Amputations of the Hip and Pelvis: A Comprehensive Surgical Guide
Amputations at the level of the hip and pelvis represent some of the most challenging and functionally debilitating procedures in orthopaedic surgery. These major limb ablations, including hip disarticulation and various forms of hemipelvectomy, are typically reserved for severe pathologies where limb salvage is either oncologically unsound, functionally impossible, or life-threatening. The primary indications are often aggressive musculoskeletal tumors, but they may also be necessitated by overwhelming trauma, intractable infection, or severe vascular compromise.
The decision to proceed with such a radical amputation is never taken lightly, requiring a multidisciplinary approach involving orthopaedic oncology, vascular surgery, infectious disease specialists, plastic surgeons, and rehabilitation teams. While significant advancements have been made in prosthetic technology, the functional outcomes following these high-level amputations remain challenging, and patient adaptation is highly variable. This chapter provides a detailed, evidence-based overview of hip disarticulation and hemipelvectomy, focusing on indications, biomechanics, surgical techniques, and comprehensive postoperative management.
Hip Disarticulation
Hip disarticulation involves the complete removal of the lower extremity through the hip joint, leaving the pelvis intact. This procedure results in the loss of the entire limb, including the femur, tibia, and foot.
Indications for Hip Disarticulation
Hip disarticulation is a definitive surgical option for conditions that preclude more distal amputation or limb salvage. The most common indications include:
- Oncological Conditions:
- High-grade bone or soft-tissue sarcomas of the proximal femur or thigh that cannot be adequately resected with limb-sparing techniques while achieving clear surgical margins.
- Recurrent tumors after previous limb-sparing surgery.
- Extensive local tumor invasion involving neurovascular structures or the hip joint capsule.
- Massive Trauma:
- Severe crush injuries or avulsion injuries of the proximal thigh and hip that result in irreparable damage to bone, soft tissue, and neurovascular structures, often complicated by infection or significant tissue loss.
- Traumatic amputations at or near the hip joint.
- Infection:
- Fulminant, necrotizing fasciitis extending into the hip region.
- Uncontrolled osteomyelitis of the proximal femur or hip joint, particularly in immunocompromised patients or those with failed previous treatments.
- Infected nonunions of the subtrochanteric or intertrochanteric femur with extensive soft tissue involvement.
- Vascular Insufficiency:
- Severe, unreconstructable arterial insufficiency leading to gangrene of the entire lower limb, especially when associated with proximal infection or tissue loss.
- Congenital Limb Deficiencies:
- Rarely, for severe congenital anomalies where the limb is non-functional, painful, or poses significant management challenges.
Clinical Pearl: In oncological cases, the primary goal is always complete tumor excision with clear margins. The choice of amputation level and flap design must prioritize oncological safety over reconstructive convenience. Preoperative imaging (MRI, CT, PET) is crucial for precise tumor mapping.
Contraindications
Absolute contraindications are few and typically relate to the patient's overall medical status:
- Uncontrolled sepsis.
- Severe cardiac or pulmonary comorbidities precluding major surgery.
- Metastatic disease with a very limited life expectancy where the procedure would not improve quality of life.
- Inadequate skin or soft tissue for flap closure, though this can often be managed with creative flap design or reconstructive techniques.
Biomechanics and Functional Implications
The loss of the entire lower limb at the hip joint has profound biomechanical consequences:
- Loss of Weight-Bearing: The primary weight-bearing function of the limb is lost, necessitating reliance on crutches, a wheelchair, or a specialized prosthesis.
- Loss of Pelvic Stability: The muscular attachments around the hip (gluteals, iliopsoas, adductors) are crucial for pelvic stability during gait. Their loss significantly compromises balance and trunk control.
- Prosthetic Challenges: Hip disarticulation prostheses are complex, heavy, and often uncomfortable. They typically incorporate a pelvic bucket, a mechanical hip joint, a knee joint, and a foot. The lack of a bony lever arm (femur) makes prosthetic control difficult, often relying on trunk movements to initiate swing phase. Few patients achieve a truly functional gait with these prostheses, often preferring crutches or wheelchairs for mobility.
Preoperative Planning
Meticulous preoperative planning is essential:
- Patient Assessment: Comprehensive medical evaluation to optimize comorbidities. Nutritional status, psychological readiness, and social support are critical.
- Imaging: MRI for soft tissue and tumor extent, CT for bone involvement and surgical planning, angiography for vascular assessment if indicated.
- Anesthesia: General anesthesia is standard. Epidural or spinal anesthesia can be used for postoperative pain control.
- Blood Management: Significant blood loss is anticipated. Type and cross-match for at least 4-6 units of packed red blood cells. Cell saver may be considered.
- Informed Consent: Thorough discussion of the procedure, potential complications, functional limitations, and prosthetic options. Psychological counseling is often beneficial.
Patient Positioning
- Lateral Decubitus Position: Often preferred, allowing access to both anterior and posterior aspects of the hip without repositioning. The affected side is uppermost.
- Supine Position with Draping for Lateral Access: Can be used, but requires careful draping to allow for significant limb manipulation and access to the posterior aspect.
- Lithotomy Position (Modified): Rarely used, but can provide excellent perineal access if required for specific tumor resections.
Surgical Warning: Ensure adequate padding of pressure points, especially the contralateral limb and axilla, to prevent nerve palsies or skin breakdown during prolonged surgery.
Surgical Approaches for Hip Disarticulation
Two classic techniques are described: the anatomical method of Boyd and the posterior flap method of Slocum. Modifications are frequently required based on the pathology's location and extent, particularly in oncological cases where clear margins dictate flap design.
Technique 12-1: Boyd's Anatomical Hip Disarticulation
This technique emphasizes an anterior racquet-shaped incision, providing excellent exposure to the major neurovascular structures and allowing for systematic muscle division.
-
1. Incision:
- Begin the anterior racquet-shaped incision at the anterior superior iliac spine (ASIS).
- Curve it distally and medially, running almost parallel to the inguinal ligament, to a point on the medial aspect of the thigh approximately 5 cm distal to the origin of the adductor muscles.
- Continue the incision around the posterior aspect of the thigh, about 5 cm distal to the ischial tuberosity.
- Extend it along the lateral aspect of the thigh, approximately 8 cm distal to the base of the greater trochanter.
- From this point, curve the incision proximally to join its beginning just inferior to the ASIS.
- Refer to the inset in Fig. 12-1A for the line of skin incision.
-
2. Anterior Dissection and Neurovascular Ligation:
- Deepen the anterior incision through the subcutaneous tissue and fascia.
- Identify and isolate the femoral artery and vein within the femoral triangle. Double ligate and divide these vessels.
- Identify and divide the femoral nerve, allowing it to retract proximally.
- This step is depicted in Fig. 12-1A, showing the ligated femoral vessels and nerve.
-
3. Muscle Detachment (Anterior and Medial):
- Detach the sartorius muscle from the ASIS and the rectus femoris muscle from the anterior inferior iliac spine (AIIS). Reflect both muscles distally.
- Divide the pectineus muscle approximately 0.6 cm from its origin on the pubis.
- Externally rotate the thigh to bring the lesser trochanter and the iliopsoas tendon into view. Divide the iliopsoas tendon at its insertion on the lesser trochanter and reflect it proximally.
- Detach the adductor longus, adductor brevis, and gracilis muscles from their origins on the pubis.
- Divide the part of the adductor magnus muscle that arises from the ischium at its origin.
- These initial muscle detachments are shown in Fig. 12-1A.
-
4. Obturator Neurovascular Bundle:
- Develop the muscle plane between the pectineus and obturator externus, and the short external rotators of the hip. This exposes the branches of the obturator artery.
- Clamp, ligate, and divide these branches at this point.
- Crucial Note: The obturator externus muscle is divided at its insertion on the femur later in the operation, rather than at its origin on the pelvis. Dividing it at its origin early could sever the obturator artery, leading to hemorrhage that might retract into the pelvis and be difficult to control.
-
5. Lateral and Posterior Dissection:
- Internally rotate the thigh.
- Detach the gluteus medius and minimus muscles from their insertions on the greater trochanter and retract them proximally.
- Divide the fascia lata and the most distal fibers of the gluteus maximus muscle distal to the insertion of the tensor fasciae latae, following the line of the skin incision.
- Separate the tendon of the gluteus maximus from its insertion on the linea aspera. Reflect this muscle mass proximally.
- Identify, ligate, and divide the sciatic nerve, allowing it to retract proximally.
- Divide the short external rotators of the hip (piriformis, gemelli superior and inferior, obturator internus, obturator externus, and quadratus femoris) at their insertions on the femur.
- Sever the hamstring muscles (semitendinosus, semimembranosus, biceps femoris) from the ischial tuberosity.
- These posterior muscle divisions and sciatic nerve ligation are depicted in Fig. 12-1B.
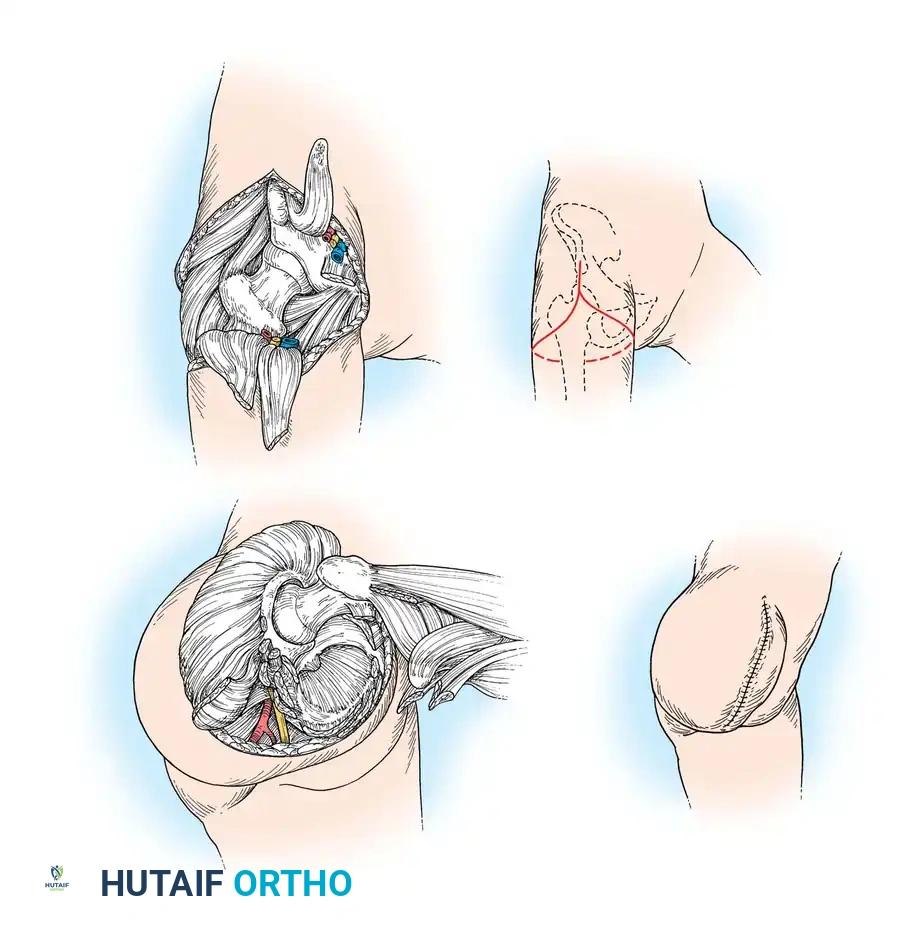
Fig. 12-1 Boyd disarticulation of hip. A, Femoral vessels and nerve have been ligated, and sartorius, rectus femoris, pectineus, and iliopsoas muscles have been detached. Inset, Line of skin incision. B, Gluteal muscles have been separated from insertions, sciatic nerve and short external rotators have been divided, and hamstring muscles have been detached from ischial tuberosity. Inset, Final closure of stump. (Redrawn from Boyd HB: Anatomic disarticulation of the hip, Surg Gynecol Obstet 84:346, 1947.) -
6. Joint Disarticulation:
- Incise the hip joint capsule circumferentially.
- Divide the ligamentum teres to complete the disarticulation of the femoral head from the acetabulum.
-
7. Wound Closure:
- Achieve meticulous hemostasis.
- Bring the gluteal flap anteriorly. Suture the distal part of the gluteal muscles (primarily gluteus maximus) to the origins of the pectineus and adductor muscles on the pubis and ischium. This provides a muscular cushion over the acetabulum.
- Place a suction drain in the inferior part of the incision to prevent hematoma formation.
- Approximate the skin edges with interrupted nonabsorbable sutures.
- The final closure of the stump is shown in the inset of Fig. 12-1B.
Technique 12-2: Slocum's Posterior Flap Method
The Slocum technique utilizes a long posteromedial flap, often providing better soft tissue coverage, particularly useful when anterior tissue is compromised.
-
1. Incision:
- Begin the incision at the level of the inguinal ligament, carrying it distally over the femoral artery for approximately 10 cm.
- Curve it along the medial aspect of the thigh, then continue it laterally and proximally over the greater trochanter.
- Swing it anteriorly to meet the starting point at the inguinal ligament.
- This design creates a long posteromedial flap, which will be used to cover the end of the stump.
-
2. Anterior Neurovascular Ligation:
- Isolate, double ligate, and divide the femoral artery and vein.
- Section the femoral nerve, allowing it to retract well proximal to the inguinal ligament to prevent neuroma formation in a pressure area.
-
3. Medial and Anterior Muscle Division:
- Abduct the thigh widely. Divide the adductor muscles (longus, brevis, magnus) at their pubic origins.
- Section the two branches of the obturator nerve, ensuring they retract away from potential pressure areas on the stump.
- Free the origins of the sartorius from the ASIS and the rectus femoris from the AIIS.
-
4. Lateral and Posterior Muscle Division:
- Moderately adduct and internally rotate the thigh.
- Divide the tensor fasciae latae at the level of the proximal end of the greater trochanter.
- At the same level, divide the muscles attached to the greater trochanter (gluteus medius, gluteus minimus, short external rotators) close to the bone.
- Markedly abduct the thigh. Divide the gluteus maximus muscle at the distal end of the posterior skin flap.
- Identify, ligate, and divide the sciatic nerve.
-
5. Joint Disarticulation:
- Divide the hip joint capsule circumferentially.
- Divide the ligamentum teres to complete the disarticulation.
-
6. Wound Closure:
- Achieve meticulous hemostasis.
- Swing the long posteromedial flap, containing the gluteus maximus muscle, anteriorly.
- Suture this flap to the anterior margins of the incision, providing robust soft tissue coverage over the acetabulum.
- Place a suction drain.
- Close the skin with interrupted nonabsorbable sutures.
Surgical Pitfall: In oncological cases, the standard flap designs may need significant modification. The primary concern is achieving clear tumor margins. This may necessitate sacrificing ideal flap aesthetics or even requiring skin grafting if local tissue is insufficient after radical resection.
Postoperative Management
Postoperative care is critical for wound healing, pain control, and early rehabilitation.
- Pain Management:
- Multimodal analgesia, including epidural catheters, regional nerve blocks, intravenous opioids, and non-opioid analgesics.
- Management of phantom limb pain, which can be severe and debilitating, often requiring gabapentinoids or tricyclic antidepressants.
- Wound Care:
- Regular wound inspection for signs of infection, dehiscence, or hematoma.
- Drains are typically removed when output is minimal (<30-50 mL/24 hours).
- Strict hygiene to prevent wound contamination, especially given the proximity to the perineum.
- Deep Vein Thrombosis (DVT) Prophylaxis:
- Pharmacological prophylaxis (low molecular weight heparin or unfractionated heparin) combined with mechanical prophylaxis (sequential compression devices) is essential due to the high risk of DVT/PE.
- Early Mobilization:
- As soon as pain is controlled and hemodynamic stability is achieved, encourage upper body strengthening and transfer training.
- Physical therapy focuses on core strength, balance, and independent transfers.
- Rehabilitation and Prosthetics:
- Referral to a specialized rehabilitation team is paramount.
- Prosthetic fitting typically begins several weeks to months post-surgery, once the wound is fully healed and stable.
- Patients require extensive training to use a hip disarticulation prosthesis effectively. Many find them cumbersome and opt for wheelchair mobility for longer distances.
Complications
- Wound Complications: Hematoma, seroma, infection, dehiscence, skin flap necrosis.
- Neuroma Formation: At the ends of divided nerves (femoral, sciatic, obturator).
- Phantom Limb Pain: Common and challenging to manage.
- Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE): High risk due to extensive dissection and immobility.
- Heterotopic Ossification: Can occur around the acetabulum.
- Psychological Distress: Depression, anxiety, body image issues.
- Functional Limitations: Significant challenges with mobility and activities of daily living.
Hemipelvectomy
Hemipelvectomy, also known as hindquarter amputation, is a more extensive procedure involving the removal of the entire lower extremity along with a portion of the ipsilateral pelvis. This procedure is almost exclusively performed for aggressive pelvic or proximal thigh tumors.
Definition and Scope
Hemipelvectomy involves resection of the lower limb and a segment of the bony pelvis. It is classified based on the extent of pelvic bone resection:
- External Hemipelvectomy (Classic): Resection of the entire lower limb and a portion of the ilium, ischium, and pubis, resulting in a significant defect in the pelvic ring.
- Internal Hemipelvectomy: Resection of a portion of the pelvic bone without removal of the lower extremity. This is a limb-sparing procedure and distinct from the ablative hemipelvectomy discussed here.
- Types of External Hemipelvectomy:
- Posterior (Sacroiliac) Hemipelvectomy: Resection through the sacroiliac joint and pubic symphysis.
- Anterior (Pubic) Hemipelvectomy: Resection through the ilium posterior to the sacroiliac joint and anteriorly through the pubic symphysis.
- Total Hemipelvectomy: Resection of the entire ipsilateral hemipelvis, including the sacrum, often requiring extensive abdominal and urological reconstruction.
Indications for Hemipelvectomy
The primary indication for external hemipelvectomy is aggressive malignancy:
- Oncological Conditions:
- Primary bone sarcomas (e.g., chondrosarcoma, osteosarcoma, Ewing sarcoma) of the ilium, ischium, or pubis that are unresectable by limb-sparing techniques.
- Extensive soft-tissue sarcomas of the gluteal region or proximal thigh with direct invasion of the pelvic bone.
- Recurrent pelvic tumors after previous surgery or radiation.
- Metastatic disease to the pelvis causing intractable pain or impending pathological fracture, where other palliative measures have failed.
- Rarely for Trauma or Infection: Extremely severe, life-threatening trauma or overwhelming infection involving the pelvic bone and soft tissues, where no other option exists.
Contraindications
Similar to hip disarticulation, but with even greater emphasis on patient fitness:
- Uncontrolled sepsis or severe systemic infection.
- Prohibitive medical comorbidities.
- Extensive metastatic disease with very poor prognosis, where the morbidity of surgery outweighs potential benefits.
- Inability to achieve clear surgical margins due to extensive tumor involvement of vital structures (e.g., contralateral iliac vessels, sacral nerve roots, bladder, rectum) that cannot be resected.
Biomechanics and Functional Implications
Hemipelvectomy leads to profound functional deficits:
- Loss of Pelvic Ring Integrity: The removal of a portion of the pelvic ring results in significant instability, making sitting and transfers challenging.
- Trunk Instability: Loss of the ipsilateral abdominal and gluteal musculature severely compromises trunk control and balance.
- Weight-Bearing: Direct weight-bearing on the remaining pelvic rim is often painful and difficult.
- Prosthetic Limitations: Standard prostheses are even less functional than for hip disarticulation. Patients often rely on custom-molded bucket prostheses that encompass the remaining pelvis, providing some support for sitting and limited ambulation. Many patients prefer wheelchair mobility.
Preoperative Planning
Preoperative planning for hemipelvectomy is even more complex than for hip disarticulation:
- Multidisciplinary Team: Essential involvement of orthopaedic oncology, general surgery (for bowel/bladder involvement), urology, vascular surgery, plastic surgery, and anesthesia.
- Extensive Imaging: High-resolution MRI and CT scans with contrast are crucial for defining tumor extent, vascular involvement, and bony resection margins. Angiography may be necessary.
- Biopsy: Preoperative biopsy is mandatory to confirm tumor type and guide treatment.
- Bowel and Bladder Preparation: If bowel or bladder resection is anticipated, appropriate preoperative preparation is required.
- Blood Management: Anticipate massive blood loss. Pre-donation of autologous blood, cell saver, and availability of significant blood products are mandatory.
- Psychological Support: Intensive counseling for the patient and family regarding the radical nature of the surgery and its profound functional impact.
Patient Positioning
- Lateral Decubitus Position: Most common, allowing access to the anterior, lateral, and posterior aspects of the pelvis and limb.
- Combined Supine and Lateral: May be necessary for very extensive resections or if abdominal access is required.
Surgical Approaches for Hemipelvectomy
The specific surgical approach and incision depend entirely on the tumor's location and extent, aiming for clear oncological margins. The following describes general principles and common steps.
-
1. Incision:
- The skin incision is highly individualized. It typically involves a large flap designed to provide adequate coverage of the remaining pelvic structures while ensuring clear margins around the tumor.
- Commonly, an anterior limb of the incision extends from the iliac crest, curving inferiorly and medially towards the groin, then sweeping posteriorly to encompass the entire limb and a portion of the gluteal region.
- The posterior limb may extend along the sacrum or posterior iliac crest.
-
2. Neurovascular Ligation:
- The major vessels (external iliac artery and vein, or common iliac vessels if more proximal) are identified, double ligated, and divided. This is often performed early to minimize blood loss.
- The femoral nerve, sciatic nerve, and obturator nerve are identified and divided proximally, allowing for retraction.
-
3. Muscle and Soft Tissue Dissection:
- Systematic division of muscles originating from the pelvis:
- Anterior: Rectus abdominis, external and internal obliques, transversus abdominis, iliopsoas.
- Medial: Adductor muscles, pectineus, gracilis.
- Lateral: Tensor fasciae latae, gluteus medius, gluteus minimus.
- Posterior: Gluteus maximus, piriformis, short external rotators, hamstrings.
- Careful dissection around the bladder, rectum, and ureter, especially if tumor involvement is suspected.
- Systematic division of muscles originating from the pelvis:
-
4. Bony Resection:
- The specific osteotomies depend on the type of hemipelvectomy (posterior, anterior, total) and tumor extent.
- Posterior Hemipelvectomy:
- Disarticulation of the pubic symphysis.
- Osteotomy through the ilium or disarticulation through the sacroiliac joint. This requires careful identification and protection of the lumbosacral plexus and contralateral sacral nerve roots.
- Anterior Hemipelvectomy:
- Osteotomy through the ilium posterior to the sacroiliac joint.
- Disarticulation of the pubic symphysis.
- Total Hemipelvectomy:
- Resection of the entire ipsilateral hemipelvis, potentially including a portion of the sacrum. This is a highly complex procedure with significant risk to the lumbosacral plexus and contralateral pelvic structures.
- Bone cuts are typically made with an oscillating saw, ensuring clear margins.
-
5. Specimen Removal:
- Once all soft tissue and bony attachments are divided, the entire limb and resected pelvic segment are removed en bloc.
-
6. Wound Closure:
- Meticulous hemostasis is paramount.
- The remaining soft tissues are mobilized to provide coverage for the exposed pelvic raw surfaces. This often involves rotating large muscle flaps (e.g., contralateral gluteus maximus, rectus abdominis, or even free flaps) to fill the defect and provide padding.
- The skin flaps are approximated, often under significant tension.
- Multiple large suction drains are placed.
- The skin is closed with interrupted nonabsorbable sutures.
Surgical Warning: Hemipelvectomy carries a very high risk of massive hemorrhage. Preoperative embolization of feeding vessels may be considered in highly vascular tumors. Intraoperative blood loss can exceed 10-15 liters.
Postoperative Management
Postoperative management is intensive and prolonged.
- Intensive Care Unit (ICU) Stay: Often required for initial hemodynamic stabilization, pain control, and close monitoring.
- Pain Management: Aggressive multimodal pain control, including epidural analgesia, nerve blocks, and systemic medications. Phantom limb pain is common.
- Wound Care: Extensive wound care is needed due to the large raw surface and potential for flap necrosis, infection, or dehiscence. Negative pressure wound therapy may be beneficial.
- Fluid and Electrolyte Management: Careful monitoring and replacement due to large fluid shifts and blood loss.
- DVT Prophylaxis: Aggressive pharmacological and mechanical prophylaxis.
- Bowel and Bladder Management: Temporary urinary catheters and nasogastric tubes are common. Bowel function needs careful monitoring, especially if bowel resection was performed.
- Rehabilitation: Begins early with bed mobility, upper body strengthening, and transfer training. Patients will require a wheelchair for primary mobility. Prosthetic options are very limited and often serve primarily for cosmesis or sitting balance.
Complications
Hemipelvectomy has a high rate of significant complications:
- Massive Hemorrhage: Intraoperative and postoperative.
- Wound Complications: Infection, dehiscence, flap necrosis, seroma, hematoma.
- Nerve Injury: To the contralateral lumbosacral plexus or sacral nerve roots.
- Urological Complications: Ureteric injury, bladder dysfunction, fistula formation.
- Bowel Complications: Bowel injury, fistula formation, ileus.
- Pelvic Instability: Significant functional impairment.
- Phantom Limb Pain: Highly prevalent and often severe.
- Psychological Distress: Profound impact on body image, self-esteem, and quality of life.
- Mortality: Higher than for hip disarticulation due to the magnitude of the surgery.
Prosthetic Considerations and Rehabilitation
For both hip disarticulation and hemipelvectomy, prosthetic fitting presents significant challenges.
- Hip Disarticulation Prostheses: These are typically Canadian-type prostheses, consisting of a rigid pelvic socket that encompasses the iliac crests, a mechanical hip joint, a knee joint, and a prosthetic foot.
- Challenges: Heavy, cumbersome, difficult to don and doff, limited control due to absence of a bony lever arm, often requiring significant trunk motion for gait initiation.
- Outcomes: While some highly motivated individuals achieve limited community ambulation, many find these prostheses too demanding and prefer crutches or wheelchairs for primary mobility.
- Hemipelvectomy Prostheses: Even more challenging due to the loss of pelvic
