS) | <5% | Early diagnosis, multimodal pain management (medications, nerve blocks), physical therapy, psychological support. Referral to pain specialist. |
| Syndesmotic Overtightening | 1-5% | Removal of syndesmotic screw, re-assessment of syndesmotic stability, re-fixation (if unstable) in appropriate dorsiflexion. May require extensive rehabilitation for dorsiflexion recovery. |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is an integral component of successful ankle surgery, aiming to restore range of motion, strength, proprioception, and functional mobility while protecting the surgical repair or reconstruction. Protocols vary significantly based on the specific procedure, fracture stability, bone quality, patient comorbidities, and surgeon preference. The general principles involve phased progression, guided by tissue healing timelines.
General Principles
- Protection Phase (Weeks 0-6): Focus on protecting the surgical site, controlling pain and swelling, and maintaining mobility of adjacent joints. Weight-bearing status is typically restricted (non-weight bearing, touch-down weight bearing) to allow initial bone and soft tissue healing. Immobilization in a splint, cast, or CAM boot is common. Gentle range of motion (ROM) exercises may be initiated for the ankle within protected limits, or for the knee/hip.
- Controlled Motion Phase (Weeks 6-12): Gradual increase in weight-bearing as tolerated and directed by imaging and surgeon assessment. Progressive ankle ROM exercises are introduced, often transitioning from passive to active-assisted to active. Gentle strengthening exercises (isometrics, theraband) are initiated. Scar mobilization techniques are important.
- Strengthening and Proprioception Phase (Weeks 12-24): Focus on restoring full muscle strength, endurance, and proprioception. Full weight-bearing is typically achieved. Advanced strengthening exercises (calf raises, heel-toe raises, balance exercises on unstable surfaces) are incorporated. Agility drills and sports-specific training are introduced for athletic populations.
- Return to Activity/Sport Phase (Months 6+): Gradual return to desired activities and sports, contingent on achieving specific functional milestones (e.g., symmetrical strength, full pain-free ROM, dynamic stability, performance on functional tests). Continued home exercise program.
Examples of Specific Rehabilitation Protocols
Ankle Fracture Open Reduction Internal Fixation (ORIF)
- Weeks 0-2: Posterior splint/cast, NWB. Elevation, ice, gentle toe ROM.
- Weeks 2-6: Transition to CAM boot, NWB or TDWB. Begin gentle ankle dorsiflexion/plantarflexion ROM (non-weight bearing).
- Weeks 6-12: Progressive weight-bearing in CAM boot, weaning off boot as tolerated and stable. Initiate active ankle ROM, gentle strengthening (theraband).
- Weeks 12-24: Full weight-bearing. Progress to advanced strengthening, balance, and proprioception exercises. Gait training.
- Months 6+: Return to full activities/sport as tolerated.
Lateral Ankle Ligament Reconstruction/Repair
- Weeks 0-2: Splint/cast in neutral or slight dorsiflexion, NWB.
- Weeks 2-6: CAM boot, NWB or TDWB. Gentle active dorsiflexion/plantarflexion, eversion (avoid inversion).
- Weeks 6-12: Progressive weight-bearing, transition out of boot. Full ROM for dorsiflexion/plantarflexion, eversion. Begin light strengthening (eversion, dorsiflexion).
- Weeks 12-24: Full return to strengthening, proprioception, balance training. Progressive agility drills.
- Months 6+: Return to sport-specific training. Bracing may be recommended for high-risk activities.
Total Ankle Arthroplasty (TAA)
- Weeks 0-2: Splint/cast, NWB. Emphasis on elevation and pain control.
- Weeks 2-6: CAM boot, TDWB or partial weight-bearing. Gentle active ROM for dorsiflexion/plantarflexion within limits (often aiming for 0-20 degrees).
- Weeks 6-12: Progressive weight-bearing in boot. Wean from boot to supportive shoe. Continue progressive ROM, light strengthening.
- Weeks 12-24: Full weight-bearing, progress strengthening and balance. Emphasize low-impact activities.
- Months 6+: Continue home exercise program. Avoid high-impact activities.
Key Considerations
- Patient Education: Crucial for adherence to protocols and realistic expectations.
- Pain Management: Adequate pain control facilitates participation in therapy.
- Edema Control: Continued elevation, compression, and cryotherapy are vital to prevent stiffness and improve healing.
- Scar Management: Massage and desensitization help improve soft tissue mobility and reduce adhesions.
- Functional Progression: Rehabilitation should be goal-oriented, progressing from isolated movements to complex functional activities.
- Individualization: Protocols serve as guidelines; adjustments based on patient response, comorbidities, and intraoperative findings are often necessary.
Summary of Key Literature and Guidelines
The field of ankle surgery is dynamic, with ongoing research refining surgical techniques, implant design, and rehabilitation protocols. A critical understanding of evidence-based literature and established guidelines is essential for optimal patient care.
Ankle Fractures
- Weber Classification: Historically, the Lauge-Hansen classification system was used, but the simpler Danis-Weber classification (A, B, C based on fibula fracture level relative to the syndesmosis) is now more commonly used to guide treatment decisions.
- Syndesmotic Injury: The importance of stable syndesmotic fixation is well-established. Studies (e.g., those by Lauge-Hansen) emphasize the biomechanical consequences of syndesmotic disruption. More recent literature debates the optimal fixation method (screw vs. suture button) and the number/size of screws, with growing evidence supporting suture button devices for their dynamic fixation properties and reduced need for hardware removal.
- Posterior Malleolus Fractures: Historically often ignored, current consensus emphasizes reduction and fixation of displaced posterior malleolus fragments, especially those involving >25-30% of the articular surface or causing syndesmotic instability, to prevent post-traumatic arthritis and maintain mortise stability.
Ankle Arthritis
- Arthrodesis vs. Total Ankle Arthroplasty (TAA): The choice between fusion and replacement for end-stage ankle arthritis remains a topic of extensive research and clinical discussion. Meta-analyses and long-term follow-up studies show good pain relief and functional outcomes with both, but TAA offers preservation of motion, albeit with a higher revision rate. Modern TAA designs show improved survivorship.
- Patient Selection: Careful patient selection is crucial for TAA, favoring older, less active patients with lower body mass index, intact subtalar motion, and minimal deformity.
Ankle Instability
- Anatomical vs. Non-anatomical Repair: Anatomical repair techniques (e.g., Broström-Gould procedure) are considered the gold standard for chronic lateral ankle instability, emphasizing direct repair of the ATFL and CFL with augmentation of the inferior extensor retinaculum. Non-anatomical repairs (e.g., Watson-Jones, Chrisman-Snook) are typically reserved for cases of poor tissue quality or revision surgery.
- Concomitant Pathology: The importance of identifying and addressing concomitant pathologies (e.g., peroneal tendon tears, osteochondral lesions) during instability surgery is increasingly recognized.
Osteochondral Lesions of the Talus (OLT)
- Treatment Algorithms: Algorithms for OLTs typically stratify treatment based on lesion size, depth, and patient symptoms. Initial management is often non-operative (rest, immobilization). Surgical options include arthroscopic debridement and microfracture for smaller lesions, and osteochondral autograft transplantation (OATS) or allograft for larger, cystic, or failed microfracture lesions.
- Biologic Augmentation: Research continues into the use of biological adjuncts (e.g., PRP, bone marrow aspirate concentrate) to enhance cartilage repair.
Pilon Fractures
- Staged Management: The principles of staged management (external fixation followed by definitive ORIF once soft tissues allow) are well-established to minimize wound complications.
- Surgical Approaches: Multiple approaches (anterior, anteromedial, anterolateral, posterolateral) are used, often in combination, to achieve anatomical reduction of the articular surface and stable fixation. The concept of "fracture specific" approaches is gaining traction, with a posterior approach gaining popularity for certain fracture patterns.
General Guidelines
- Multidisciplinary Approach: Complex ankle pathologies often benefit from a multidisciplinary team involving orthopedic surgeons, physical therapists, pain management specialists, and vascular surgeons.
- Evidence-Based Practice: Surgeons should stay abreast of the latest evidence, participate in continuous medical education, and critically evaluate new technologies and techniques.
- Patient-Reported Outcomes: The increasing emphasis on patient-reported outcome measures (PROMs) allows for a more comprehensive assessment of surgical success beyond radiographic healing.
This comprehensive overview underscores that successful ankle surgery hinges on a profound anatomical understanding, judicious surgical planning, meticulous technique, and tailored postoperative care, all guided by the continually evolving body of scientific literature.
Clinical & Radiographic Imaging