PEDIATRIC ACROMIOCLAVICULAR DISLOCATIONS
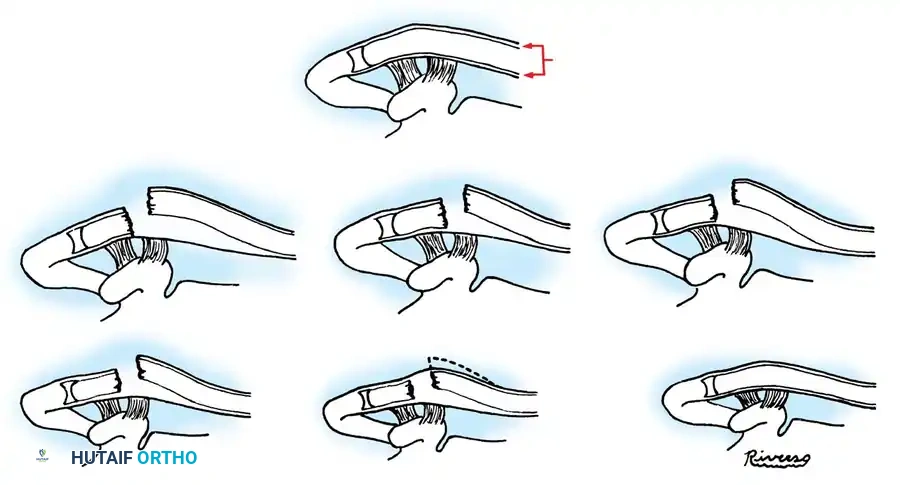
Acromioclavicular (AC) joint injuries in the pediatric and adolescent populations present a unique pathoanatomical challenge. Unlike adults, whose failure mechanism typically involves mid-substance ligamentous rupture, the pediatric injury is dictated by the immense structural integrity of the periosteal sleeve. The coracoclavicular (CC) and acromioclavicular ligaments are contiguous with this thick periosteal tube. Consequently, high-energy trauma often results in the clavicle rupturing through the superior aspect of the periosteum, leaving the ligaments anatomically intact but functionally detached from the displaced osseous clavicle. This phenomenon is classically termed a "pseudodislocation."
Classification of Pediatric AC Injuries
Dameron, Reibel, and Rockwood established a highly prognostic, five-tier classification system for pediatric acromioclavicular injuries based on the degree of periosteal disruption and the direction of clavicular displacement.
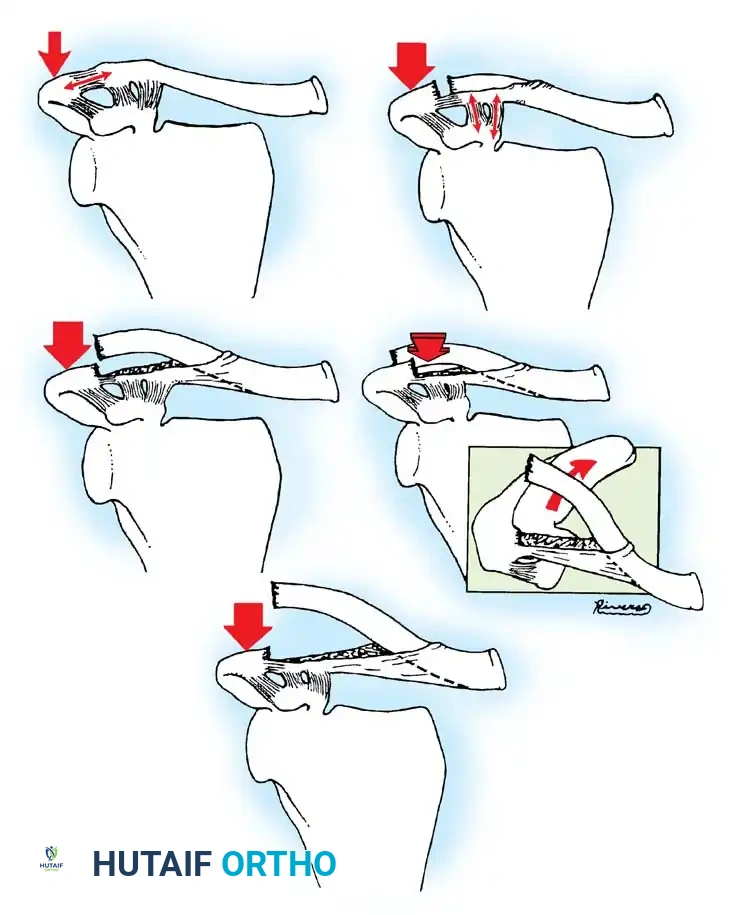
- Type I: A mild contusion or sprain of the AC joint. The force is insufficient to rupture either the acromioclavicular or the coracoclavicular ligaments. The periosteal sleeve remains entirely intact.
- Type II: The acromioclavicular ligaments are stretched or partially torn. The coracoclavicular ligaments remain intact. A partial periosteal sleeve (tube) tear occurs, leading to mild clinical instability but no gross radiographic displacement.
- Type III (The Classic Pseudodislocation): The acromioclavicular ligament is completely ruptured. The coracoclavicular ligaments remain entirely intact because they are firmly attached to the inferior periosteum. However, the clavicle itself is highly unstable; it displaces superiorly through a longitudinal rent in the superior periosteal tube.
- Type IV: Identical to the Type III pseudodislocation in terms of periosteal tearing, but the distal clavicle is displaced posteriorly into or through the trapezius muscle fascia, rather than purely superiorly.
- Type V: A severe, high-energy disruption. The acromioclavicular ligaments are completely disrupted. The coracoclavicular ligaments remain attached to the empty periosteal sleeve, but the lateral end of the clavicle is grossly unstable. It is driven superiorly and laterally, often burying itself deep within the trapezius and deltoid muscle bellies, or piercing the fascia to lie subcutaneously in the posterior aspect of the shoulder.
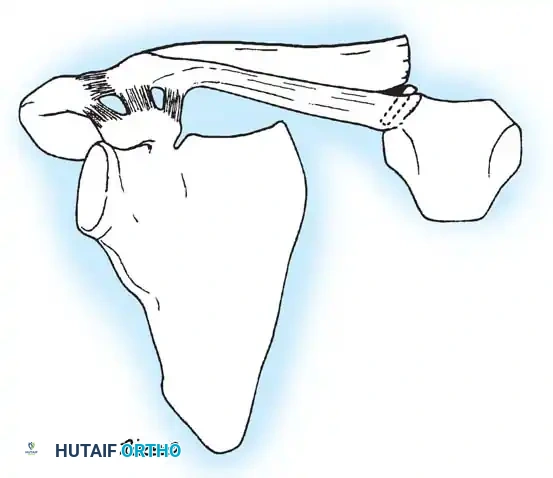
CLINICAL PEARL: In many Type III, IV, and V dislocations, an unrecognized fracture of the extreme distal end of the clavicle occurs concurrently. The AC and CC ligaments remain attached to this small distal osseous fragment and the empty periosteal tube. Always scrutinize high-quality orthogonal radiographs (including a Zanca view) to rule out transphyseal or distal metaphyseal fractures.
Indications for Management
The management of pediatric AC joint injuries is heavily influenced by the patient's age and the classification type. According to Curtis, Dameron, Reibel, and Rockwood, children and adolescents under the age of 15 with Type I, II, and III separations can be managed non-operatively. The robust osteogenic potential of the periosteal tube ensures that new bone will form along the path of the displaced clavicle, eventually remodeling into a Y-shaped lateral clavicle that is functionally excellent, albeit sometimes cosmetically prominent.
In patients older than 15 years, Type III injuries exist in a transitional zone and may require more aggressive, operative treatment depending on the patient's athletic demands.
Conversely, Type IV and V injuries are absolute indications for surgical intervention. The distal clavicle is incarcerated within the trapezius and deltoid musculature. If closed reduction maneuvers fail to disengage the clavicle from the muscle bellies, open reduction is mandatory to prevent severe dyskinesia, chronic pain, and unsightly deformity.
Surgical Technique: Open Reduction of Type IV and V AC Dislocations
When operative intervention is indicated for severe pediatric AC dislocations, the primary goal is the extrication of the clavicle from the surrounding musculature and its anatomical reduction back into the periosteal sleeve.
- Positioning and Setup: The patient is placed in the beach-chair position with the operative arm draped free to allow for manipulation. A bump is placed between the scapulae to allow the shoulder girdle to fall posteriorly, aiding in reduction.
- Surgical Approach: A saber-cut or transverse incision is made over the distal clavicle, extending laterally toward the acromion. Dissection is carried down through the subcutaneous tissue.
- Identification of Pathology: The deltotrapezial fascia is often found to be violently rent. The distal end of the clavicle will be visualized protruding through the trapezius (Type IV) or superiorly into the subcutaneous fat (Type V). The empty periosteal tube is identified inferiorly, with the CC ligaments still attached to it.
- Reduction: The clavicle must be meticulously disengaged from the muscle fibers. Traction on the arm combined with direct downward pressure on the clavicle usually facilitates reduction. The clavicle is then guided back into the empty periosteal tube.
- Repair and Imbrication: The periosteal tube must be meticulously repaired over the reduced clavicle using heavy absorbable sutures. Following this, the deltoid and trapezius muscle fascia must be imbricated superiorly over the clavicle to provide a robust dynamic stabilizer.
- Internal Fixation: If the periosteal repair is tenuous or the reduction remains unstable, internal fixation is required. This can be achieved via temporary acromioclavicular smooth Kirschner wires (which must be bent to prevent migration) or coracoclavicular fixation (e.g., suture buttons or heavy non-absorbable cerclage), similar to adult techniques.
SURGICAL WARNING: Falstie-Jensen and Mikkelsen note that the true extent of periosteal damage can only be determined intraoperatively. In some high-energy Type IV and V lesions, a total rupture of the coracoclavicular ligaments may actually be present, necessitating primary ligamentous repair or augmentation alongside periosteal closure.
FRACTURES AND DISLOCATIONS OF THE CLAVICLE
Pediatric clavicle fractures are ubiquitous, yet their management differs fundamentally from adult protocols. They are anatomically classified into fractures of the outer (distal), middle, and proximal (medial) thirds.
Distal (Outer) Third Clavicle Fractures
Fractures of the distal third of the clavicle in children heal exceptionally well without surgical intervention. This is directly attributable to the periosteal tube remaining intact at the fracture site, which acts as an internal splint and a scaffold for rapid osteogenesis.
The ligamentous attachments (coracoclavicular and coracoacromial) remain securely fastened to the inferior periosteal sleeve. Even in the presence of significant superior displacement of the proximal fracture fragment, remodeling occurs rapidly along the intact periosteal tube.
While some authors advocate for surgical reduction of displaced distal clavicle fractures in adults due to the high risk of nonunion, this paradigm does not apply to children. Havranek's pivotal study of distal physeal clavicular injuries demonstrated that conservative management (closed reduction, figure-of-eight bandage, or Desault bandage) yields excellent functional outcomes. Surgery is reserved strictly for older adolescents nearing skeletal maturity or for extreme cases where the displacement of the central metaphyseal fragment causes severe shortening of the shoulder girdle and unacceptable cosmetic deformity.
Midshaft Clavicle Fractures
Fractures of the midshaft of the clavicle are the most common pediatric clavicle injuries. They rarely require surgical treatment. In fact, open reduction is generally avoided in children because periosteal stripping during surgery significantly increases the incidence of delayed union and nonunion.
If a severely displaced midshaft fracture is tenting the skin and threatening necrosis, it can often be reduced closed. Under general or local anesthesia, a sterile towel clip can be used to percutaneously grasp the fragment and manipulate it beneath the trapezius to relieve skin tension.
Indications for Surgery in Pediatric Midshaft Fractures:
1. Open Fractures: Requiring emergent irrigation and débridement.
2. Neurovascular Compromise: A vascular injury complicating the fracture is an absolute surgical emergency.
3. Severe Shortening: As noted by Kubiak et al., severe shortening of the shoulder girdle with displaced, comminuted intermediate fragments may warrant fixation to prevent long-term scapular dyskinesia.
4. Established Traumatic Nonunion: While exceedingly rare in children, true traumatic nonunion requires operative intervention.
PITFALL: Do not confuse an acute pediatric clavicle fracture or a traumatic nonunion with Congenital Pseudarthrosis of the Clavicle. Congenital pseudarthrosis almost exclusively occurs on the right side, presents painlessly in early childhood, and demonstrates smooth, "rounded" sclerotic bone ends on radiography without a history of acute trauma.
Surgical Management of Midshaft Nonunion
When a true traumatic nonunion is established, open reduction and internal fixation (ORIF) is required.

Fig. 33-98A: Radiographic presentation of a traumatic nonunion of the right clavicle in a 3-year-old child. Note the lack of bridging callus and the sharp, non-rounded bone ends, differentiating it from congenital pseudarthrosis.

Fig. 33-98B: Postoperative radiograph following open reduction and internal fixation. At surgery, fibrous tissue and rudimentary callus were excised. Rigid fixation was achieved using a semitubular plate, leading to successful osseous union.
Operative Steps for Midshaft Plating:
1. An infraclavicular incision is utilized to minimize scar widening and avoid direct pressure from backpack straps.
2. The supraclavicular nerves are identified and protected to prevent postoperative chest wall numbness.
3. The nonunion site is exposed. Minimal periosteal stripping is performed—only enough to apply the plate.
4. The fibrous nonunion is taken down, and the bone ends are decorticated until punctate bleeding (the "paprika sign") is observed.
5. Rigid fixation is applied superiorly or anteroinferiorly using a pre-contoured locking or semitubular plate, ensuring at least three bicortical screws on each side of the fracture.
6. Autologous bone grafting (often from the iliac crest) may be added if a significant defect exists after debridement.
Proximal (Medial) Clavicle Fractures and Sternoclavicular Injuries
Injuries to the medial third of the clavicle and the sternoclavicular (SC) joint are notoriously difficult to diagnose clinically and radiographically. Standard anteroposterior radiographs are often obscured by the overlapping ribs and mediastinal structures.
The medial physis of the clavicle is the last growth plate in the body to close, typically fusing between the ages of 20 and 24. Consequently, the vast majority of injuries diagnosed clinically as "anterior dislocations of the sternoclavicular joint" in children and young adults are, in reality, Salter-Harris Type I or II fractures of the proximal clavicular physis.
Diagnostic Imaging
To differentiate between a true SC dislocation and a physeal fracture, specialized imaging is required.
* The Serendipity View: A 45-degree cephalic tilt view, as recommended by Rockwood, is highly effective. In an anterior displacement, the injured medial clavicle will appear cephalad compared to the uninjured contralateral side. In a posterior displacement, it will appear caudad.
* Axial Computed Tomography (CT): CT is the gold standard and the most informative imaging modality for medial clavicle injuries. It definitively delineates physeal separations from true joint dislocations and assesses the proximity of the displaced bone to critical mediastinal structures.
Management of Anterior Displacements
Anterior physeal fractures and anterior SC dislocations should almost universally be treated conservatively. A visible "knot" or prominence usually appears 2 to 3 weeks post-injury as robust fracture callus forms.
While closed reduction is easily achieved by pulling the shoulders posteriorly, it is notoriously difficult to maintain. Fortunately, these fractures remodel exceptionally well, leaving only a minor, asymptomatic anterior prominence. Operative treatment for anterior displacements is strongly discouraged; Rockwood has extensively documented the severe, sometimes fatal, complications associated with ill-advised pin fixation of the medial clavicle, including pin migration into the heart or great vessels.
Management of Posterior (Retrosternal) Displacements
Posterior displacement of the medial clavicle—whether a true dislocation or a retrosternal physeal fracture—is a true orthopedic emergency.
Goldfarb et al. emphasized that retrosternal displacements carry a high risk of compressing adjacent mediastinal structures, including the trachea, esophagus, and the great vessels (subclavian artery/vein, brachiocephalic vein).
Treatment Protocol for Posterior Displacements:
1. Immediate CT Angiography: To evaluate the exact location of the bone fragment relative to the vascular structures.
2. Cardiothoracic Standby: Any reduction maneuver must be performed in the operating room under general anesthesia with a cardiothoracic or vascular surgeon immediately available, as dislodging the clavicle can unroof a tamponaded vascular tear.
3. Closed Reduction: A sandbag is placed between the scapulae. Lateral traction is applied to the abducted arm while a sterile towel clip is used to percutaneously grasp the medial clavicle and lift it anteriorly.
4. Open Reduction: Waters et al. noted that if closed reduction fails, open reduction is mandatory. The periosteum is incised, the clavicle is levered out of the mediastinum, and it is secured. If it is a physeal fracture, heavy non-absorbable transosseous sutures (e.g., figure-of-eight configuration) are used to secure the metaphysis to the medial epiphysis/sternum. Hardware (plates or K-wires) should be strictly avoided at the sternoclavicular joint due to the catastrophic risks of migration.
Postoperative Protocols and Rehabilitation
Following surgical intervention for either AC dislocations or clavicle fractures, the pediatric patient is immobilized in a sling or shoulder immobilizer for 4 to 6 weeks to allow for soft tissue healing and initial osseous consolidation.
