Mastering Regional Anesthesia: Comprehensive Guide to Ankle and Popliteal Sciatic Nerve Blocks
Key Takeaway
The ankle block is a fundamental regional anesthesia technique providing comprehensive coverage for foot and ankle surgery. By systematically targeting the tibial, deep peroneal, superficial peroneal, sural, and saphenous nerves, surgeons can achieve profound intraoperative anesthesia and extended postoperative analgesia. This guide details the precise anatomical landmarks, injection techniques, and evidence-based protocols required to maximize block efficacy while minimizing neurovascular complications.
Introduction to Regional Anesthesia in Foot and Ankle Surgery
Regional anesthesia has revolutionized the perioperative management of foot and ankle pathology. For orthopedic surgeons, mastering the ankle block and the popliteal sciatic nerve block is essential for providing optimal intraoperative conditions, minimizing the need for general anesthesia, and delivering superior postoperative analgesia. These techniques facilitate early discharge in ambulatory settings, reduce opioid consumption, and significantly improve patient satisfaction scores.
An ankle block provides anesthesia to the entire foot by targeting the five terminal branches of the sciatic and femoral nerves at the level of the malleoli. Conversely, the popliteal sciatic nerve block provides broader coverage, anesthetizing the distal two-thirds of the lower extremity (excluding the medial strip innervated by the saphenous nerve), making it ideal for more extensive hindfoot and ankle reconstructions.
This comprehensive academic guide details the precise anatomical landmarks, biomechanical considerations, step-by-step surgical techniques, and evidence-based protocols required to execute these blocks with a high degree of clinical success.
Preoperative Preparation and Pharmacology
Successful regional anesthesia requires meticulous preparation, an understanding of local anesthetic pharmacology, and strict adherence to safety protocols to prevent Local Anesthetic Systemic Toxicity (LAST).
Equipment Selection
- Needles: A 25-gauge or 27-gauge, 1.5-inch needle is typically utilized for the superficial nerves of the ankle block. For the popliteal block, a 21-gauge, 100-mm insulated stimulating needle is preferred.
- Syringes: 10-mL or 20-mL syringes with ring controls allow for precise aspiration and injection.
- Nerve Stimulator: Essential for the popliteal block, set initially at 1.0 to 1.5 mA (2 Hz, 0.1 ms) and dialed down to 0.3 to 0.5 mA to confirm proximity without intraneural placement.
Pharmacologic Agents
The choice of local anesthetic depends on the desired duration of the block:
- Short-to-Medium Acting: 1% or 2% Lidocaine provides rapid onset (5-10 minutes) with a duration of 1 to 2 hours.
- Long-Acting: 0.5% Bupivacaine or 0.5% Ropivacaine provides a slower onset (15-30 minutes) but offers prolonged postoperative analgesia lasting 12 to 24 hours.
- Additives: Epinephrine (1:200,000) may be added to prolong the block and serve as an intravascular marker, though it must be used with extreme caution in patients with peripheral vascular disease to avoid digital ischemia.
💡 Clinical Pearl: Maximum Safe Doses
Always calculate the maximum safe dose based on lean body weight. For Lidocaine without epinephrine, the limit is 4.5 mg/kg; with epinephrine, it is 7 mg/kg. For Bupivacaine, the limit is strictly 2.5 mg/kg.
Surgical Technique: The Ankle Block
The ankle block systematically targets five specific nerves: the tibial, deep peroneal, superficial peroneal, saphenous, and sural nerves. Four of these are terminal branches of the sciatic nerve, while the saphenous nerve is the terminal branch of the femoral nerve.
1. Superficial Peroneal Nerve Block
The superficial peroneal nerve provides sensory innervation to the dorsum of the foot and all toes, except for the first web space and the lateral aspect of the fifth toe.
Anatomical Landmarks:
- Palpate the tip of the lateral malleolus.
- Proceed proximally 8 to 10 cm anterior to the subcutaneous border of the fibular shaft.
Injection Technique:
- At this level, the superficial peroneal nerve has typically penetrated the deep fascia and lies subcutaneously. It may have already divided into its medial and lateral dorsal cutaneous branches.
- Insert the needle subcutaneously and instill 5 to 7 mL of the local anesthetic agent in a fan-like distribution.
- The proximity of the medial and lateral branches to one another ensures that both are effectively anesthetized with this volume of agent.
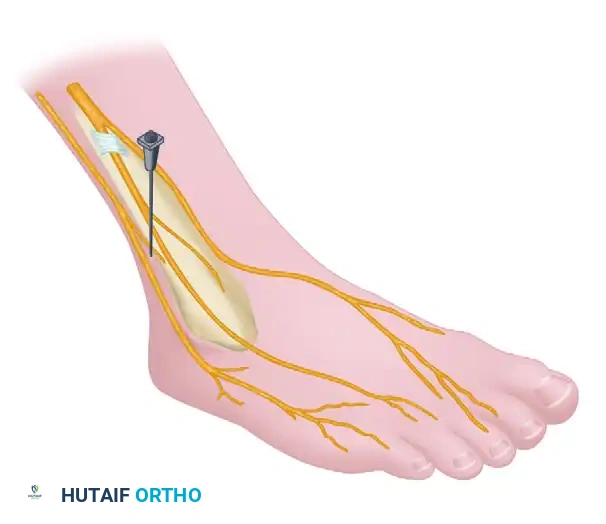
2. Deep Peroneal Nerve Block
The deep peroneal nerve provides sensory innervation to the first dorsal web space and motor innervation to the short extensors of the toes.
Anatomical Landmarks:
- The anterior tibial artery can usually be palpated beneath the superior extensor retinaculum, approximately 4 to 5 cm proximal to the distal articular surface of the tibia.
- The artery and the accompanying deep peroneal nerve lie between the tendons of the anterior tibial (TA) and the extensor digitorum longus (EDL), just lateral to the extensor hallucis longus (EHL), which is situated more deeply. The nerve typically lies just lateral to the artery.
Alternative Landmarks (If Artery is Non-Palpable):
- The tendon of the anterior tibialis is large and lies adjacent to the subcutaneous border of the tibia. Enter the skin just lateral to this tendon. The nerve is located 1 to 1.5 cm deep to the skin.
Injection Technique:
- Advance the needle perpendicular to the skin.
- Carefully aspirate to ensure the anterior tibial artery has not been breached.
- Inject 3 to 5 mL of the anesthetic agent. The fluid should flow freely; if resistance is met, reposition the needle slightly to avoid intraneural or intratendinous injection.
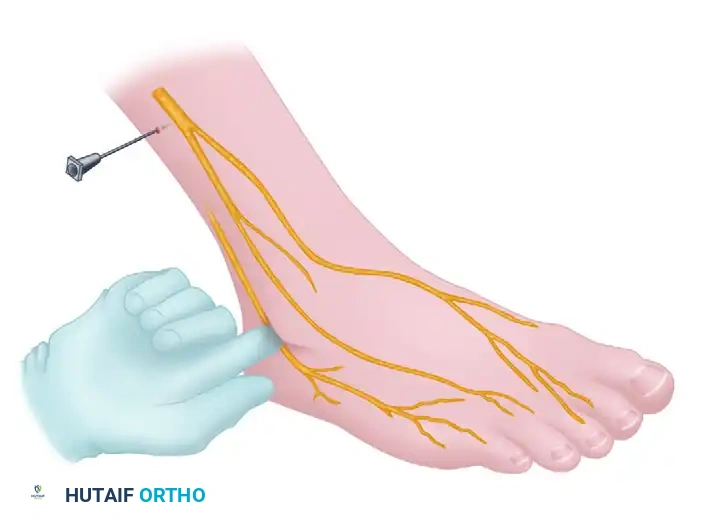
3. Saphenous Nerve Block
The saphenous nerve is the only branch in the ankle block derived from the femoral nerve. It supplies sensation to the medial aspect of the ankle and foot.
Anatomical Landmarks:
- Palpate the tip of the medial malleolus.
- Move 3 to 5 cm proximal to this landmark.
Injection Technique:
- Enter the subcutaneous space, directing the needle anteriorly.
- The saphenous nerve lies just medial or posterior to the great saphenous vein in a slightly deeper fascial plane.
- Aspirate carefully to avoid intravenous injection into the saphenous vein, then inject 2 mL of the anesthetic agent.

4. Sural Nerve Block
The sural nerve provides sensory innervation to the posterolateral aspect of the ankle and the lateral aspect of the foot and fifth toe.
Anatomical Landmarks:
- Palpate the tip of the lateral malleolus.
- At 5 cm proximal to this point, palpate the peroneus longus tendon along the posterior subcutaneous border of the fibula.
Injection Technique:
- The sural nerve passes just anterolateral to the small saphenous vein, approximately halfway between the peroneus longus tendon and the lateral border of the Achilles tendon.
- These two structures usually cross one another behind the lateral malleolus, positioning the nerve posterior to the vein.
- Inject 2 to 3 mL of the solution subcutaneously at this point, utilizing a superficial wheal.

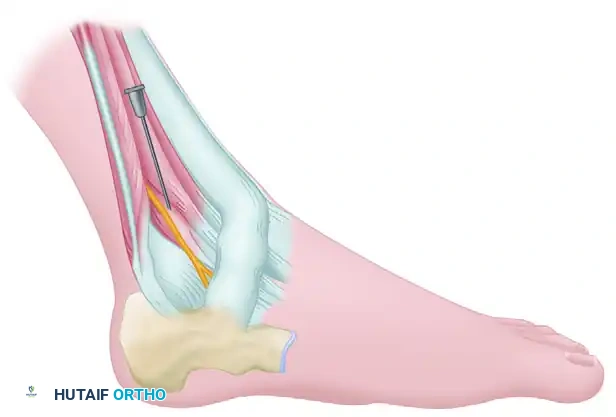
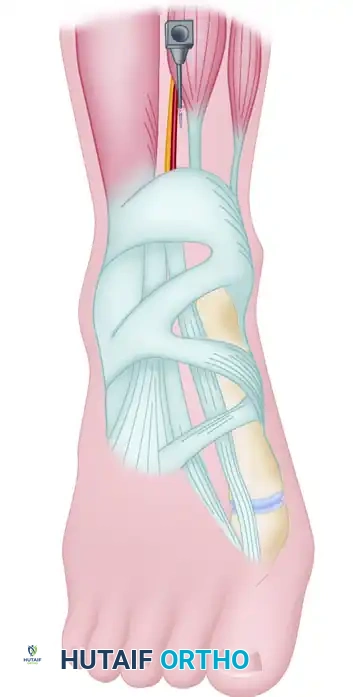
5. Tibial Nerve Block
The tibial nerve is the most critical nerve to block for foot surgery, as it provides sensory innervation to the entire plantar aspect of the foot via its medial and lateral plantar branches. It is also the most technically demanding to block effectively due to its deeper anatomical position beneath the flexor retinaculum.
Anatomical Landmarks:
- Palpate the posteromedial border of the tibia approximately 5 cm proximal to the tip of the medial malleolus.
- Allow the index and middle fingers to slide over the flexor digitorum longus (FDL) and the deeper posterior tibial (PT) tendons. Place a marking pen point of reference at the posterior border of these tendons.
- Palpate the medial border of the Achilles tendon.
- The posterior tibial artery lies halfway between these two points. It is usually palpable at this level and serves as a highly reliable landmark. The nerve lies immediately posterior and lateral to the artery.
Injection Technique:
- Point the needle inferiorly at an angle of about 60 degrees to the skin.
- Penetrate the skin and advance the needle 1 to 1.5 cm until a subtle "pop" is felt as the needle pierces the deep fascia (flexor retinaculum).
- Crucial Step: Aspirate rigorously to ensure the posterior tibial artery or its accompanying venae comitantes have not been entered.
- Instill 8 to 10 mL of the anesthetic agent. The volume is larger here to ensure adequate spread within the neurovascular sheath.
🚨 Surgical Warning: Intravascular Injection
The tibial nerve is intimately bound with the posterior tibial artery and veins within a tight fascial compartment. Aspiration must be performed before every incremental injection of 2-3 mL to definitively rule out intravascular placement.

Surgical Technique: Popliteal Sciatic Nerve Block (Prone)
For more extensive procedures, such as open reduction and internal fixation (ORIF) of ankle fractures, Achilles tendon repairs, or complex hindfoot arthrodesis, the popliteal sciatic nerve block is highly effective. It provides profound intraoperative anesthesia and extended postoperative analgesia.
Clinical Evidence and Efficacy
Extensive literature supports the efficacy of the popliteal block. Provenzano et al. reported on the use of popliteal fossa nerve blocks in 439 patients, noting zero instances of neuralgia, neurapraxia, or other major complications. The overall success rate of the block as a sole anesthetic was 79%; the 92 patients in whom the block was insufficient were seamlessly transitioned to additional local or general anesthesia. Analgesia typically lasts 20 to 24 hours, drastically reducing postoperative opioid requirements. While Chelly et al. described a technique for postoperative pain management with the patient in the supine position, the prone approach remains the gold standard for anatomical clarity.
Anatomical Landmarks
- The popliteal fossa is bounded superolaterally by the biceps femoris and superomedially by the semimembranosus and semitendinosus muscles.
- The sciatic nerve typically bifurcates into the tibial and common peroneal nerves at the apex of the popliteal fossa, roughly 7 to 10 cm proximal to the popliteal crease.
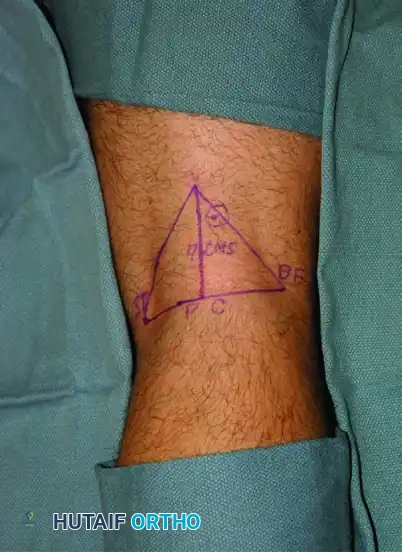
Marking the Patient:
- Outline the popliteal triangle.
- Draw a line through the popliteal crease.
- Draw a perpendicular line bisecting the crease and extending proximally.
- The injection site is typically 7 cm proximal to the crease and 1 cm lateral to the midline.
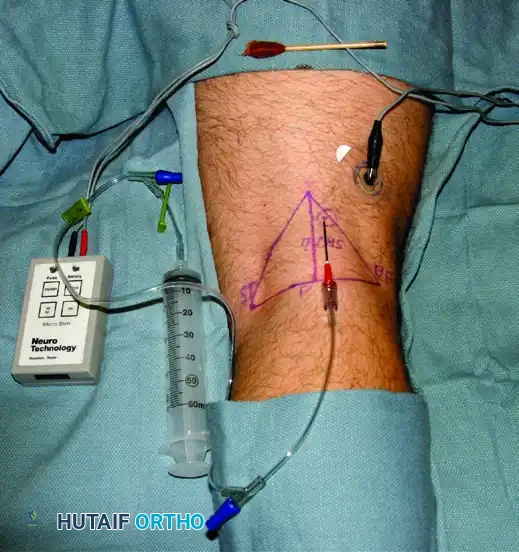
Injection Technique with Nerve Stimulation
Whether the block is administered intraoperatively or postoperatively, the use of a peripheral nerve stimulator significantly improves success rates by ensuring precise needle placement relative to the nerve sheath.
- Positioning: Place the patient in the prone position with the knee slightly flexed to relax the hamstring tendons.
- Stimulator Setup: Attach the grounding electrode to the patient's calf. Connect the insulated needle to the stimulator, initially set at 1.0 to 1.5 mA.
- Needle Insertion: Insert the needle at a 45-degree angle directed anteriorly and slightly superiorly.
- Eliciting a Response: Advance the needle until a motor response is elicited.
- Plantar flexion and inversion indicate stimulation of the tibial nerve component.
- Dorsiflexion and eversion indicate stimulation of the common peroneal nerve component.
- Refining Position: Once a twitch is observed, dial the current down. A persistent twitch at 0.3 to 0.5 mA confirms optimal needle placement adjacent to the nerve. If the twitch persists below 0.2 mA, the needle may be intraneural; withdraw slightly to prevent nerve injury.
- Injection: After negative aspiration, inject 20 to 30 mL of long-acting local anesthetic (e.g., 0.5% Ropivacaine) in 5 mL increments. The motor twitch should fade immediately upon injection as the fluid displaces the nerve from the needle tip.
💡 Clinical Pearl: The "Double Twitch" Technique
To maximize the success of the popliteal block, some advanced practitioners utilize a double-injection technique. After locating and blocking the tibial component, the needle is withdrawn slightly and redirected laterally to independently stimulate and block the common peroneal component. This ensures circumferential spread around both major divisions before they fully separate.
Postoperative Protocols and Complication Management
Postoperative Care
Patients receiving long-acting regional blocks must be educated regarding the expected duration of sensory and motor blockade.
- Weight-Bearing: Patients with a dense popliteal block will lack proprioception and motor control of the foot and ankle. Strict non-weight-bearing protocols or the use of a controlled ankle motion (CAM) boot and crutches are mandatory to prevent falls and inadvertent injury to the insensate limb.
- Rebound Pain: The transition from a dense block to normal sensation can cause sudden, severe "rebound pain." Multimodal oral analgesics (acetaminophen, NSAIDs, and a short course of oral opioids) should be initiated before the block completely wears off.
Recognizing and Managing Complications
While regional anesthesia is overwhelmingly safe, surgeons must be vigilant for potential complications:
1. Intravascular Injection (LAST): Symptoms include perioral numbness, tinnitus, metallic taste, agitation, and in severe cases, seizures and cardiovascular collapse. Immediate management includes airway support, seizure control, and the rapid administration of 20% Intravenous Lipid Emulsion (Intralipid).
2. Nerve Injury: Intraneural injection or direct needle trauma can lead to prolonged neurapraxia or permanent neuropathy. Always avoid injecting if high resistance is met or if the patient reports severe, sharp, radiating pain during injection (paresthesia).
3. Hematoma: Given the proximity of the nerves to major vessels (especially the posterior tibial and anterior tibial arteries), hematoma formation is a risk, particularly in anticoagulated patients. Firm pressure should be applied to any arterial puncture site for a minimum of 5 minutes.
Conclusion
The ankle block and popliteal sciatic nerve block are indispensable tools in the armamentarium of the modern orthopedic surgeon. By combining a profound understanding of cross-sectional anatomy with meticulous technique and modern adjuncts like nerve stimulation, surgeons can consistently achieve excellent regional anesthesia. This not only optimizes the surgical environment but fundamentally enhances the patient's postoperative recovery trajectory.
📚 Medical References
- ankle block anesthesia for foot surgery, Foot Ankle 13:344, 1992.
- Michelson JD, Perry M: Clinical safety and effi cacy of calf tourniquets, Foot Ankle Int 17:573, 1996.
- Mizel MS, Temple HT, Michelson JD, et al: Thromboembolism after foot and ankle surgery: a multicenter study, Clin Orthop Relat Res 348:180, 1998.
- Provenzano DA, Viscusi ER, Adams SB Jr, et al: Safety and effi cacy of the popliteal fossa nerve block when utilized for foot and ankle surgery, Foot Ankle Int 23:394, 2002.
- Reyes C, Barnauskas S, Hetherington V: Retrospective assessment of antibiotic and tourniquet use in an ambulatory surgery center, J Foot Ankle Surg 36:55, 1997.
- Rongstad K, Mann RA, Prieskorn D, et al: Popliteal
You Might Also Like


