ANKYLOSING SPONDYLITIS: PATHOPHYSIOLOGY AND CLINICAL PRESENTATION
Ankylosing spondylitis (AS) is a chronic, progressive inflammatory spondyloarthropathy that primarily affects the axial skeleton, sacroiliac joints, peripheral joints, and entheses. It belongs to a broader family of seronegative spondyloarthropathies, which includes enteropathic arthritis (associated with Crohn's disease and ulcerative colitis), reactive arthritis (Reiter syndrome), and psoriatic arthritis. When associated with these systemic disorders, ankylosing spondylitis often exhibits a significantly more severe clinical course, particularly regarding spinal involvement.
The disease has a well-established genetic predisposition, with the HLA-B27 antigen present in 88% to 96% of affected patients. Epidemiologically, men are affected four times more frequently than women, with the onset of symptoms typically occurring in the second and third decades of life. The prevalence in the Caucasian male population is estimated at 0.5 to 1 per 1,000.
Initially, patients present with insidious lower back pain and profound morning stiffness that improves with activity. As the disease progresses, the inflammatory enthesopathy leads to progressive ossification and ankylosis, typically advancing in a caudal-to-cephalad direction. Paradoxically, as the spine completely fuses, axial pain symptoms often improve, though the patient is left with a rigid, biomechanically compromised spine.
Extraspinal and Systemic Manifestations
Orthopaedic surgeons must remain acutely aware of the systemic manifestations of AS, as they directly impact perioperative management:
* Ocular: Acute anterior uveitis (iritis) occurs in up to 40% of patients, requiring urgent ophthalmological care to prevent synechiae and permanent vision loss.
* Pulmonary: Apical pulmonary cavitary lesions and interstitial fibrosis can occur. Furthermore, fusion of the costochondral and costovertebral articulations severely restricts chest wall expansion, rendering respiration almost entirely diaphragmatic.
* Cardiovascular: Aortitis can lead to aortic root dilation, aortic insufficiency, and conduction defects (e.g., AV block).
* Renal: Secondary amyloidosis (AA type) can precipitate progressive renal failure.
* Peripheral Joints: Hip arthritis is common and may progress to spontaneous arthrodesis, severely compounding the patient's functional disability when combined with a rigid spine.
RADIOGRAPHIC EVALUATION AND BIOMECHANICS
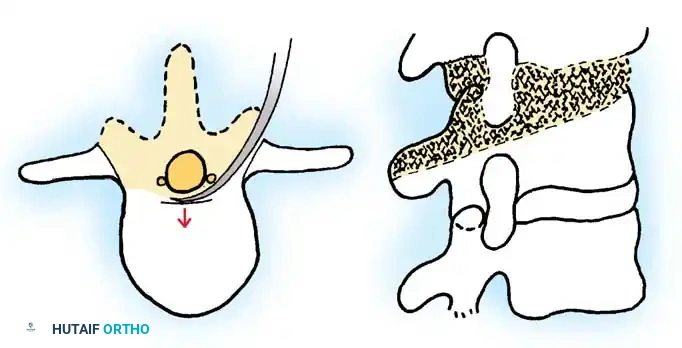
The radiographic hallmark of ankylosing spondylitis begins with bilateral, symmetrical sacroiliitis, eventually leading to complete fusion of the sacroiliac joints. In the vertebral column, the initial inflammatory phase involves bone resorption at the entheses (Romanus lesions), causing periarticular osteopenia and the characteristic "squaring off" of the anterior vertebral body corners.
Subsequent ossification occurs within the outer fibers of the annulus fibrosus (syndesmophytes), while typically sparing the anterior longitudinal ligament (ALL) and the central intervertebral disc. This creates the classic "bamboo spine" appearance. The posterior elements are similarly affected, with dense ossification of the facet joints, interspinous ligaments, supraspinous ligaments, and the ligamentum flavum.
Clinical Pearl: The ankylosed spine acts biomechanically as a single, long osteopenic bone. It lacks the shock-absorbing capacity of mobile segments, making it highly susceptible to shear forces and transverse fractures even from trivial trauma.
Cervical Spine Involvement and Instability
Atlantoaxial instability is a critical consideration and must be actively ruled out in any AS patient undergoing surgery, regardless of the primary indication. Because the subaxial spine becomes completely rigid, physiological stresses are disproportionately transferred to the craniocervical junction. Consequently, atlantoaxial instability occurs in 25% to 90% of patients with advanced AS.
Surgical intervention at the cervical spine is dictated by the presence of intractable pain, neurological deficits, and radiographic parameters of instability (e.g., Posterior Atlantodental Interval [PADI] < 14 mm, Space Available for Cord [SAC] < 13 mm). Management ranges from conservative observation to complex occipitocervical (O-C2) or C1-C2 fusions, depending on the reducibility of the deformity and the presence of basilar invagination.
SPINAL FRACTURES IN THE ANKYLOSED SPINE
Spinal fractures in patients with ankylosing spondylitis are catastrophic, frequently life-threatening injuries. They most commonly occur in the lower cervical spine or at the cervicothoracic junction. Because the spine is rigid and osteopenic, these "chalk stick" fractures are highly unstable, often involving all three spinal columns.
Diagnosis and Emergency Management
A high index of suspicion is mandatory. Any perceived change in spinal alignment or new-onset axial pain in an AS patient, even following trivial trauma, must be considered a fracture until proven otherwise.
- Delayed Diagnosis: These fractures are notoriously discovered late. Persistent pain may be the only initial finding, with catastrophic neurological deterioration occurring days or weeks later due to progressive translation or epidural hematoma.
- Radiographic Findings: A widened anterior disc space may be the only obvious plain radiographic finding. This creates a highly unstable configuration prone to translation. CT with sagittal and coronal reconstructions is the gold standard for diagnosis, while MRI is essential to evaluate the spinal cord, epidural space (for hematoma), and ligamentous disruption.
Surgical Warning: The standard emergency protocol is to immobilize the patient in the exact position in which they are found. Forcing an AS patient with a fixed kyphotic deformity into a standard flat cervical collar or rigid backboard can cause sudden hyperextension, massive translation at the fracture site, and immediate spinal cord transection.
Treatment Strategies for Fractures
The management of AS spinal fractures remains controversial, balancing the high morbidity of surgery against the risks of conservative care.
- Conservative Management: Historically advocated by some authors (Graham, Rowed) using traction and halo immobilization. Traction must be meticulously designed to reestablish the patient's previous kyphotic deformity, not to achieve a "normal" anatomical alignment. However, halo vests in severe kyphosis are difficult to fit, poorly tolerated, and carry a high risk of pin-site infections, skin breakdown, and loss of reduction.
- Operative Stabilization: Modern consensus heavily favors early surgical stabilization. Due to the three-column nature of these injuries, long-segment posterior instrumentation (at least three levels above and below the fracture) is required.
- Complications: Pseudarthrosis is a frequent complication. Late radiographic findings include progressive disc space widening and discovertebral disruption. Occult fractures may present as a "hot" spot on a bone scan in an otherwise metabolically inactive, fused spine.
SURGICAL CORRECTION OF SEVERE SPINAL DEFORMITY
As ankylosing spondylitis progresses, patients often develop a severe, rigid thoracolumbar kyphosis. This debilitating flexion deformity severely restricts the patient's field of vision, limits ambulation, and causes visceral compression leading to gastrointestinal distress and restrictive pulmonary disease.
Preoperative Evaluation: The Chin-Brow to Vertical Angle (CBVA)
The primary metric for evaluating global sagittal balance and the patient's horizontal gaze is the Chin-Brow to Vertical Angle (CBVA).
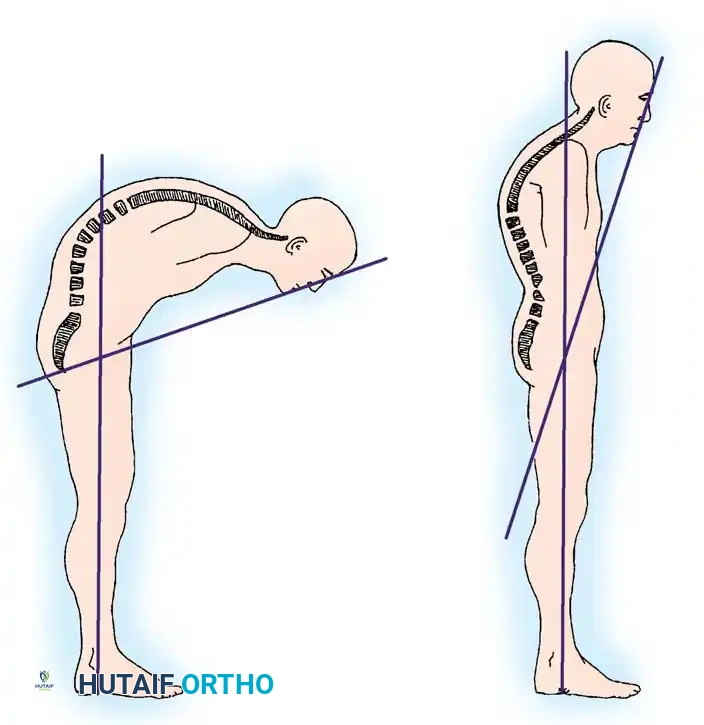
The CBVA is measured with the patient standing with hips and knees extended and the neck in a fixed or neutral position. An angle is drawn from the patient's brow to their chin, and the intersection of this line with the true vertical represents the CBVA. The surgical goal is to restore the CBVA to approximately 10 to 20 degrees of flexion, allowing the patient to see straight ahead while maintaining the ability to look down for ambulation.
Principles of Spinal Osteotomy
Corrective osteotomies are typically performed in the mid-to-lower lumbar spine (L2, L3, or L4) for several reasons:
1. The spinal canal is wider in the lumbar region, accommodating the cauda equina more safely than the thoracic spinal cord.
2. The osteotomy is distal to the conus medullaris, reducing the risk of central cord injury.
3. Creating lumbar lordosis effectively compensates for fixed thoracic kyphosis.
Surgical Warning: Extreme deformities may require staged corrections. Rapid, single-stage correction of massive deformities carries a severe risk of stretching and rupturing the aorta or inferior vena cava, particularly if the vessels are tethered to the anterior longitudinal ligament (a risk heightened in patients who previously received radiation therapy for AS).
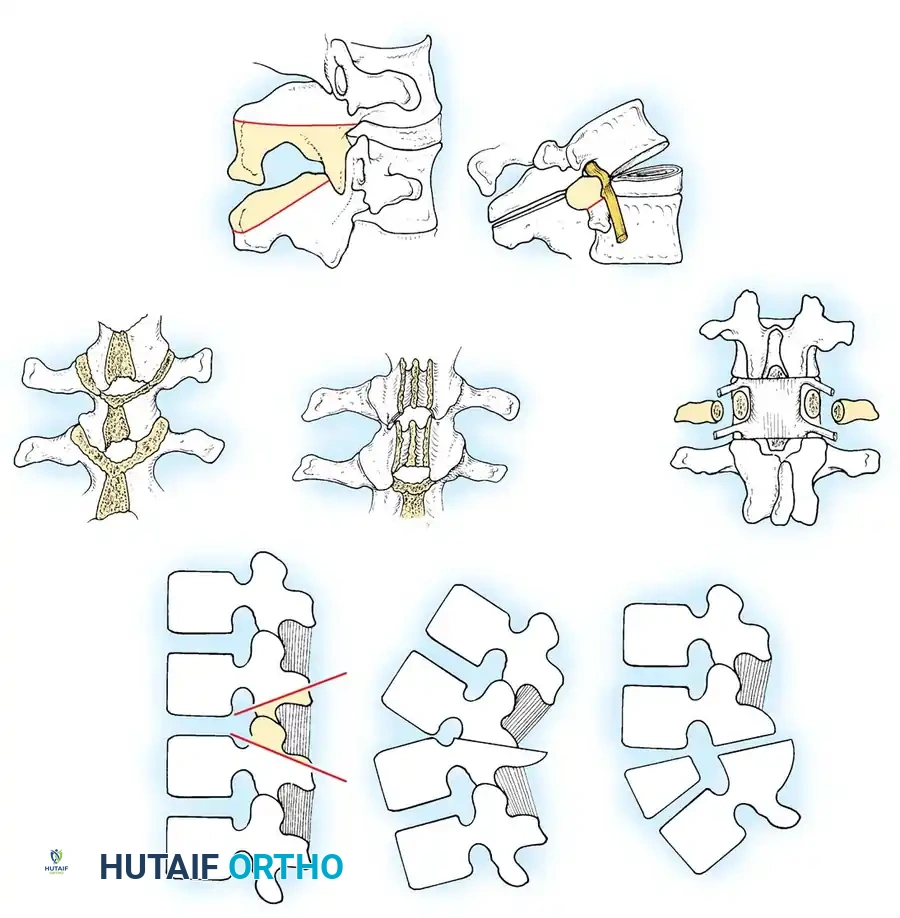
1. The Smith-Petersen Osteotomy (SPO)
Originally described in 1945, the Smith-Petersen Osteotomy is a posterior column shortening procedure. It is an excellent option for correcting smaller degrees of spinal deformity or when multiple levels of correction are desired.
Technique:
* A wide posterior exposure is achieved.
* Bone is resected through the pars interarticularis and the fused facet joints. If a previous fusion mass is present, it is thinned using a high-speed burr until the ligamentum flavum or dura is exposed.
* Symmetrical, V-shaped resection of the posterior elements is mandatory to prevent inducing an iatrogenic coronal deformity.
* The underlying ossified ligaments must be completely excised to prevent dural buckling and iatrogenic spinal stenosis during closure.
* Biomechanics: The osteotomy hinges on the posterior longitudinal ligament (PLL) or the posterior annulus. In a mobile spine, the anterior column opens through the disc space. However, in AS, the anterior longitudinal ligament and disc are ossified. Therefore, closure of the posterior osteotomy requires controlled osteoclasis (fracture) of the anterior column.
* Correction Yield: Approximately 10 degrees of lordosis is obtained for every 10 mm of posterior bone resection.
2. Pedicle Subtraction Osteotomy (PSO)
The Pedicle Subtraction Osteotomy is a three-column, closing-wedge osteotomy. It is the procedure of choice for patients with significant sagittal imbalance (>4 cm SVA) and completely fused anterior columns.
Advantages over SPO: PSO is inherently safer for the major anterior vascular structures because it does not lengthen the anterior column. Instead, it shortens the posterior and middle columns while hinging on the anterior cortex of the vertebral body.
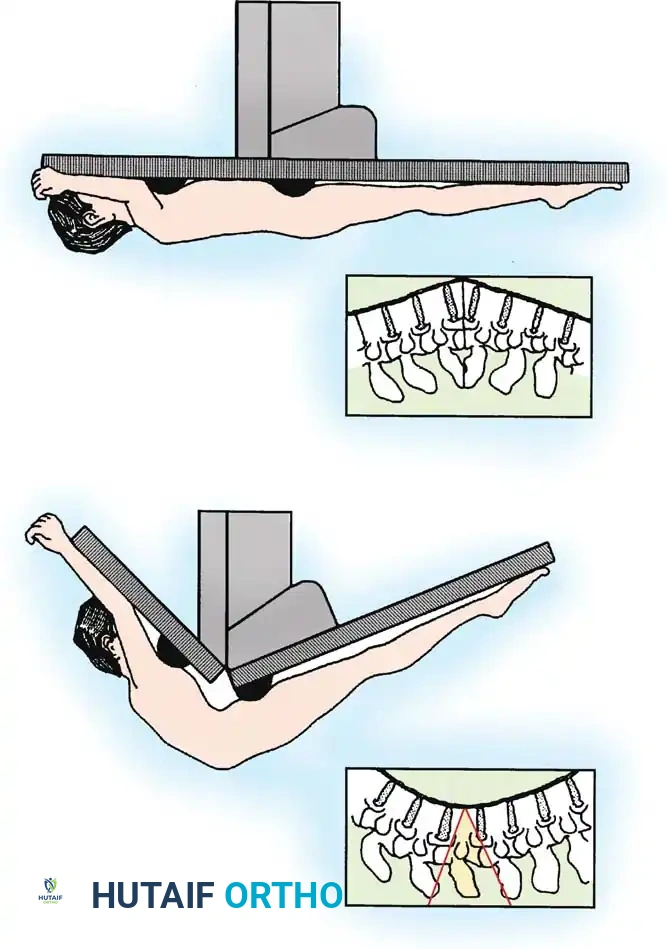
Technique and Positioning:
* Positioning: The patient is placed prone on a specialized hinged operative table (e.g., Jackson table with a hinge mechanism). Meticulous padding is required. The table is initially positioned to accommodate the patient's fixed kyphosis.
* Exposure & Instrumentation: Pedicle screws are placed multiple levels above and below the planned osteotomy site (typically L3).
* Decompression: A wide laminectomy is performed at the target level, completely exposing the dura and the exiting nerve roots bilaterally.
* Decancellization: The pedicles of the target vertebra are hollowed out using burrs and curettes. The decancellization is extended into the vertebral body, creating a wedge-shaped void with the apex at the anterior cortex.
* Posterior Wall Resection: The posterior wall of the vertebral body is carefully impacted into the created cavity, ensuring no bone fragments retropulse into the spinal canal.
* Closure: The osteotomy is closed by gradually extending the hinged operating table and applying compression across the posterior instrumentation. The dura must be directly visualized during closure to ensure it does not buckle or become compressed.
* Correction Yield: A single-level PSO typically provides 30 to 40 degrees of sagittal correction.
3. Eggshell Osteotomy / Vertebral Column Resection (VCR)
The eggshell osteotomy, or Vertebral Column Resection, is the most aggressive corrective procedure, reserved for severe, rigid, multiplanar deformities (e.g., sagittal imbalance >10 cm combined with severe coronal decompensation).
Technique:
* This is a profound spinal shortening procedure. It involves complete circumferential decancellization of the vertebral body ("eggshelling").
* The posterior elements, pedicles, and the entire vertebral body are resected, leaving only a thin rim of anterior and lateral cortical bone to protect the great vessels.
* The spine is then shortened and realigned using robust posterior instrumentation.
* Because this creates a massive destabilization of all three columns, temporary stabilizing rods must be utilized during the resection phase to prevent catastrophic spinal subluxation and spinal cord transection.
PERIOPERATIVE COMPLICATIONS AND MANAGEMENT
Spinal osteotomies in the ankylosed spine are highly demanding procedures with a steep learning curve. The morbidity and mortality rates, while improved with modern techniques, remain significant.
- Neurological Deficits: Can occur from dural buckling, direct trauma, or subluxation during osteotomy closure. A wake-up test or continuous intraoperative neuromonitoring (SSEP and MEP) is mandatory.
- Vascular Injury: Rupture of the aorta or inferior vena cava is a catastrophic risk, particularly during opening-wedge osteotomies (SPO) in patients with prior radiation therapy.
- Dural Tears: The dura in AS patients is often thin, friable, and densely adherent to the ossified ligamentum flavum. Dural tears are common and must be meticulously repaired to prevent cerebrospinal fluid leaks and pseudomeningoceles.
- Systemic Complications: Prolonged prone positioning in patients with restrictive lung disease and rigid chest walls can lead to severe postoperative pulmonary complications. Extubation should be delayed until the patient is fully awake and demonstrating adequate spontaneous tidal volumes.
- Pseudarthrosis and Hardware Failure: Due to the long lever arms of the ankylosed spine, massive biomechanical forces are concentrated at the osteotomy site. Robust, multi-rod constructs and copious autologous cancellous bone grafting are essential to achieve solid arthrodesis.
CONCLUSION
The operative management of ankylosing spondylitis requires a profound understanding of the disease's unique biomechanics, systemic manifestations, and altered surgical anatomy. Whether managing a highly unstable "chalk stick" fracture or executing a complex Pedicle Subtraction Osteotomy for severe sagittal imbalance, the orthopaedic surgeon must employ meticulous preoperative planning, specialized positioning techniques, and rigid internal fixation to optimize patient outcomes and minimize catastrophic complications.
📚 Medical References
- ankylosing spondylitis: a multicenter study, Orthopedics 18:1005, 1995.
- Beard VV, Hochschuler SH: Refl ex sympathetic dystrophy following spinal surgery, Semin Spine Surg 5:153, 1993.
- Beaty JH, ed: Orthopaedic knowledge update, home study syllabus 6, Rosemont, Ill, 1999, American Academy of Orthopaedic Surgeons. Bohlman HH: Pathology and current treatment concepts of acute spine injuries, Instr Course Lect 21:108, 1972.
- Bosch A, Stauffer ES, Nickel VL: Incomplete traumatic quadriplegia: a ten-year review, JAMA 216:473, 1971.
- Botte MJ, Byrne TP, Abrams RA, et al: Halo skeletal fi xation: techniques of application and prevention of complications, J Am Acad Orthop Surg 4:44, 1996.
- Bracken MB: Methylprednisolone and
