Introduction & Epidemiology
Acromioclavicular (AC) joint injuries are common pathologies encountered in orthopedic practice, comprising approximately 9% of all shoulder girdle injuries and up to 40% of all shoulder injuries. These injuries typically result from direct trauma to the superior aspect of the acromion, often with the arm adducted, driving the scapula inferiorly relative to the clavicle. This mechanism is frequently observed in contact sports (e.g., football, rugby, hockey), cycling accidents, and falls.
The severity of AC joint injuries is most widely classified using the Rockwood classification system, which categorizes injuries into six types based on the degree of ligamentous disruption and displacement of the clavicle relative to the acromion.
*
Type I:
Sprain of the AC ligaments without complete tear; joint remains stable.
*
Type II:
Complete tear of the AC ligaments, but intact coracoclavicular (CC) ligaments; mild superior subluxation of the clavicle (<25% CC distance).
*
Type III:
Complete tears of both AC and CC ligaments; clavicle significantly displaced superiorly, typically 25-100% increased CC distance.
*
Type IV:
Complete tears of AC and CC ligaments; clavicle displaced posteriorly into or through the trapezius muscle.
*
Type V:
Complete tears of AC and CC ligaments, with severe superior displacement of the clavicle, often exceeding 100% of CC distance, and detachment of deltoid and trapezius fascia.
*
Type VI:
Extremely rare; complete tears of AC and CC ligaments with inferior displacement of the clavicle beneath the coracoid process or acromion.
The incidence of AC joint injuries shows a bimodal distribution, with peaks in young, active males involved in sports and in older individuals due to falls. While Type I and II injuries often respond to non-operative management, Type III injuries remain controversial, and Type IV, V, and VI injuries generally necessitate surgical intervention due to significant instability, cosmetic deformity, and functional impairment.
Surgical Anatomy & Biomechanics
A thorough understanding of the AC joint's intricate anatomy and biomechanics is paramount for effective diagnosis and treatment of its injuries. The AC joint is a diarthrodial joint stabilized by both static and dynamic restraints.
Static Stabilizers
- Acromioclavicular (AC) Ligaments: These ligaments include superior, inferior, anterior, and posterior bundles. The superior AC ligament is the strongest and most consistently defined, providing primary horizontal stability and resisting posterior translation of the clavicle. The AC ligaments primarily limit anterior-posterior translation and axial rotation of the clavicle on the acromion.
-
Coracoclavicular (CC) Ligaments:
These are extra-articular ligaments crucial for vertical stability, connecting the coracoid process of the scapula to the inferior aspect of the clavicle. They consist of two distinct fascicles:
- Conoid Ligament: Medial and conical, originating from the posteromedial base of the coracoid and inserting onto the conoid tubercle of the clavicle. It resists superior translation and posterior rotation of the clavicle.
-
Trapezoid Ligament:
Lateral and quadrilateral, originating from the superior surface of the coracoid and inserting onto the trapezoid line on the undersurface of the clavicle. It resists superior translation and posterior rotation of the clavicle, and limits anterior translation.
The combined CC ligaments primarily prevent superior displacement of the clavicle relative to the acromion and limit excessive clavicular rotation. The distance from the superior aspect of the coracoid to the inferior aspect of the clavicle, typically 11-13 mm, is a critical radiographic measurement.
- Articular Capsule: A fibrous capsule surrounds the joint, reinforced by the AC ligaments.
- Articular Disc (Meniscus): A small, often degenerated, fibrocartilaginous disc may be present within the joint, acting as a partial shock absorber and incongruity filler, though its functional significance diminishes with age.
Dynamic Stabilizers
The deltoid and trapezius muscles, which originate from and insert onto the distal clavicle and acromion, provide dynamic stability. Their fascial attachments, particularly the deltotrapezial fascia, are critical in maintaining reduction following injury, especially in Rockwood Type V injuries where these fascial attachments are severely disrupted.
Biomechanics of Injury
Trauma to the AC joint typically involves an impact that drives the acromion inferiorly, resulting in a sequential failure of the supporting structures:
*
Type I:
Sprain of the AC ligaments, capsule intact.
*
Type II:
Complete tear of the AC ligaments and capsule, CC ligaments intact. This allows mild superior clavicular displacement and anterior-posterior instability.
*
Type III:
Complete tear of both AC and CC ligaments. This leads to significant vertical instability, loss of normal AC joint alignment, and disruption of the deltotrapezial fascia. The clavicle migrates superiorly due to unopposed sternocleidomastoid pull.
*
Type IV, V, VI:
These represent progressive severity of Type III injuries with additional vectors of displacement (posterior into trapezius, gross superior displacement with extensive fascial stripping, or inferior displacement).
The CC ligaments are the primary restraints to superior clavicular displacement, contributing 60-80% of vertical stability. The AC ligaments provide the remaining vertical stability and are the primary restraints to anterior-posterior translation. Disruption of both sets of ligaments leads to multidirectional instability and symptomatic shoulder dysfunction.
Indications & Contraindications
The decision-making process for AC joint injuries is nuanced, particularly for Rockwood Type III injuries, and involves consideration of patient factors, activity level, functional demands, and the specific injury pattern.
Operative vs. Non-Operative Indications
| Indication Type | Rockwood Classification | Key Considerations |
|---|---|---|
| Non-Operative | Type I | Pain management, sling for comfort, early range of motion (ROM). |
| Type II | Pain management, sling, early ROM. Surgical intervention considered for persistent pain or high-demand overhead athletes failing conservative care. | |
| Type III (Controversial) | Many studies support non-operative management for sedentary individuals or those with low functional demands, demonstrating comparable long-term functional outcomes to operative management, albeit with potential for cosmetic deformity and slight strength deficits. Sling immobilization for 2-4 weeks, followed by progressive rehabilitation. | |
| Operative | Acute Type III | High-demand overhead athletes, laborers, or individuals requiring robust shoulder function. Persistent symptoms (pain, weakness, instability) after a trial of non-operative management. Patients with significant cosmetic concern. |
| Acute Type IV | Clavicle displaced posteriorly into the trapezius, requiring surgical reduction and stabilization due to high risk of functional deficit and potential neurovascular compromise. | |
| Acute Type V | Marked superior displacement (>100% CC distance) with extensive deltotrapezial fascia disruption. Significant cosmetic and functional impairment, consistently managed surgically. | |
| Acute Type VI | Inferior displacement of the clavicle beneath the coracoid or acromion. Extremely rare but necessitates surgical intervention due to severe instability and potential for brachial plexus or subclavian vessel compression. | |
| Chronic Symptomatic AC Instability (Any Type) | Failed non-operative management for Type II or III injuries, presenting with persistent pain, weakness, crepitus, or impingement symptoms related to AC joint instability. | |
| Distal Clavicle Fracture with AC Dislocation | Often requires concomitant management of the fracture and stabilization of the AC joint. |
Absolute Contraindications to Surgery
- Active infection (local or systemic).
- Uncontrolled medical comorbidities that preclude safe anesthesia or surgery (e.g., severe cardiopulmonary disease).
- Severe soft tissue compromise around the shoulder that would prevent wound healing.
- Patient unwilling or unable to comply with post-operative rehabilitation protocols.
Relative Contraindications / Cautions
- Advanced age (relative, depends on functional demands and comorbidity).
- Smoking (increases risk of complications, especially wound healing and infection).
- Poor bone quality (may affect hardware purchase).
- Previous ipsilateral shoulder surgery that complicates access or anatomy.
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is essential to ensure successful surgical outcomes for AC joint injuries.
Imaging
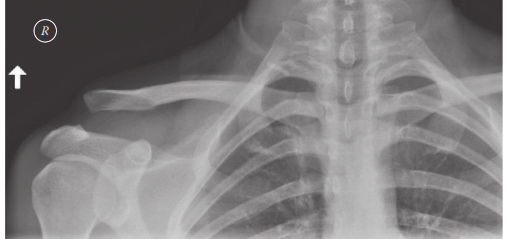
- Plain Radiographs: Anteroposterior (AP), Zanca view (10-15 degrees cephalic tilt, visualizing the AC joint without glenoid overlap), and axillary lateral views are standard. Bilateral stress views (with patient holding 10-15 lb weights) can aid in diagnosing subtle Type II or III injuries by accentuating vertical displacement, though their utility is debated due to discomfort and potential for false positives/negatives. Coracoclavicular distance measurement on AP view is critical.
- MRI: Useful for assessing soft tissue damage (AC/CC ligaments, rotator cuff, labrum) and evaluating for concomitant injuries, especially in chronic cases or when pain is disproportionate to plain film findings. It can differentiate between partial and complete ligament tears.
- CT Scan: Valuable for complex injuries, particularly Type IV (posterior displacement into trapezius) or Type VI (inferior displacement), to delineate the exact position of the clavicle and assess for associated fractures (e.g., coracoid, distal clavicle, scapula). 3D reconstructions are particularly helpful for surgical planning.
Pre-Operative Discussion
Before surgery, a thorough discussion with the patient regarding the injury, proposed surgical technique, potential complications (e.g., infection, loss of reduction, hardware failure, stiffness, nerve injury, persistent pain), expected outcomes, and the demanding post-operative rehabilitation protocol is critical. Obtaining informed consent is paramount.
Patient Positioning
The patient is typically positioned in the
beach chair position
.
* The entire ipsilateral arm and shoulder are prepped and draped freely to allow for intra-operative manipulation and assessment of reduction.
* The head is secured to allow for unimpeded surgical access to the superior shoulder.
* Care is taken to pad all pressure points to prevent nerve injury (e.g., ulnar nerve at the elbow, peroneal nerve at the fibular head).
* A sterile tourniquet is generally not used for AC joint surgery.
* Image intensification (fluoroscopy) is often used intraoperatively, particularly for accurate drilling and hardware placement for CC fixation. The C-arm should be draped and positioned to allow for AP and lateral views of the shoulder.
Detailed Surgical Approach / Technique
Surgical goals for AC joint injuries include anatomical reduction of the clavicle to the acromion and coracoid, stable fixation, and restoration of the AC and CC ligament complexes, often incorporating biological augmentation. Various techniques exist, broadly categorized as direct AC joint fixation, CC ligament reconstruction, or combined approaches.
General Principles
- Incision: A transverse incision (Langer's lines) approximately 5-7 cm long is made centered over the AC joint, or a saber-cut incision can be used for more extensive exposure.
-
Dissection:
- Subcutaneous dissection proceeds carefully to protect the supraclavicular nerves, which course superficially. Identifying and retracting these nerves can prevent post-operative dysesthesias.
- The deltotrapezial fascia is incised longitudinally along the fibers, exposing the underlying AC joint and distal clavicle. In Type V injuries, this fascia is often severely disrupted, and reapproximation is a critical step in reconstruction.
- The AC joint capsule and ligaments are assessed. The distal clavicle is then cleared to visualize the superior surface of the coracoid process.
- Reduction: The clavicle is anatomically reduced to the acromion and coracoid. This often requires traction on the arm, direct downward pressure on the clavicle, and upward pressure on the elbow/humerus. The reduction is confirmed visually and often fluoroscopically.
Common Surgical Techniques
1. Coracoclavicular (CC) Ligament Reconstruction with Suture Button System (e.g., AC TightRope™)
This technique aims to restore vertical stability by recreating the CC ligaments. It is increasingly popular due to its minimally invasive nature and good outcomes.
Steps:
1.
Exposure:
As described above, identify the distal clavicle and the base of the coracoid.
2.
Tunnel Preparation:
* A guidewire is advanced from the superior aspect of the clavicle (approximately 2.5-3 cm medial to the AC joint, ensuring adequate bone stock for button purchase) through the clavicle and centered over the coracoid base.
* Fluoroscopic guidance is essential to confirm correct positioning over the coracoid.
* A drill bit (e.g., 3.5-4.0 mm) is used to create a single clavicular tunnel and a single coracoid tunnel through the guidewire.
* Some systems utilize two tunnels for a double-button construct (e.g., one for conoid, one for trapezoid insertion sites).
3.
Suture Button Passage:
* The suture button device, pre-loaded with high-strength sutures, is passed through the clavicular and coracoid tunnels. The coracoid button is deployed beneath the coracoid.
* The sutures are then tensioned and tied over the superior clavicular button, reducing the clavicle to the coracoid. This should achieve a firm, stable reduction.
4.
Concomitant AC Joint Fixation/Repair (Optional but Recommended):
* While the suture button addresses vertical stability, horizontal stability (anterior-posterior) still relies on the AC joint capsule and ligaments.
* Consider repairing the disrupted AC joint capsule and superior AC ligament directly.
* Some surgeons advocate for an additional suture cerclage or trans-AC fixation (e.g., K-wires temporarily) to further stabilize the AC joint, especially in cases of significant horizontal instability.
2. Hook Plate Fixation
This method provides rigid fixation for both vertical and horizontal stability, but it's a temporary implant.
Steps:
1.
Exposure and Reduction:
As described, reduce the clavicle.
2.
Plate Placement:
A specialized hook plate is contoured. The hook engages the posterior-inferior aspect of the acromion, providing a buttress against superior migration. The plate shaft lies superiorly on the clavicle.
3.
Fixation:
The plate is secured to the clavicle with cortical screws. Care is taken to ensure the hook is properly seated and does not impinge on the rotator cuff or cause stress fractures of the acromion.
4.
Deltotrapezial Fascia Repair:
The fascia is repaired meticulously over the plate to aid in soft tissue healing and provide additional stability.
5.
Hardware Removal:
Hook plates are typically removed at 3-6 months post-operatively to prevent complications such as subacromial impingement, acromial osteolysis, or plate breakage.
3. Coracoclavicular Ligament Reconstruction with Graft (Autograft/Allograft)
This biological reconstruction aims to recreate the native CC ligaments. Tendon grafts (e.g., semitendinosus autograft, tibialis anterior allograft) are commonly used.
Steps:
1.
Exposure and Reduction:
As described.
2.
Tunnel Preparation:
* Two clavicular tunnels are drilled, mirroring the anatomical attachments of the conoid and trapezoid ligaments on the clavicle (one medial, one lateral).
* A single coracoid tunnel is drilled through the base of the coracoid, or two separate tunnels if recreating distinct conoid/trapezoid attachments.
3.
Graft Passage:
* The graft is looped around the coracoid process (or passed through a coracoid tunnel) and then woven through the clavicular tunnels.
* The graft is then tensioned with the clavicle reduced and secured using interference screws, cortical buttons, or suture anchors.
4.
Augmentation:
Often combined with an AC suture cerclage or other AC joint stabilization.
5.
Deltotrapezial Fascia Repair:
Essential for augmenting stability.
4. AC Joint Fixation with Suture Cerclage or K-wires (Less common as primary fixation)
Historically, K-wires were used to stabilize the AC joint directly. However, their high complication rates (migration, infection, breakage) have led to their limited use, primarily as temporary adjuncts or in combination with stronger CC fixation. Suture cerclage over the AC joint provides some horizontal stability.
Concomitant Procedures
- Distal Clavicle Excision (DCE): Rarely performed acutely. May be considered in chronic settings with significant AC joint arthritis or persistent pain/impingement after initial stabilization.
- Rotator Cuff or Labral Repair: If concomitant injuries are identified pre-operatively or intra-operatively.
Wound Closure
Layered closure of the deltotrapezial fascia, subcutaneous tissue, and skin is performed. Meticulous repair of the deltotrapezial fascia is crucial for long-term stability and strength.
Complications & Management
Despite advancements in surgical techniques, complications following AC joint reconstruction can occur. Awareness and proactive management are critical.
Common Complications and Salvage Strategies
| Complication | Incidence | Management / Salvage Strategy |
|---|---|---|
| Loss of Reduction/Fixation Failure | 5-15% (varies by technique) | Prevention: Meticulous technique, appropriate implant selection, strict post-operative immobilization. Management: Non-symptomatic: Observation. Symptomatic/Significant displacement: Revision surgery (re-reduction and re-fixation, often with a different or augmented technique, e.g., stronger graft, hook plate revision, or additional CC fixation). |
| Infection | <2% | Prevention: Strict sterile technique, prophylactic antibiotics. Management: Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics, possible hardware removal if persistent. |
| Hardware-Related Issues | Varies (e.g., Hook Plate removal ~100%; Suture Button ~5-10% symptomatic) | Hook Plate: Impingement, subacromial pain, acromial osteolysis, plate breakage. Management: Symptomatic plate removal (typically 3-6 months post-op). Suture Button: Suture breakage, osteolysis around tunnels, knot irritation. Management: Symptomatic hardware removal or revision. |
| Neurovascular Injury | Rare (<1%) | Prevention: Careful dissection, identification and protection of supraclavicular nerves, careful drilling to avoid subclavian vessels/brachial plexus. Management: Nerve laceration: Microsurgical repair. Paresthesia/neuropraxia: Observation, nerve gliding exercises. Vascular injury: Urgent vascular surgery consultation. |
| Stiffness/Adhesive Capsulitis | 5-10% | Prevention: Early, controlled range of motion as per rehab protocol, patient education. Management: Aggressive physical therapy, anti-inflammatories, manipulation under anesthesia, arthroscopic capsular release if recalcitrant. |
| Chronic Pain/Arthritis | 5-20% | Prevention: Anatomical reduction, restoration of joint congruity, appropriate stabilization. Management: Conservative measures (NSAIDs, injections, PT). Persistent symptoms: Distal clavicle excision (Mumford procedure), typically delayed until 6-12 months post-initial surgery. |
| Acromial Stress Fracture/Osteolysis | <5% (higher with hook plate) | Prevention: Proper hook plate sizing and positioning, avoiding aggressive contouring, early hardware removal. Management: Non-displaced: Immobilization. Displaced: Open reduction and internal fixation. |
| Heterotopic Ossification | Rare | Prevention: May consider NSAIDs or radiation in high-risk patients. Management: Observation, surgical excision if symptomatic and mature. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical component of successful AC joint injury management, aiming to protect the repair while gradually restoring range of motion, strength, and function. Protocols vary slightly depending on the surgical technique, surgeon preference, and patient's baseline function.
General Phases
Phase 1: Immobilization & Protection (0-4 weeks)
- Goals: Protect the surgical repair, minimize pain and swelling, prevent stiffness of uninvolved joints.
- Immobilization: Arm in a sling (often a shoulder immobilizer) for 2-4 weeks, depending on surgical stability and technique. For suture button repairs, a shorter immobilization period may be acceptable. For hook plates, strict immobilization for the entire duration of plate presence (until removal) is common, though some allow passive motion.
-
Activity:
- No active shoulder range of motion.
- Elbow, wrist, and hand active range of motion (AROM) exercises within the sling.
- Passive range of motion (PROM) for glenohumeral joint (pendulums, supine external rotation to 30 degrees, flexion to 90 degrees) may be initiated around 2-3 weeks, strictly avoiding AC joint stress.
- Scapular stabilization exercises (isometrics without shoulder movement).
- Cryotherapy and pain management.
- Restrictions: No lifting, pushing, pulling, or sudden movements. No abduction or external rotation beyond neutral for the AC joint.
Phase 2: Early Motion & Gentle Strengthening (4-8 weeks)
- Goals: Gradually restore active shoulder range of motion, initiate gentle strengthening, improve neuromuscular control.
-
Activity:
- Continue sling for comfort and protection (e.g., in public, sleeping), but progressively wean during the day for exercises.
- Progressive AROM and PROM of the shoulder: flexion, abduction, external rotation (as tolerated, usually to 90 degrees initially).
- Initiate gentle isometric exercises for the rotator cuff and deltoid, avoiding direct AC joint loading.
- Scapular stabilization exercises (e.g., retraction, depression).
- Start light resistance bands for internal/external rotation with the arm at the side.
- Restrictions: No heavy lifting. Avoid overhead activities. No direct AC joint loading (e.g., push-ups, dips).
Phase 3: Moderate Strengthening & Functional Return (8-16 weeks)
- Goals: Restore full pain-free range of motion, improve strength and endurance, prepare for return to light activities.
-
Activity:
- Full AROM should be achieved.
- Progressive strengthening exercises for the entire shoulder girdle (deltoid, rotator cuff, scapular stabilizers) with increasing resistance.
- Begin closed-chain exercises (e.g., wall push-ups, progress to kneeling push-ups) carefully.
- Introduce proprioceptive exercises (e.g., rhythmic stabilization).
- Hook Plate Removal (if applicable): Typically occurs at 3-6 months. Rehabilitation will often have a temporary setback immediately post-removal, followed by accelerated progression.
- Restrictions: Continue to avoid heavy lifting and direct contact sports. Gradual return to activities of daily living.
Phase 4: Advanced Strengthening & Return to Sport/Work (16+ weeks)
- Goals: Maximize strength, power, and endurance; achieve full functional recovery; prepare for return to sport or demanding occupations.
-
Activity:
- Sport-specific or work-specific training.
- Plyometric exercises, overhead activities, throwing progression.
- Progressive increase in weight and intensity for strengthening exercises.
- Focus on dynamic stability and power.
- Return to Play/Work: Typically allowed at 4-6 months for non-contact activities, and 6+ months for contact sports, pending full restoration of strength, stability, and pain-free range of motion, with specific criteria for functional testing. Return to full overhead labor may take 6-9 months.
Summary of Key Literature / Guidelines
The management of AC joint injuries, particularly Type III, remains a topic of ongoing debate and evolving evidence within orthopedic literature.
Rockwood Type III Injuries: Operative vs. Non-Operative
Historically, Type III injuries were often surgically managed. However, multiple prospective randomized controlled trials (e.g., the Cochrane review by Smith et al.) and systematic reviews have demonstrated that for many patients, non-operative management of acute Type III injuries yields comparable long-term functional outcomes to operative treatment, although with a higher rate of residual cosmetic deformity and potentially slight strength deficits. Studies often cite similar rates of osteoarthritis in both groups. The decision for operative intervention in Type III injuries is increasingly individualized, favoring operative treatment for high-demand athletes, heavy laborers, or those with significant cosmetic concerns. Chronic symptomatic Type III injuries often benefit from surgical reconstruction.
Surgical Techniques: Evolving Evidence
- Hook Plates: While providing rigid initial fixation and good early results, the mandatory second surgery for hardware removal (typically 3-6 months) and potential for complications such as subacromial impingement, acromial osteolysis, and plate breakage have led to a decline in their primary use, especially for non-Type III injuries. They remain a viable option for acute unstable injuries requiring robust fixation.
- Coracoclavicular Ligament Reconstruction (Suture Button Systems): Techniques like the AC TightRope™ have gained popularity due to their biological approach, dynamic stability, and potential for earlier rehabilitation. Comparative studies (e.g., Martetschläger et al., Mazzocca et al.) often report good to excellent clinical outcomes with these systems, showing improved stability and reduced hardware-related complications compared to older methods. Concerns include potential for osteolysis around the tunnels, loss of reduction, and knot irritation.
- Biological Reconstruction (Grafting): Using autograft or allograft to reconstruct the CC ligaments provides a more biological solution. Studies support its efficacy in restoring stability, particularly for chronic instabilities. However, graft harvest morbidity (for autografts), graft incorporation time, and potential for graft failure are considerations. Many modern techniques combine suture button fixation with additional autograft or allograft augmentation to enhance stability and promote biological healing, often referred to as a "hybrid" approach.
- Combined AC and CC Stabilization: There is a growing consensus that addressing both vertical (CC ligaments) and horizontal (AC ligaments/capsule) instability is crucial for optimal long-term outcomes, especially in severe injuries. Techniques combining CC reconstruction with direct AC joint repair or augmentation (e.g., suture cerclage or direct capsular repair) are favored by many surgeons to achieve more comprehensive stability.
Timing of Surgery
Acute repairs (within 2-3 weeks of injury) are generally preferred for Type IV, V, and VI injuries, as well as for selected Type III injuries, as they allow for primary ligament repair and anatomical reduction before significant scarring or retraction occurs. Chronic instability (typically >3-6 weeks post-injury) often necessitates reconstructive procedures, as primary ligament repair is no longer feasible due to tissue degradation.
Rehabilitation Principles
Most literature emphasizes a phased, progressive rehabilitation approach. Early passive motion is often allowed, with protection of the repair site. Gradual return to active motion and strengthening, followed by sport-specific training, is crucial. The duration of immobilization and weight-bearing restrictions varies, but a typical timeline for return to contact sports is 4-6 months or longer, contingent on individual healing and functional recovery.
In summary, the management of AC joint injuries is guided by the Rockwood classification, patient-specific factors, and the evolving evidence base. While non-operative treatment remains viable for many Type I, II, and select Type III injuries, surgical intervention for higher-grade injuries and symptomatic chronic instability aims to restore anatomical alignment and function through robust, biologically sound fixation and reconstruction techniques.
