ACL Reconstruction in the Skeletally Immature Patient: An Intraoperative Masterclass

Key Takeaway
This masterclass details anterior cruciate ligament (ACL) reconstruction in skeletally immature patients, focusing on physeal-sparing and transphyseal techniques. We cover comprehensive anatomy, preoperative planning, granular intraoperative steps, critical pearls and pitfalls, and extensive postoperative management. Essential for fellows mastering pediatric orthopaedic surgery.
Comprehensive Introduction and Patho-Epidemiology
The Changing Landscape of Pediatric Knee Injuries
Welcome, fellows and colleagues, to another definitive session in the operating theater. Today, we are undertaking an exhaustive review of one of the most intellectually and technically demanding procedures in pediatric orthopaedics: Anterior Cruciate Ligament (ACL) reconstruction in the skeletally immature patient. Historically, the prevailing dogma suggested that the pediatric equivalent of an adult ACL rupture was invariably a tibial eminence avulsion fracture, owing to the relative weakness of the unossified chondroepiphysis compared to the robust native ligamentous tissue. However, the epidemiological landscape has shifted dramatically over the past two decades. We are now witnessing an exponential increase in the frequency of true intrasubstance ACL tears in children and adolescents. This paradigm shift is largely driven by early single-sport specialization, year-round competitive play, and the increasing intensity of youth athletics.
This is emphatically not just an adult ACL reconstruction scaled down to fit a smaller knee. The skeletally immature patient presents a unique biological milieu that demands a profound, nuanced understanding of growth plate biology, meticulously executed surgical technique, and a highly tailored, patient-specific approach. The presence of open physes—specifically the distal femoral and proximal tibial growth plates—dictates our entire surgical philosophy. Our primary objective is twofold: we must restore the complex biomechanical stability of the knee to prevent devastating secondary intra-articular injuries, while simultaneously navigating the treacherous anatomical corridors to prevent iatrogenic growth disturbances, such as premature physeal closure, angular deformities, or clinically significant leg-length discrepancies.
The natural history of the unaddressed pediatric ACL-deficient knee is unforgiving. Unstabilized, these knees are subjected to repetitive microtrauma and macroscopic giving-way episodes, which almost universally lead to rapid, progressive deterioration of the menisci and articular cartilage. The posterior horn of the medial meniscus, which acts as the primary secondary restraint to anterior tibial translation in the ACL-deficient knee, is particularly vulnerable. Once this meniscal wedge is compromised, the knee enters a spiral of accelerated degenerative changes, often culminating in early-onset osteoarthritis within four to five years of the index injury. Therefore, our surgical mandate is clear: we must stabilize the joint, preserve the meniscal and chondral envelopes, and safeguard the patient's future joint health, all while respecting the immense regenerative and growth potential of their open physes.
Pathomechanics and the Traumatic Hemarthrosis
When evaluating these young athletes, the clinical history is often classic, though eliciting it requires patience. Patients, or more frequently their observant parents, will report a distinct, audible or palpable "pop" at the exact moment of injury. This is typically a non-contact mechanism involving a rapid deceleration, a sudden change of direction (cutting), or an awkward landing from a jump with the knee in a near-extended, valgus position. This catastrophic failure of the ligament is immediately followed by the rapid onset of a tense knee effusion. This acute traumatic hemarthrosis is a hallmark sign, present in up to 65% to 70% of pediatric ACL injuries, and should be considered an ACL tear until proven otherwise via advanced imaging or examination under anesthesia.
On magnetic resonance imaging (MRI), we routinely observe a highly characteristic and virtually pathognomonic pattern of osseous contusions, or bone bruises. These are typically located on the posterior aspect of the lateral tibial plateau and the corresponding distal aspect of the lateral femoral condyle near the sulcus terminalis.

This specific bone bruise pattern is the radiographic footprint of the injury mechanism. It reflects the violent, transient impaction that occurs as the tibia subluxates anteriorly and internally rotates relative to the femur during the catastrophic "shift" of the knee at the moment the ACL ruptures. Understanding this pathomechanics is crucial, as the severity of these bone bruises often correlates with concomitant osteochondral injuries that must be meticulously evaluated and potentially addressed during the surgical reconstruction. Furthermore, the presence of these bruises serves as a stark visual reminder of the immense forces absorbed by the pediatric joint during these non-contact pivoting episodes.
Detailed Surgical Anatomy and Biomechanics
The Anterior Cruciate Ligament Bundles and Footprints
To master pediatric ACL reconstruction, one must first master the intricate three-dimensional anatomy of the native ligament. The ACL is a complex, multifascicular structure, originating from a broad, semicircular footprint on the posterior portion of the medial aspect of the lateral femoral condyle. From this femoral origin, the ligament courses obliquely—anteriorly, medially, and distally—across the intercondylar notch to insert onto a wide footprint on the anteromedial aspect of the tibial plateau, situated just anterior and lateral to the medial tibial eminence (spine).
Functionally and anatomically, the ACL is divided into two distinct, synergistic bundles named for their tibial insertion sites: the anteromedial (AM) bundle and the posterolateral (PL) bundle. The AM bundle is the more anterior and vertical of the two; it primarily resists anterior tibial translation and experiences its maximum tension in the last 30 degrees of extension and early flexion. Conversely, the PL bundle is more posterior and oblique. It is more isometric throughout the range of motion but is absolutely critical for rotational control, particularly in resisting the pivot-shift phenomenon near full extension.
In the skeletally immature knee, recreating this complex, dual-bundle biomechanics is challenging due to the limited real estate available for tunnel placement without violating the physes. While anatomic single-bundle reconstructions targeting the center of the native footprint are the standard of care to restore both translational and rotational stability, the surgeon must possess a profound understanding of how subtle deviations in tunnel placement will disproportionately affect knee kinematics. A tunnel placed too vertically (a common historical error in trans-tibial drilling) will fail to restore the function of the PL bundle, leaving the child with persistent rotational instability despite a negative Lachman test.
Physeal Proximity and Growth Plate Biology
The absolute crux of pediatric ACL reconstruction lies in the intimate, perilous proximity of the native ACL attachment sites to the adjacent open physes. The physes are highly active, biologically complex zones of endochondral ossification responsible for longitudinal bone growth. The distal femoral physis is the most active growth plate in the human body, contributing approximately 70% of the longitudinal growth of the femur and 37% of the entire lower extremity (growing at a rate of roughly 9 mm per year). The proximal tibial physis is similarly critical, contributing 55% of the tibia's length (roughly 6 mm per year).

The tibial footprint of the ACL is relatively "safe," typically located 15 to 20 mm proximal to the undulating proximal tibial physis. However, the femoral attachment is a veritable minefield. The distal femoral physis curves precipitously in the posterior notch, coming within mere millimeters of the femoral attachment of the ACL, particularly at the most posterior and proximal aspect of its insertion. This intimate relationship is why conventional adult transphyseal techniques, which utilize large-diameter tunnels and robust interference screw fixation at the aperture, carry an unacceptably high risk of iatrogenic growth disturbance in young children.
Any insult to the physis—whether from the thermal necrosis of drilling, the physical volumetric displacement of a bone plug, the rigid compression of an interference screw, or even the sustained compressive forces of a highly tensioned soft-tissue graft crossing the growth plate (the "tethering" effect)—can induce premature, asymmetric physeal closure. A central arrest typically leads to a leg-length discrepancy, while a peripheral arrest will inevitably lead to a progressive angular deformity, such as genu valgum or recurvatum, depending on the specific quadrant of the physis violated. Therefore, absolute respect for the perichondrial ring of LaCroix and the zone of Ranvier is mandatory during all surgical dissection and tunnel preparation.
Associated Intra-Articular and Neurovascular Structures
Beyond the ligament and the physes, the pediatric knee is surrounded by critical intra-articular and neurovascular structures that demand meticulous attention. Associated injuries are rampant in this population and must be systematically ruled out or addressed. Lateral meniscus tears are exceedingly common acutely, often occurring at the posterior root or as vertical longitudinal tears in the periphery. In chronically ACL-deficient knees, the posterior horn of the medial meniscus is at massive risk, as it acts as the primary "chock block" preventing anterior tibial subluxation.
Furthermore, collateral ligament injuries, particularly to the medial collateral ligament (MCL), frequently accompany acute ACL ruptures. While many pediatric MCL injuries can be managed non-operatively with bracing, severe grade III injuries may require concurrent or staged surgical intervention. Chondral injuries, ranging from focal osteochondral defects to widespread cartilage delamination, are also significant concerns that dictate long-term prognosis. Finally, though statistically less common in children than adults, a missed posterolateral corner (PLC) injury is a notorious cause of early ACL reconstruction failure. The popliteus tendon, fibular collateral ligament, and popliteofibular ligament must be thoroughly assessed.
Neurovascularly, the posterior aspect of the knee houses the popliteal artery and vein, as well as the tibial nerve. These structures are at risk during over-penetration of guide pins or drills, particularly during tibial tunnel creation or when working deep in the posterior notch. Laterally, the common peroneal nerve wraps intimately around the fibular neck; it is highly vulnerable during lateral extra-articular procedures, such as the harvest of an iliotibial band graft or the creation of a lateral extra-articular tenodesis. Meticulous surgical technique, the use of protective retractors, and fluoroscopic guidance when necessary are essential to avoid catastrophic iatrogenic injury to these vital structures.
Exhaustive Indications and Contraindications
Defining the Threshold for Operative Intervention
The decision-making process for an ACL tear in a skeletally immature patient is one of the most heavily debated topics in pediatric orthopaedics. Historically, a "wait-and-see" approach was advocated, delaying reconstruction until skeletal maturity to avoid physeal injury. However, landmark longitudinal studies have unequivocally demonstrated that delaying surgery in an active child with a complete ACL tear leads to an unacceptably high rate of secondary meniscal and chondral damage. Therefore, the current standard of care heavily favors early surgical stabilization for the vast majority of pediatric patients with complete intrasubstance ruptures who wish to return to cutting and pivoting sports.
Operative intervention is strongly indicated for patients with a complete ACL tear accompanied by subjective episodes of instability (giving way) during activities of daily living or sports. Furthermore, the presence of repairable, concurrent intra-articular pathology—such as a bucket-handle meniscal tear or a significant osteochondral defect—represents an absolute indication for early surgery. In these scenarios, the ACL must be reconstructed to protect the meniscal repair or cartilage restoration procedure; a meniscal repair in an ACL-deficient knee has a high likelihood of failure due to ongoing abnormal shear forces.
For partial or incomplete tears, the indications are more nuanced. If the tear involves less than 50% of the ligament, the posterolateral bundle is relatively preserved, and the patient has a normal or near-normal Lachman and pivot-shift test under anesthesia, a trial of non-operative management may be considered. This involves rigorous physical therapy, bracing, and strict activity modification. However, the surgeon must maintain a low threshold to convert to surgical reconstruction if the patient develops functional instability or fails to progress in their rehabilitation.
Absolute and Relative Contraindications
While early reconstruction is generally favored, there are strict contraindications that must be respected. Absolute contraindications include the presence of active, untreated intra-articular or peri-articular infection, which must be eradicated prior to any elective ligamentous reconstruction. Severe, uncorrected malalignment of the lower extremity (e.g., profound genu varum or valgum) is also a contraindication to isolated ACL reconstruction, as the abnormal mechanical axis will place excessive stress on the graft, leading to premature failure. In such cases, a staged or concurrent corrective osteotomy must be considered.
Relative contraindications revolve primarily around the patient's biological age and psychosocial factors. In exceedingly young patients (e.g., Tanner stage I, chronological age under 8 years) with massive growth potential remaining, the risk of iatrogenic growth disturbance is at its absolute zenith. In these rare cases, if the knee is relatively stable and there are no concurrent meniscal injuries, a prolonged period of non-operative management with custom bracing may be attempted, though it requires immense compliance from the patient and family.
Furthermore, poor patient or parental compliance is a significant relative contraindication. Pediatric ACL reconstruction requires a grueling, months-long postoperative rehabilitation protocol. If the surgeon suspects that the family cannot adhere to the strict weight-bearing restrictions, bracing requirements, and physical therapy milestones, the risk of early graft failure or catastrophic complications (like arthrofibrosis) outweighs the benefits of the procedure.
| Category | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Clinical Status | Recurrent functional instability (giving way) | Active local or systemic infection |
| Associated Injuries | Repairable meniscal tear (e.g., bucket-handle) | Severe, uncorrected lower extremity malalignment |
| Associated Injuries | Concomitant osteochondral defect requiring repair | Complex regional pain syndrome (CRPS) |
| Activity Level | Desire to return to high-demand, pivoting sports | Sedentary lifestyle with no functional instability |
| Anatomy/Tear Type | Complete intrasubstance ACL rupture | Asymptomatic partial tear (<50% involvement) |
| Psychosocial | High compliance with postoperative rehabilitation | Documented inability to comply with strict rehab |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Tanner Staging
The foundation of a successful pediatric ACL reconstruction is laid long before the patient enters the operating room. A meticulous, comprehensive clinical evaluation is paramount. Adolescents can be notoriously poor historians, so the surgeon must act as a detective, gleaning every possible detail about the mechanism of injury, the presence of acute or recurrent effusions, and the specific activities that elicit instability. The physical examination must be thorough and comparative, always using the uninjured contralateral knee as the baseline, as pediatric athletes frequently exhibit a high degree of baseline physiologic ligamentous laxity.
The single most critical factor in pre-operative planning is the accurate determination of the patient's physiologic age and remaining growth potential. Chronological age is notoriously unreliable. We must formally assess the patient's Tanner staging (Stages I through V) in the clinic, evaluating secondary sexual characteristics, and then confirm these findings. Tanner staging provides a robust clinical proxy for the status of the physes. A Tanner stage I or II patient has wide-open physes and massive growth potential, necessitating a strictly physeal-sparing approach. A Tanner stage III patient is in the transitional phase, while Tanner IV and V patients are nearing skeletal maturity and can often be treated with adult-type transphyseal techniques.
To definitively quantify skeletal age, we routinely obtain standardized posteroanterior (PA) radiographs of the left hand and wrist. These images are meticulously compared against the Greulich and Pyle atlas. This radiographic skeletal age, combined with the clinical Tanner stage, dictates our entire surgical algorithm. Furthermore, full-length, weight-bearing hip-to-ankle radiographs are obtained if there is any clinical suspicion of varus or valgus malalignment, as unaddressed mechanical axis deviations will doom the reconstruction to failure.
Advanced Imaging and Pre-Operative Templating
Advanced imaging is the cornerstone of our pre-operative templating. While plain radiographs (AP, lateral, tunnel, and sunrise views) are essential to rule out physeal fractures, tibial eminence avulsions, and osteochondritis dissecans (OCD) lesions, an MRI is the definitive diagnostic modality for evaluating the ACL and the entire intra-articular envelope. We meticulously review the sagittal, coronal, and axial sequences to assess the integrity of the ACL fibers, the presence of the characteristic bone bruising, and the status of the menisci and articular cartilage.
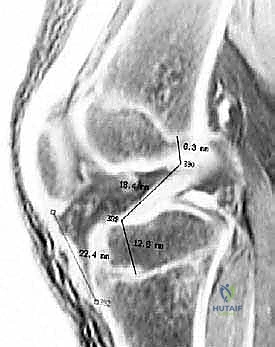
Crucially, the MRI is also used for pre-operative templating of the physes. We carefully evaluate the undulating topography of the distal femoral and proximal tibial physes in relation to the native ACL footprints. We measure the exact distance from the proposed tunnel apertures to the physis, mapping out our trajectory to ensure we maintain a safe margin of at least 3 to 5 millimeters. It is important to note that MRI can be less sensitive and specific for ACL injuries in the pediatric population compared to adults, and it carries a higher false-positive rate for meniscal tears due to the increased vascularity and signal intensity of the normal pediatric meniscus. Therefore, the MRI findings must always be correlated with the clinical exam.

The algorithm above illustrates our decision-making matrix based on Tanner staging and physiologic age. This is not a mere suggestion; it is a rigid protocol designed to minimize the catastrophic risk of growth arrest while maximizing joint stability.
Operating Room Setup and Patient Positioning
Meticulous operating room setup and patient positioning are critical for executing these technically demanding procedures flawlessly. Once the patient is anesthetized, a comprehensive examination under anesthesia (EUA) is mandatory. This is the moment of truth where we definitively assess the Lachman test, the pivot-shift phenomenon (which is often poorly tolerated in the awake pediatric patient), and the integrity of the collateral ligaments and posterolateral corner without the confounding factor of muscle guarding.
The patient is positioned supine on a standard operating table. A well-padded high-thigh tourniquet is applied to the operative leg, but it is typically only inflated if visualization becomes severely compromised, as we prefer to minimize ischemic time to the developing musculature. The contralateral leg is carefully padded and placed in a well-leg holder or secured flat on the table, ensuring all bony prominences are protected to prevent neuropraxia.
The operative leg is placed in a specialized knee positioner (such as a morph board or a commercial leg holder) that allows for a full, unobstructed range of motion from hyperextension to hyperflexion (at least 120 degrees). This extreme flexion is absolutely critical, particularly when drilling the femoral tunnel through an anteromedial portal in all-epiphyseal or transphyseal techniques, to ensure the tunnel trajectory avoids the posterior aspect of the distal femoral physis. The entire extremity is prepped and draped in a standard sterile fashion, ensuring access to the iliac crest if bone grafting is anticipated.
Step-by-Step Surgical Approach and Fixation Technique
Algorithm for Skeletally Immature ACL Reconstruction
Our surgical approach is entirely dictated by the patient's skeletal maturity. We employ a strict, tiered algorithm. For prepubescent patients with wide-open physes and significant growth remaining (Tanner stages I and II, skeletal age <10 in girls, <12 in boys), we utilize strictly physeal-sparing techniques. For adolescent patients in the transitional phase of growth (Tanner stage III, skeletal age 11-13 in girls, 13-14 in boys), we utilize partial transphyseal or all-epiphyseal techniques. Finally, for older adolescents nearing skeletal maturity (Tanner stages IV and V, skeletal age >14 in girls, >15 in boys), we utilize modified transphyseal techniques, taking great care to use soft-tissue grafts and place fixation hardware far away from the closing physes.

Regardless of the technique chosen, the diagnostic arthroscopy is the first critical step. We establish standard anterolateral and anteromedial portals, being mindful that the joint space in a child is smaller and the articular cartilage is thicker and softer, making it highly susceptible to iatrogenic scuffing from our instruments. We systematically evaluate all compartments, probe the menisci meticulously, and address any concurrent pathology before proceeding to the ACL reconstruction.
Physeal-Sparing Techniques (Iliotibial Band Autograft)
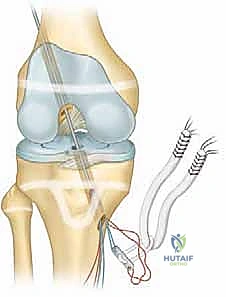
For the youngest, most vulnerable patients (Tanner I/II), the Micheli-Kocher combined intra-articular and extra-articular physeal-sparing reconstruction using an iliotibial band (ITB) autograft is our gold standard. This technique brilliantly completely avoids drilling tunnels across either the femoral or tibial physes.
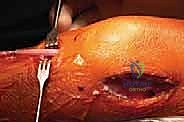
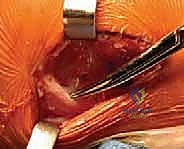
We begin by harvesting a long, robust strip of the central third of the ITB, leaving its distal attachment at Gerdy's tubercle intact. The graft is meticulously tubularized with high-strength, non-absorbable suture. We then create a carefully placed "over-the-top" route on the femur. A curved clamp is passed through the posterior capsule, superior to the lateral femoral condyle, taking extreme care to stay extra-periosteal and well away from the perichondrial ring.

The tubularized ITB graft is passed through this over-the-top position, routed through the intercondylar notch, and brought out anteriorly. For the tibial fixation, instead of a transphyseal tunnel, we create a trough in the proximal tibial epiphysis, anterior to the tibial spine, or we route the graft under the intermeniscal ligament and suture it directly to the periosteum of the proximal tibia, distal to the physis. This creates a stable, living graft that respects the growth plates entirely.


Partial Transphyseal and All-Epiphyseal Techniques
For Tanner III patients, we often employ the all-epiphyseal technique popularized by Anderson. This highly technical procedure utilizes hamstring autograft and relies on precise fluoroscopic guidance to drill sockets entirely within the epiphyses of the femur and tibia, never crossing the radiolucent physis.

The tibial tunnel is the most challenging aspect. Under direct AP and lateral fluoroscopy, a guide pin is introduced from the medial aspect of the proximal tibial epiphysis, aiming for the center of the native ACL footprint, remaining strictly superior to the proximal tibial physis. The femoral socket is typically drilled through an accessory anteromedial portal with the knee in hyperflexion to ensure the trajectory stays within the distal femoral epiphysis.


Alternatively, a partial transphyseal approach may be used, where a small-diameter (typically 7-8mm) vertical tunnel is drilled centrally across the tibial physis, but the femoral fixation remains all-epiphyseal or "over-the-top." The central placement of the tibial tunnel is crucial; if a growth arrest occurs centrally, it results in a leg-length discrepancy, which is easier to
Clinical & Radiographic Imaging Archive