Anterograde Femoral Nailing: A Masterclass in Diaphyseal Fracture Fixation
Key Takeaway
Step into the operating theater for an in-depth masterclass on anterograde intramedullary nailing of femoral shaft fractures. This guide covers comprehensive anatomy, meticulous preoperative planning, real-time intraoperative execution, and critical pearls to navigate challenges. We'll detail patient positioning, entry point selection, fracture reduction techniques, reaming, nail insertion, and locking, ensuring a thorough understanding of this essential orthopedic procedure.
Comprehensive Introduction and Patho-Epidemiology
The management of femoral shaft fractures has evolved dramatically over the past century, transitioning from prolonged periods of skeletal traction associated with devastating morbidity to the elegant, biomechanically superior technique of intramedullary (IM) nailing. A femoral shaft fracture is strictly defined as an injury to the femoral diaphysis, extending from approximately 5 cm distal to the lesser trochanter to within 6 to 8 cm of the distal femoral articular surface. Recognizing the precise anatomical boundaries of the diaphysis is critical, as fractures extending into the subtrochanteric or supracondylar regions possess a distinctly different "personality" and biomechanical environment, often requiring specialized implants or alternative fixation strategies. The anterograde intramedullary nail remains the undisputed workhorse for diaphyseal injuries, providing load-sharing stability that promotes robust secondary bone healing.

Femoral shaft fractures exhibit a classic bimodal epidemiological distribution. In the younger demographic, these injuries are overwhelmingly the result of high-energy trauma, such as motor vehicle collisions, motorcycle crashes, and falls from significant heights. The sheer kinetic energy required to fracture the adult femoral diaphysis is immense; consequently, an isolated femoral shaft fracture carries an Abbreviated Injury Scale (AIS) score of 3, yielding an isolated Injury Severity Score (ISS) of 9. This high-energy transfer dictates that the orthopedic surgeon must maintain a high index of suspicion for concomitant, life-threatening injuries, strictly adhering to Advanced Trauma Life Support (ATLS) protocols. Conversely, in the elderly population, the mechanism is often a low-energy ground-level fall superimposed on osteoporotic bone. In these patients, the medullary canal is frequently widened, and the cortices are thinned, fundamentally altering the biomechanics of nail fit and stability.

The systemic physiological response to a major long bone fracture cannot be overstated. The release of inflammatory mediators, marrow fat, and cytokines into the systemic circulation precipitates a Systemic Inflammatory Response Syndrome (SIRS). In the polytraumatized patient, the "second hit" of definitive intramedullary nailing—which involves reaming and further marrow embolization—can overwhelm the patient's physiological reserves, potentially leading to Acute Respiratory Distress Syndrome (ARDS) and multi-organ failure. This physiological reality birthed the paradigm shift from Early Total Care (ETC) to Damage Control Orthopedics (DCO). Today, the decision to proceed with early definitive anterograde nailing versus temporary external fixation hinges on a meticulous assessment of the patient's acid-base status, lactate clearance, coagulation profile, and pulmonary function.

Classification of these fractures is paramount for standardized communication and surgical planning. While the historical Winquist-Hansen classification focused heavily on the degree of comminution and cortical contact to dictate the need for static versus dynamic locking, modern traumatology relies almost exclusively on the AO/OTA classification system. The femoral diaphysis is designated as segment 32. Fractures are subclassified into simple (Type A: spiral, oblique, transverse), wedge (Type B: intact or fragmented butterfly), and complex/multifragmentary (Type C). Understanding this morphology is essential; for instance, a transverse fracture (32-A3) may be notoriously difficult to reduce closed due to the interposition of the linea aspera, whereas a highly comminuted fracture (32-C) relies entirely on the interlocking screws to maintain length and rotation, necessitating meticulous preoperative templating.

Systemic Evaluation and Resuscitation
Before any surgical intervention is contemplated, the patient must undergo a rigorous systemic evaluation. The presence of a femoral shaft fracture implies high-energy trauma until proven otherwise. The primary survey must rule out tension pneumothorax, massive hemothorax, pelvic ring disruptions, and intra-abdominal hemorrhage. The thigh itself can accommodate up to 1.5 liters of extravasated blood, contributing significantly to hemorrhagic shock. Initial management consists of gross realignment of the limb and the application of a traction splint (e.g., Hare or Sager splint). This serves a dual purpose: it restores the cylindrical volume of the thigh to tamponade bleeding via the intact fascial envelope, and it provides crucial pain relief by neutralizing the deforming forces of the robust thigh musculature.

Once the patient is hemodynamically stable, a comprehensive secondary survey is performed. The vascular status of the limb is evaluated by palpating the popliteal, dorsalis pedis, and posterior tibial pulses. It is critical to remember that a palpable pulse represents a pressure wave, not necessarily adequate tissue perfusion. In the setting of high-energy trauma, particularly with associated knee dislocations or highly displaced distal third fractures, an Ankle-Brachial Index (ABI) must be obtained. An ABI of less than 0.9 is highly suspicious for an occult arterial injury and mandates further investigation with CT angiography. Neurological examination, while often limited by patient pain and compliance, must specifically assess the function of the sciatic nerve (peroneal and tibial divisions) and the femoral nerve.

If definitive surgical fixation must be delayed due to physiological instability (DCO pathway) or logistical constraints, the temporary traction splint must be converted to skeletal traction to prevent skin necrosis in the perineum and foot. A proximal tibial traction pin is generally preferred over a distal femoral pin, as the latter can contaminate the future surgical field, tether the quadriceps mechanism, and interfere with the passage of the intramedullary nail. Skeletal traction should be applied with 20 to 30 pounds of weight, ensuring the limb is elevated to facilitate venous drainage and reduce compartment pressures.
Detailed Surgical Anatomy and Biomechanics
Mastery of anterograde femoral nailing requires an intimate, three-dimensional understanding of femoral osteology, the surrounding muscular envelopes, and the critical neurovascular structures that traverse the thigh. The femur is the longest and strongest bone in the human body, designed to transmit massive axial loads and bending moments from the pelvis to the tibia. The diaphysis is not a perfectly straight cylinder; it exhibits a distinct anterior bow, with an average radius of curvature of approximately 120 cm. This anatomical bowing is of paramount importance during intramedullary nailing. A mismatch between the radius of curvature of the selected nail and the patient's native femur can lead to catastrophic complications, including anterior cortical perforation distally or iatrogenic comminution during nail insertion.
The posterior aspect of the femoral diaphysis is characterized by the linea aspera, a prominent longitudinal ridge of thickened cortical bone. This structure serves as the primary attachment site for the fascial septa and massive muscle groups, including the adductors and the vasti. In high-energy transverse fractures, the linea aspera can fracture in continuity with the thick fascial attachments, acting as a robust soft-tissue hinge. If the fracture ends become entrapped within this fascial sleeve, closed reduction becomes nearly impossible without specific maneuvers to "unwind" the soft tissues or, occasionally, a limited open reduction. Furthermore, the thick cortex of the linea aspera dictates the eccentric positioning of the medullary canal, which sits relatively anteriorly within the diaphyseal cross-section.

The vascular supply to the femoral diaphysis is dual-sourced and highly robust, contributing to the generally excellent union rates of these fractures. The primary endosteal supply is derived from the nutrient artery, which typically branches from the second perforating artery of the profunda femoris. It enters the bone posteriorly along the linea aspera, typically in the proximal or middle third of the shaft, and branches proximally and distally within the medullary canal. The periosteal blood supply, derived from the surrounding muscular envelope, supplies the outer one-third of the cortex. Under normal physiological conditions, blood flow is centrifugal (from inside out). However, following a fracture and subsequent intramedullary reaming—which temporarily obliterates the endosteal supply—the flow reverses, becoming centripetal. The periosteal vessels hypertrophy to sustain the healing callus until the endosteal circulation reconstitutes.

Compartmental Anatomy and Neurovascular Relations
The thigh is divided into three distinct fascial compartments: anterior, posterior, and medial. The anterior compartment houses the quadriceps femoris group and the femoral nerve. The posterior compartment contains the hamstring muscles and the sciatic nerve. The medial compartment contains the adductor group and the obturator nerve. During antegrade nailing, the surgical approach to the proximal femur typically exploits the interval between the gluteus medius and gluteus maximus, or involves splitting the gluteus medius and minimus fibers to access the piriformis fossa or greater trochanter. Distally, interlocking screws are placed through the vastus lateralis, necessitating careful blunt dissection to the bone to avoid tethering the muscle fibers, which can lead to postoperative pain and restricted knee flexion.

Neurovascular structures are at risk during specific phases of the procedure. The superior gluteal artery and nerve, which exit the pelvis via the greater sciatic notch and run superior to the piriformis muscle, are highly vulnerable during the establishment of a piriformis fossa entry point. If the awl or entry reamer is directed too medially or superiorly, catastrophic hemorrhage or disabling abductor weakness can ensue. Distally, the perforating branches of the profunda femoris artery wrap around the posterior aspect of the femur. Errant drilling for distal interlocking screws, particularly if directed too posteriorly or if the drill bit plunges past the far cortex, can lacerate these vessels, leading to pseudoaneurysm formation or acute hemorrhage.

Biomechanically, the intramedullary nail functions as a load-sharing device, positioned at the neutral axis of the bone. This central placement minimizes the bending moments exerted on the implant, making it mechanically superior to eccentric plate fixation for diaphyseal fractures. The stability of the construct is governed by the working length of the nail—defined as the distance between the proximal and distal points of fixation (either the locking screws or intimate cortical contact at the isthmus). A shorter working length yields a stiffer construct. While high stiffness is desirable in highly comminuted fractures to maintain length, a construct that is too stiff in a simple transverse fracture may suppress the micromotion necessary for robust secondary callus formation. The modern paradigm emphasizes static locking to control rotation and length, relying on the inherent flexibility of the titanium or steel nail to provide the optimal mechanical environment for healing.

Exhaustive Indications and Contraindications
The decision to proceed with anterograde intramedullary nailing is grounded in a thorough understanding of its absolute and relative indications, weighed against specific patient and fracture variables. Anterograde nailing is the gold standard for the vast majority of adult diaphyseal femoral fractures. It is particularly indicated for closed fractures of the isthmus, where the nail can achieve intimate cortical contact, providing excellent rotational and axial stability. Furthermore, it is the treatment of choice for pathological fractures or impending pathological fractures of the diaphysis, allowing for prophylactic stabilization of the entire bone segment.

Open fractures of the femoral shaft are also routinely managed with intramedullary nailing. For Gustilo-Anderson Grade I, II, and IIIA fractures, immediate reamed intramedullary nailing following meticulous surgical debridement is safe and highly effective, with infection rates comparable to closed fractures. Even in the setting of Grade IIIB and IIIC injuries, early nailing is often performed, provided the soft tissue envelope can be adequately managed and vascular flow is restored. The use of unreamed nails in open fractures, once thought to preserve endosteal blood supply and reduce infection, has largely been abandoned, as modern literature demonstrates that reamed nailing provides superior biomechanical stability and higher union rates without increasing the risk of osteomyelitis.

Contraindications to anterograde nailing, while relatively few, are critical to recognize. Absolute contraindications include the presence of active, untreated osteomyelitis of the femur or a severe, established infection at the proposed proximal entry site (e.g., extensive gluteal decubitus ulcer or deep burns). In the pediatric population, the presence of open proximal femoral physes is an absolute contraindication to rigid, straight antegrade nailing due to the unacceptably high risk of iatrogenic avascular necrosis (AVN) of the femoral head and premature physeal closure. These patients are better served with flexible intramedullary nails or submuscular plating techniques.

Markdown Table: Indications and Contraindications
| Category | Specific Conditions | Rationale / Surgical Considerations |
|---|---|---|
| Absolute Indications | Closed diaphyseal fractures (AO/OTA 32) | Gold standard; provides load-sharing stability and high union rates. |
| Pathological diaphyseal fractures | Allows full-length stabilization; can be combined with tumor resection/cement. | |
| Gustilo Grade I, II, IIIA open fractures | Safe following meticulous debridement; reamed nailing is preferred. | |
| Relative Indications | Polytrauma (Borderline physiology) | Requires careful assessment; ETC vs. DCO based on lactate, base deficit. |
| Ipsilateral femoral neck fracture | Can be managed with a single reconstruction nail or separate constructs (e.g., sliding hip screw + retrograde nail). | |
| Gustilo Grade IIIB/IIIC open fractures | Nailing is viable, but requires multidisciplinary approach for soft tissue/vascular repair. | |
| Relative Contraindications | Extreme anatomical bowing | Risk of anterior cortical perforation; consider plate fixation or custom nails. |
| Narrow medullary canal (< 8mm) | High risk of iatrogenic comminution; requires careful sequential reaming. | |
| Absolute Contraindications | Active femoral osteomyelitis | High risk of propagating infection throughout the entire medullary canal. |
| Open proximal physes (Pediatrics) | Risk of AVN of the femoral head and growth arrest; use flexible nails instead. | |
| Severe soft tissue compromise at entry site | e.g., deep burns over the greater trochanter; precludes safe surgical approach. |

Relative contraindications require nuanced clinical judgment. Patients with extreme anatomical bowing of the femur, often seen in metabolic bone diseases like Paget's disease or osteogenesis imperfecta, may not accommodate a standard intramedullary nail. Forcing a straight or moderately bowed nail into a highly curved femur will inevitably result in iatrogenic fracture or anterior cortical blowout. In these scenarios, alternative fixation methods, such as submuscular plating, or complex reconstructive procedures involving corrective osteotomies prior to nailing, must be considered. Similarly, a congenitally narrow medullary canal (less than 8 mm) poses a significant challenge, requiring meticulous, slow sequential reaming to avoid thermal necrosis and iatrogenic bursting of the diaphysis.

Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of a successful intramedullary nailing procedure. The surgeon must never enter the operating room without a clear, templated roadmap. The radiographic evaluation must include high-quality anteroposterior (AP) and lateral views of the entire femur, strictly adhering to the rule of imaging "a joint above and a joint below." A dedicated internal-rotation AP view of the ipsilateral hip is absolutely mandatory to rule out a concomitant femoral neck fracture, which occurs in up to 10% of femoral shaft fractures and is frequently missed. Given the devastating consequences of a missed femoral neck fracture, modern trauma protocols heavily advocate for a fine-cut CT scan of the pelvis and proximal femur in all high-energy mechanisms.

Templating involves determining the appropriate nail length and diameter. Length is ideally measured from the contralateral, uninjured femur using a radiographic ruler. The goal is to select a nail that extends from the tip of the greater trochanter (or piriformis fossa) to the epiphyseal scar distally, ensuring adequate purchase in the dense cancellous bone of the distal metaphysis. Nail diameter is estimated by measuring the narrowest portion of the medullary canal (the isthmus) on both the AP and lateral radiographs. The surgeon should plan to over-ream the canal by 1.0 to 1.5 mm larger than the selected nail diameter to facilitate smooth insertion and minimize the risk of incarceration.

Table Setup and Patient Positioning
The choice of operating table and patient positioning profoundly influences the ease of reduction and the flow of the operation. The two primary options are the specialized fracture table and a standard radiolucent flat table.
The fracture table allows the patient to be positioned supine or in the lateral decubitus position. The primary advantage of the fracture table is the ability to apply sustained, powerful skeletal traction via a boot or a distal femoral/proximal tibial pin, freeing the surgeon's hands and facilitating closed reduction. However, the fracture table has significant drawbacks. The perineal post places the patient at risk for pudendal nerve palsy and soft tissue necrosis, particularly if surgery is prolonged. Furthermore, positioning the C-arm for unobstructed AP and lateral views of the proximal femur can be technically demanding and time-consuming.

Alternatively, many modern traumatologists prefer the radiolucent flat table with the patient positioned supine ("sloppy lateral" with a bump under the ipsilateral hip). This setup eliminates the risk of pudendal nerve injury and allows for rapid, unimpeded C-arm fluoroscopy from the hip to the knee. However, it requires manual traction or the use of intraoperative skeletal traction devices (e.g., femoral distractor) to achieve length and reduction. The flat table is particularly advantageous in polytrauma patients, as it allows simultaneous access to the abdomen, chest, or contralateral extremities by multiple surgical teams. Regardless of the table chosen, the entire limb from the iliac crest to the toes must be meticulously prepped and draped free to allow for dynamic manipulation during the procedure.

Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of anterograde femoral nailing is a highly choreographed sequence of steps, demanding precision and constant fluoroscopic vigilance. The procedure begins with the establishment of the entry point, which is arguably the most critical step of
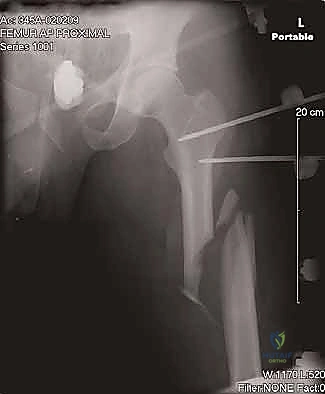
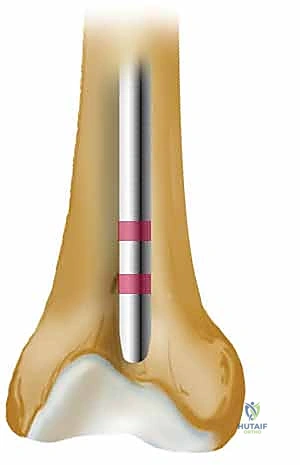
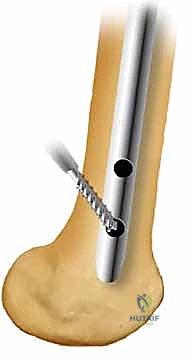
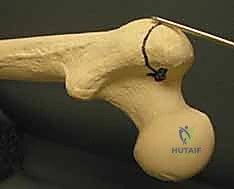
Clinical & Radiographic Imaging Archive