Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 38-year-old man reports a 2-week history of acute lower back pain with radiation into the left lower extremity. There is no history of trauma and no systemic signs are noted. Examination reveals a positive straight leg test at 35 degrees on the left side and a contralateral straight leg raise on the right side. Motor testing demonstrates mild weakness of the gluteus medius and weakness of the extensor hallucis longus of 3+/5. Sensory examination demonstrates decreased sensation along the lateral aspect of the calf and top of the foot. Knee and ankle reflexes are intact and symmetrical. Radiographs demonstrate no obvious abnormality. MRI scans show a posterolateral disk hernation. The diagnosis at this time is consistent with a herniated nucleus pulposus at

Explanation
The patient's history and physical examination findings are consistent with a lumbar disk herniation at the L4-5 level. Weakness of the extensor hallucis longus and gluteus medius are consistent with an L5 lumbar radiculopathy. Nerve root tension signs are also consistent with sciatica from a lumbar disk herniation. The MRI scans confirm a posterolateral disk herniation at L4-5, which typically affects the exiting L5 nerve root. Hoppenfeld S: Orthopedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 45-74.
Question 2
A 10-year-old girl has a midshaft both bone forearm fracture. After attempted closed reduction, alignment consists of bayonet apposition, 10 degrees of malrotation, and 8 degrees of volar angulation. Management should now consist of

Explanation
Acceptable alignment in both bone forearm fractures is related to age and location. In children younger than age 9 years, angulations of 15 degrees and malrotation of 45 degrees are acceptable. In children older than age 9 years, acceptable alignment is 10 degrees of angulation and 30 degrees of malrotation. Bayonet apposition is acceptable provided that the angular and rotational reductions are held within these guidelines. A long arm cast provides better control of deforming forces than a short arm cast. Do TT, Strub WM, Foad SL, et al: Reduction versus remodeling in pediatric distal forearm fractures: A preliminary cost analysis. J Pediatr Orthop B 2003;12:109-115. Flynn JM: Pediatric forearm fractures: Decision making, surgical techniques, and complications. Instr Course Lect 2002;51:355-360. Ring D, Waters PM, Hotchkiss RN, et al: Pediatric floating elbow. J Pediatr Orthop 2001;21:456-459.
Question 3
A 23-year-old man has had right posterolateral knee pain and occasional lateral calf dysesthesias for the past 8 months. A radiograph, CT scan, MRI scans, and a biopsy specimen are shown in Figures 62a through 62e. What is the most likely diagnosis?





Explanation
The radiograph shows an eccentric, cortically based lytic lesion in the proximal fibula. The CT and MRI scans confirm that it is well circumscribed and cortically based with significant surrounding edema. The radiographic differential diagnosis would be a Brodie's abscess or osteoid osteoma. An osteoblastoma would have to be greater than 2 cm in size. A chondroblastoma may also have significant edema around it, but it is an epiphyseal-based lesion, not cortically based. The well-circumscribed nature of the lesion is not consistent with osteosarcoma. The pathology shows a very cellular and vascular stroma with plump, but not atypical osteoblast cells making a matrix of immature woven bone. There are no abundant inflammatory cells or dead bone suggestive of osteomyelitis or a Brodie's abscess. Therefore, the clinical and histologic picture is most consistent with an osteoid osteoma. Percutaneous radiofrequency ablation, usually with CT guidance, has become the preferred method for treating most cases of osteoid osteoma. Rosenthal DI: Radiofrequency treatment. Orthop Clin North Am 2006;37:475-484.
Question 4
In a retroperitoneal approach to the lumbar spine, what nerve is commonly found on the psoas muscle?
Explanation
The genitofemoral nerve and the sympathetic plexus consistently lie on the ventral surface of the psoas muscle. The ilioinguinal and iliohypogastric nerves are the most superior branches of the lumbar plexus and emerge along the upper lateral border of the psoas muscle traveling toward the quadratus lumborum. Both the obturator and femoral nerves are deep and lateral to the psoas muscle. Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107. Johnson R, Murphy M, Southwick W: Surgical approaches to the spine, in Herkowitz HH (ed): The Spine, ed 4. Philadelphia, PA, WB Saunders, 1992, p 1559.
Question 5
A 16-year-old boy with osteochondritis dissecans of the capitellum has intermittent symptoms of catching and locking. Examination is unremarkable. Radiographs reveal a loose body anteriorly with a diameter of 10 mm. To remove the loose body, elbow arthroscopy is being considered. Which of the following procedures would minimize the risk of neurovascular complication during the procedure?
Explanation
Complications of elbow arthroscopy are usually minor or temporary. However, serious complications include nerve injuries. The deep radial nerve is the closest to any of the portals, resting as close as 1 mm away from the scope inserted in the anterolateral portal. The capsule can be displaced anteriorly by distending the joint with about 25 mL of saline solution, thus moving the deep radial nerve approximately 1 cm anteriorly and decreasing the risk of injuring it while establishing the anterolateral portal. Keeping plastic cannulae in the portals may help to diminish fluid extravasation and swelling, which is more of an impediment than a serious complication. The image intensifier has no documented role in guiding loose body removal. While the proximal anteromedial portal is probably the safest anterior portal to establish, it is actually easier to remove a large loose body from this portal while viewing it from an anterolateral position. There is less tendon and muscle bulk to pass through at the site of the proximal anteromedial portal than at the anterolateral portal, making it less likely for the loose body to get stuck in the soft tissues. Techniques have been developed to permit removal of loose bodies as large as 2 cm in diameter without breaking them up into pieces. If it is possible to remove a large loose body intact, doing so greatly simplifies and shortens the procedure. Lynch GJ, Meyers JF, Whipple TL, Caspari RB: Neurovascular anatomy and elbow arthroscopy: Inherent risks. Arthroscopy 1986;2:190-197.
Question 6
In the anterior approach (Smith-Petersen) to the hip, dissection is carried out between muscles innervated by the

Explanation
In the Smith-Petersen approach to the hip, dissection is carried out between the tensor fascia lata laterally (supplied by the superior gluteal nerve) and the sartorius and rectus femoris medially (both supplied by the femoral nerve). Crenshaw AH Jr: Surgical techniques and approaches, in Canale ST (ed): Campbell's Operative Orthopaedics, ed 9. St Louis, MO, Mosby-Year Book, 1998, vol 1, pp 82-85.
Question 7
What muscle attaches to the site shown by the arrow in Figure 2?

Explanation
The latissimus dorsi inserts on the humerus metaphysis between the pectoralis major (posterior) and teres major (anterior). Teres minor inserts on the base of the greater tuberosity. Pectoralis minor does not insert on the humerus. Williams PL, Warwick R, Dyson M, Bannister LH: Neurology, in Gray's Anatomy, ed 37. Edinburgh, Scotland, Churchill Livingstone, 1989, pp 1131-1132.
Question 8
What is the 5-year overall survival rate for adults with high-grade soft-tissue sarcomas?
Explanation
The 5-year overall survival rate for deep, high-grade soft-tissue sarcomas is around 50%. The overall survival and disease-free survival rates chiefly depend on the tumor stage, but for all stages combined, most cancer treatment centers report a 5-year overall survival rate of around 70% and a disease-free survival rate of 65%. Fleming ID, et al: Manual for Staging of Cancer/American Joint Committee on Cancer, ed 5. Philadelphia, PA, Lippincott Raven, 1997, pp 149-156.
Question 9
A 15-year-old athlete collapses suddenly during practice and dies. What is the most likely cause of death?

Explanation
The number one cause of sudden death in the young athlete is myocardial pathology, with hypertrophic cardiomyopathy being most common. Because of cardiac muscle hypertrophy, the ventricular capacity is diminished and can result in decreased cardiac output. During exertional activities, the increased demand may not be able to be met and leads to sudden death. While the other choices can be the cause of sudden death in an otherwise healthy young athlete, their incidence is even more rare. Van Camp SP, Bloor CM, Mueller FO, et al: Nontraumatic sports death in high school and college athletes. Med Sci Sports Exerc 1995;27:641-647. Maron BJ, Shirani J, Pollac LC, et al: Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. JAMA 1996;276:199-204.
Question 10
High Yield
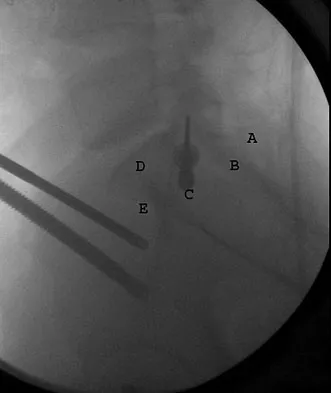
What letter in Figure 33 marks the correct starting point for a transiliac pelvic screw?
Explanation
Iliosacral screws cannot always be placed safely due to variations in pelvic anatomy. Transiliac bars are an alternative method for fixation but are placed using an open technique. A screw can be placed percutaneously through both iliac wings posterior to the posterior border of the sacrum. The starting point is visualized using a lateral C arm shot and is located on the posterior iliac crest at about the level of the S1 body where the crest has its largest area posterior to the sacrum. This area is labeled A in the figure, B represents the sacral canal, C is S1, D is the area cephalad to the iliocortical density, and E is the anterior border of the sacrum. The radiograph demonstrates a well-placed sacroiliac screw. Moed BR, Fissel BA, Jasey G: Percutaneous transiliac pelvic fracture fixation: Cadaver feasibility study and preliminary clinical results. J Trauma 2007;62:357-364.
Question 11
An 11-year-old boy has had a fever and pain and swelling over the lateral aspect of his right ankle for the past 3 days. Examination reveals warmth, swelling, and tenderness over the lateral malleolus, and he has a temperature of 103.2 degrees F (39.5 degrees C). Laboratory studies show a WBC count of 13,200/mm3 with 61% neutrophils, an erythocyte sedimentation rate of 112 mm/h, and a C-reactive protein of 15.7. Radiographs and a T2-weighted MRI scan are shown in Figures 13a through 13c. Aspiration yields 1 mL of purulent fluid. Management should now consist of



Explanation
The initial signs and symptoms of acute hematogenous osteomyelitis vary widely but usually include fever, bone pain, and impaired use of the involved extremity. In lower extremity infections, the child may limp or refuse to walk. Examination often reveals bone tenderness. In more advanced cases, erythema, warmth, and swelling may be present. The WBC and neutrophil counts are not always elevated, but the erythocyte sedimentation rate will be abnormal in more than 90% of patients. When the infection is diagnosed early, before a subperiosteal abscess has formed, antibiotics alone may be adequate to treat the infection. This patient has a more advanced infection, however, with the MRI scan revealing a subperiosteal abscess that was confirmed by aspiration. When an abscess is present, surgical drainage is generally indicated to remove devitalized tissue and to enhance the efficacy of the antibiotics. Further studies, such as bone or indium scans, are not necessary and will delay definitive treatment. Scott RJ, Christofersen MR, Robertson WW Jr, et al: Acute osteomyelitis in children: A review of 116 cases. J Pediatr Orthop 1990;10:649-652.
Question 12
An 18-year-old man recently underwent an uncomplicated arthroscopic partial medial meniscectomy that was complicated by reflex sympathetic dystrophy (RSD), also termed "sympathetically maintained pain" (SMP). What is the most common finding of this condition?

Explanation
The hallmark for RSD or SMP is the presence of pain that is out of proportion to that expected for the degree of the injury. SMP often extends well beyond the involved area and is present in a nonanatomic distribution. The pain is frequently described as a burning sensation, with extreme sensitivity to light touch. Joint stiffness can be present but is a nonspecific finding. There may be cold intolerance, but this is not a cardinal symptom. Sweating actually may be increased. Osteopenia, if present, is a late finding. Lindenfeld TN, Bach BR Jr, Wojtys EM: Reflex sympathetic dystrophy and pain dysfunction in the lower extremity. Instr Course Lect 1997;46:261-268.
Question 13
An extended head hemiarthroplasty (rotator cuff tear arthropathy head) has what theoretic advantage when compared to a standard hemiarthroplasty?
Explanation
The theoretic advantage of a metal-to-bone articulation with the acromion is that there is a greater arc in which a smooth metal surface contacts the glenoid and acromion. This may improve pain and function, but no studies have evaluated this to date. One study showed results comparable to that of a standard hemiarthroplasty. There are no other biomechanic advantages. Visotsky JL, Basamania C, Seebauer L, et al: Cuff tear arthropathy: Pathogenesis, classification, and algorithm for treatment. J Bone Joint Surg Am 2004;86:35-40.
Question 14
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of

Explanation
The prognosis for most patients with Osgood-Schlatter disease is good. When the secondary ossification center unites with the main body of the tibial tubercle, the patellar tendon has a more rigid anchor, and heterotopic ossification and its associated reaction often become quiescent. However, even after closure of the growth plates, some patients have persistent symptoms. Excision of the ossicle and prominence of the tibial tuberosity decompresses the patellar tendon and allows most patients to resume sports activities. Nonsurgical modalities are ineffective. Better results have been reported after excision than after drilling of the tubercle. Excision of the ossicle is not indicated prior to skeletal maturity because symptoms will resolve in most patients when the secondary ossification center unites. Flowers MJ, Bhadreshwar DR: Tibial tuberosity excision for symptomatic Osgood-Schlatter disease. J Pediatr Orthop 1995;15:292-297.
Question 15
A 29-year-old woman was injured in a high-speed motor vehicle accident 3 hours ago. Radiographs are shown in Figures 7a through 7e. Her right foot injury is open and contaminated. Her associated injuries include a closed head injury and a ruptured spleen requiring resection. She has had 6 units of packed red blood cells and the trauma surgeon has turned her care over to you. Her current base deficit is 10 and her urinary output has averaged 0.4 mL/kg for the last 2 hours. What is the best treatment at this time?





Explanation
The patient appears to be a borderline or unstable surgical patient following her initial trauma and spleenectomy (high base excess and low urine output). She needs continued resuscitation and minimal additional blood loss. This is best accomplished with irrigation and debridement of the ankle, external fixation of the ankle, foot, and femur, and splinting of the forearm. A traction pin for the femoral fracture will not control bleeding as well as an external fixator. Intramedullary nailing of the femur and open reduction and internal fixation of the forearm would be appropriate in patients that are euvolemic and stable. Pape HC, Hildebrand F, Pertschy S, et al: Changes in the management of femoral shaft fractures in polytrauma patients: From early total care to damage control orthopedic surgery. J Trauma 2002;53:452-461. Taeger G, Ruchholtz S, Waydhas C, et al: Damage control orthopedics in patients with multiple injuries is effective, time saving, and safe. J Trauma 2005;59:409-416. Harwood PJ, Giannoudis PV, van Griensven M, et al: Alterations in the systemic inflammatory response after early total care and damage control procedures for femoral shaft fracture in severely injured patients. J Trauma 2005;58:446-452.
Question 16
Which of the following findings is the best radiographic indicator of segmental instability at L4-L5?

Explanation
Motion segments that demonstrate more than 4 mm of translation or 10 degrees of angulation compared with adjacent motion segments on flexion-extension radiographs have excessive motion and instability. Anterior marginal osteophytes form at the insertion of the annulus from increased forces but do not indicate increased motion. A spondylolisthesis or lateral listhesis is often static without increased motion. More than 3.5 mm of translation or 11 degrees of angulation is considered instability criteria for the cervical spine. Internal disk disruption does not denote instability. Boden SD, Wiesel SW: Lumbosacral segmental motion in normal individuals. Have we been measuring instability properly? Spine 1990;15:571-576.
Question 17
The essential lesion responsible for posterolateral rotatory instability of the elbow is disruption of the
Explanation
Posterolateral rotatory instability (PLRI) of the elbow represents a three-dimensional injury pattern of rotational displacement of the ulna from the trochlea and the radius from the capitellum. The ulna supinates (externally rotates) past its normal limit and the radiocapitellar joint subluxates posterolaterally, permitting the coronoid process to slide beneath the trochlea. In cadaver studies, the lateral ulnar collateral ligament has been shown to be the essential lesion responsible for PLRI. The medial collateral ligament (of which the anterior bundle is the most important) is the primary restraint to valgus instability. The posterolateral capsule and radial collateral ligament may be disrupted in a complete posterolateral dislocation but are not essential injuries for PLRI. The primary function of the annular ligament is to stabilize the proximal radioulnar joint. O'Driscoll SW, Jupiter JB, King GJW, Hotchkiss RN, Morrey BF: The unstable elbow. J Bone Joint Surg Am 2000;82:724-738. Olsen BS, Sojbjerg JO, Dalstra M, Sneppen O: Kinematics of the lateral constraints of the elbow. J Shoulder Elbow Surg 1996;5:333-341.
Question 18
A 14-year-old boy has had knee pain for the past 2 months. He also has a low-grade fever of 101.3 degrees F (38.5 degrees C). Laboratory studies show a WBC count of 12,100/mm3 and an erythrocyte sedimentation rate of 58/h. A biopsy specimen of a lesion in the distal femoral metaphysis is shown in Figure 38. What is the most appropriate treatment?

Explanation
The clinical presentation of this patient is consistent with both acute osteomyelitis and Ewing's sarcoma. Both entities can be noted in the distal femoral metaphysis although Ewing's sarcoma is classically noted in the diaphysis. The histology reveals a mixed inflammatory cell infiltrate with neutrophils, plasma cells, lymphocytes, and histiocytes. Ewing's sarcoma would be a uniform population of small round blue cells without an inflammatory component. Eosinophilic granuloma (EG) is characterized by Langerhans histiocytes and eosinophils. Treatment of EG often consists of an intralesional steroid injection. Treatment of acute osteomyelitis includes surgical debridement and antibiotics. McCarthy JJ, Dormans JP, Kozin SH, et al: Musculoskeletal infections in children: Basic treatment principles and recent advancements. Instr Course Lect 2005;54:515-528.
Question 19
Following preoperative chemotherapy, the percent of tumor necrosis has been shown to be of prognostic value for which of the following tumors?

Explanation
The grading of response to chemotherapy for osteosarcoma was introduced by Huvos and associates. Patients with tumors that show more than 90% necrosis after neoadjuvant chemotherapy are considered to have had a good response and have better survival rates than those with less than 90% necrosis. However, it should be noted that survival rates for patients with a poor response are still better than in patients who do not receive neoadjuvant chemotherapy. More recently, similar results have been reported in patients with Ewing's sarcoma. Chemotherapy is not typically used for giant cell tumor of bone. Meyers PA, Heller G, Healey J, Huvos A, Lane J, Marcove R, et al: Chemotherapy for nonmetastatic osteogenic sarcoma: The Memorial Sloan- Kettering experience. J Clin Oncol 1992;10:5-15.
Question 20
A young man sustains a lumbar strain in an on-the-job motor vehicle accident. Both he and his treating physician feel that he is capable of limited duty with appropriate restrictions shortly after the injury. What term best describes his work status?
Explanation
Because the man is only recently removed from his injury and is judged capable of returning to work with some restrictions, the term that best describes his work status is temporary partial disability.
Question 21
Figures 11a and 11b show the T2-weighted MRI scans of the lumbar spine of a 53-year-old woman who has low back and right lower extremity pain. What structure is the arrow pointing to in Figure 11a?


Explanation
The arrow is pointing to a cystic-appearing structure with high signal intensity on T2-weighted image sequencing. It appears to be contiguous with the hypertrophied right facet joint, which appears to also have high signal intensity. The mass significantly narrows the right lateral recess. The high signal intensity suggests that this is a fluid-filled mass. In addition, the facet joints are degenerative and there is a very mild degree of anterolisthesis on the sagittal image. These findings make a lumbar synovial cyst the most likely diagnosis. Most lumbar juxtafacet cysts are observed at the L4-5 level, extradurally and adjacent to the degenerative facet joint. They may contain synovial fluid and/or extruded synovium. Presentation is indistinguishable from that of a herniated disk. The etiology of spinal cysts remains unclear, but there appears to be a strong association between their formation and worsening spinal instability. They occasionally regress spontaneously and may respond to aspiration and injection of corticosteroids, though there is a high recurrence rate with nonsurgical management. Synovial cysts resistant to nonsurgical management should be treated surgically. If the patient's symptoms can be attributable to radicular findings, a microsurgical decompression that limits further destabilization should suffice. However, if there is significant low back pain attributable to spinal instability, decompression and fusion remains an appropriate option. Banning CS, Thorell WE, Leibrock LG: Patient outcome after resection of lumbar juxtafacet cysts. Spine 2001;26:969-972. Deinsberger R, Kinn E, Ungersbock K: Microsurgical treatment of juxta facet cysts of the lumbar spine. J Spinal Disord Tech 2006;19:155-160.
Question 22
A 29-year-old woman who underwent an anterior cruciate ligament (ACL) reconstruction 6 months ago now reports difficulty achieving full knee extension, and physical therapy fails to provide relief. The knee is stable on ligament testing. Figure 3 shows the findings at a repeat arthroscopy. Treatment should now include

Explanation
The patient has a cyclops lesion. This is a nodule of fibroproliferative tissue that originates from either drilling debris from the tibial tunnel or remnants of the ACL stump; more rarely it is the result of broken graft fibers. The treatment of choice is excision of the nodule and, if needed, additional notchplasty. Marked improvements in function and symptoms have been noted after removal of the extension block and resumption of a rehabilitation program. Delince P, Krallis P, Descamps PY, et al: Different aspects of the cyclops lesion following anterior cruciate ligament reconstruction: A multifactorial etiopathogenesis. Arthroscopy 1998;14:869-876.
Question 23
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of

Explanation
The clinical photographs show a patient with a type I hereditary sensory motor neuropathy who has cavus feet with a flexible hindfoot. The Coleman block test shows that the hindfoot corrects into valgus. To prevent progressive cavus, patients with this condition may benefit from soft-tissue releases at a younger age while the foot is flexible. Once there is fixed deformity, combined soft-tissue and bone procedures usually are necessary. Metatarsal osteotomies will correct the cavus, but will do nothing for the drop foot. Transfer of the extensor hallucis longus to the neck of the first metatarsal and modified transfer of the extensor digitorum longus to the dorsum of the foot will prevent further claw toes and improve foot dorsiflexion. Anterior transfer of the posterior tibialis tendon will also aid in dorsiflexion. Calcaneal osteotomy should be reserved for fixed hindfoot varus that does not correct with block testing, and triple arthrodesis should be avoided as long as possible because the long-term outcome is poor. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, Ill, American Academy of Orthopaedic Surgeons, 1999, pp 235-245. Coleman SS: Complex Foot Deformities in Children. Philadelphia, Pa, Lea & Febiger, 1983, pp 147-165.
Question 24
A 10-year-old boy sustained an injury to the left knee. The radiographic findings shown in Figure 19 are most commonly associated with injury to which of the following structures?

Explanation
The radiograph shows a bony avulsion of the ACL attachment site on the tibial spine in this skeletally immature patient. In this age group, injury often results in failure of the bony attachment site rather than the substance of the ligament. Avulsion of the patellar tendon insertion site can occur, but this structure is located at the apophysis of the tibial tubercle. The attachment site of the PCL is much more posterior. In adults, bony avulsion is more commonly associated with PCL injuries than with ACL injuries. When a small bony avulsion of the lateral capsule from the lateral tibial plateau is seen on the AP view, this finding is considered pathognomonic of an ACL injury (Segond sign) in adults. The area of the pes anserinus is anterior and distal; avulsion would be unusual. Baxter MP, Wiley JJ: Fractures of the tibial spine in children: An evaluation of knee stability. J Bone Joint Surg Br 1988;70:228-230. Meyers MH, McKeever FM: Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1970;52:1677-1684.
Question 25
Figures 4a through 4c show the radiographs of a 43-year-old woman who sustained a twisting injury to her right ankle. She has ankle pain and tenderness medially and laterally. To help determine the optimal treatment, an external rotation stress radiograph of the ankle is obtained. This test is designed to evaluate the integrity of what structure?



Explanation
In the presence of a supination external rotation-type fracture of the distal fibula (Weber type B), stability of the ankle is best assessed by performing an external rotation stress AP view of the ankle. This test is used to assess the integrity of the deltoid ligament. The presence of a deltoid ligament rupture results in instability and generally is best managed surgically. The gravity stress test can also be used. Egol KA, Amirtharajah M, Tejwani NC, et al: Ankle stress test for predicting the need for surgical fixation of isolated fibular fractures. J Bone Joint Surg Am 2004;86:2393-2398. McConnell T, Creevy W, Tornetta P III: Stress examination of supination external rotation-type fibular fractures. J Bone Joint Surg Am 2004;86:2171-2178.
Question 26
In an effort to reduce costs, a limited MRI sequence is planned to detect a possible occult hip fracture. What is the anticipated fracture signal?
Explanation
At present, radiologists perform multiple MRI images to rule out all possible diagnoses. The ability to specify the anticipated changes on MRI should become more important as a means of reducing costs. MRI is sensitive to changes in free water (or hemorrhage) and thus this will appear dark on T1 and bright on T2. Miller MD: Review of Orthopaedics, ed 3. Philadelphia PA, WB Saunders, 2000, p 116.
Question 27
A 23-year-old baseball pitcher reports pain in the posterior aspect of his dominant shoulder during the late cocking phase of throwing. With the dominant shoulder positioned in 90 degrees of abduction from the body and with the scapula stabilized, examination reveals 135 degrees of external rotation and 20 degrees of internal rotation. Examination of the opposite shoulder reveals 100 degrees of external rotation and 75 degrees of internal rotation. Both shoulders are stable on examination. Radiographs and MRI scans are unremarkable. What is the primary cause of his pain?

Explanation
Internal impingement of the shoulder is a leading cause of shoulder pain in the throwing athlete. The primary lesion in pathologic internal impingement is excessive tightening of the posterior band of the inferior glenohumeral ligament complex. To obtain an accurate assessment of true glenohumeral rotation, the scapula is stabilized during examination. A loss of 20 degrees or more of internal rotation, as measured with the shoulder positioned in 90 degrees of abduction, indicates excessive tightness of the posterior band of the inferior glenohumeral ligament complex. Burkhart SS, Morgan CD, Kibler WB: The disabled throwing shoulder: Spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 2003;19:404-420.
Question 28
Figure 8 shows the radiograph of a 76-year-old man who has knee pain and swelling. History reveals that he underwent total knee arthroplasty 18 years ago. What is the most likely diagnosis?

Explanation
The radiograph reveals complete loss of joint space with particulate metal debris consistent with total polyethylene failure and metal-on-metal articulation. The components appear to be well fixed and minimal osteolysis is evident. Kilgus DJ, Moreland JR, Finerman GA, et al: Catastrophic wear of tibial polyethylene inserts. Clin Orthop Relat Res 1991;273:223-231.
Question 29
A 43-year-old woman is referred after excisional biopsy of a cutaneous soft-tissue mass from her left shoulder. Based on the biopsy specimens shown in Figures 44a and 44b, what is the best course of action?


Explanation
Dermatofibrosarcoma protuberans (DFSP) is a rare superficial sarcoma that is frequently misdiagnosed at presentation. It is frequently excised prior to suspecting that the lesion is a sarcoma and if not appropriately treated with tumor bed resection to obtain wide margins, these lesions have a high incidence of local recurrence. It is recommended that the wide excision include the deep fascia and a 2.5- to 3-cm cuff of normal-appearing skin. Distant disease spread is rare and usually occurs in the face of a multiply recurrent lesion. Despite the apparent gross circumscription of these lesions, the tumor diffusely infiltrates the dermis and subcutaneous tissues. A characteristic histologic finding can be seen in the deep margins of the tumor where it intricately interdigitates with normal fat. Lindner NJ, Scarborough MT, Powell GJ, et al: Revision surgery in dermatofibrosarcoma protuberans of the trunk and extremities. Eur J Surg Oncol 1999;25:392-397.
Question 30
Figures 22a and 22b show the radiograph and sagittal MRI scan of the upper cervical spine of a 62-year-old woman who has had a long history of rheumatoid arthritis. Following hospitalization and skeletal traction, her symptoms improve significantly, her neurologic examination returns to normal, and repeat radiographs show a normal occiput and C1-C2 relationship. Treatment should now include


Explanation
Although opinions differ on whether a decompression is indicated in a patient with symptomatic basilar invagination, it is generally agreed that occipitocervical stabilization is indicated. This has been done with and without concomitant arthrodesis. Crockard HA, Grob D: Rheumatoid arthritis upper cervical involvement, in Clark CR (ed): The Cervical Spine, ed 3. Philadelphia, PA, Lippincott Raven, 1998, p 701.
Question 31
Figures 2a and 2b show the clinical photograph and radiograph of a 16-year-old cheerleader who fell on her left lower extremity while performing a pyramid. Following adequate sedation, closed reduction is performed, but an incomplete reduction is noted. What structure is most likely preventing a reduction?


Explanation
The stretched peroneus brevis muscle and tendon follow anterior to the fibula and are most likely incarcerated with reduction. The anterior talofibular ligament is too small to prevent reduction of the ankle joint itself. The extensor digitorum brevis originates from the talus; therefore, it is not involved in the tibiotalar joint. The posterior tibial tendon lies medially and would not be interposed into the ankle joint. Similarly, the anterior tibialis tendon also would not be involved. Pehlivan O, Akmaz I, Solakoglu C, et al: Medial peritalar dislocation. Arch Orthop Trauma Surg 2002;122:541-543.
Question 32
A 21-year-old collegiate pitcher has had pain in his dominant shoulder for the past 3 months despite management consisting of rest, rehabilitation, and an analysis of throwing mechanics. An arthroscopic photograph from the posterior portal is shown in Figure 10. The biceps anchor to the bone was not detached to probing. Treatment of the lesion to the left of the cannula should consist of arthroscopic

Explanation
The lesion is a variation of a type I superior labrum anterior and posterior lesion; therefore, appropriate treatment is simple debridement. Biceps tenodesis or release is not indicated because the biceps tendon and anchor are intact. There is no indication for labral repair or capsulorraphy. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 261-270.
Question 33
A 35-year-old woman who is training for a triathlon has had a 2-month history of heel pain with weight bearing and is unable to run. History reveals that she is amenorrheic. Examination reveals that she is thin and has pain over the heel that is exacerbated with medial and lateral compression. Range of motion and motor and sensory function are normal. Radiographs are normal. What is the most likely diagnosis?

Explanation
The most likely diagnosis is a stress fracture of the calcaneus and is supported by the history of running, female gender, and amenorrhea. Reproducing pain with medial and lateral compression of the heel also supports the diagnosis. A bone scan or MRI would most likely confirm the diagnosis. Plantar fasciitis would result in pain on the bottom of the heel with point tenderness. The lack of other areas of involvement or other symptoms does not support a seronegative inflammatory arthritis. Tarsal tunnel syndrome and peripheral neuropathy are unlikely because of the normal neurologic examination. Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 597-612.
Question 34
A 78-year-old man being seen for routine follow-up studies reports mild to moderate pain in his left arm. The patient has a history of lung cancer and severe heart disease. A radiograph and a bone scan are shown in Figures 36a and 36b. Treatment should consist of


Explanation
The patient has lung cancer metastatic to the left humerus that is mildly to moderately symptomatic. Radiographically, the lesion is small and is not associated with significant cortical destruction. Metastatic lesions in the upper extremity have a lower incidence of pathologic fracture than lesions in the lower extremity.
Question 35
The sartorius muscle is innervated by which of the following nerves?

Explanation
The femoral nerve enters the thigh behind the inguinal ligament, lying on the surface of the iliopsoas muscle lateral to the femoral artery and vein. The nerve divides into numerous muscular and cutaneous branches in the femoral triangle. The first motor branch (sometimes two branches) is to the sartorius. There is a variable branch to the pectineus. Subsequent branches go to the rectus femoris and then the vastus muscles in variable order. The last motor branch is to the articularis genu. The muscular branches can be injured in anterior approaches to the hip, especially the middle window of the ilioinguinal approach. Hollinshead WH: Textbook of Anatomy, ed 3. Hagerstown, MD, Harper and Row, 1974, p 404.
Question 36
A healthy, active, independent 74-year-old woman fell and sustained the elbow injury shown in Figures 41a and 41b. Management should consist of


Explanation
Open reduction and internal fixation of distal humeral fractures in elderly patients often fails. These fractures characteristically have a very small distal segment and poor bone quality, resulting in failure of fixation and nonunion. Nonunion is often painful and functionally debilitating. Total elbow arthroplasty provides good results when used for distal humeral fractures in elderly patients with osteopenic bone and fracture patterns thought to be irreconstructable. Long arm casting may result in union, but the resulting stiffness is unacceptable for an active patient. Elbow arthrodesis has few indications. A sling and range-of-motion exercises will often result in a painful and debilitating nonunion at the fracture site. Frankle MA, Herscovici D Jr, DiPasquale TG, et al: A comparison of open reduction and internal fixation and primary total elbow arthroplasty in the treatment of intra-articular distal humerus fractures in women older than 65. J Orthop Trauma 2003;17:473-480. Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humerus fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Question 37
Figures 45a and 45b show the AP and lateral radiographs of a 15-year old patient who is undergoing surgery to add 3 cm of length to the femur. Based on the radiographic findings, what is the next most appropriate step in management?


Explanation
Because the radiographs reveal poor regenerate bone, especially anteriorly and laterally, the first step in management is to slow the distraction rate. If this does not solve the problem, temporary reversal of the distraction, or "accordionization," can be used to induce a greater healing response. Maintaining the same distraction rate will further impair regenerate formation and delay healing. Bone grafting should be reserved as an option if decreasing the distraction rate or alternating a week of compression with a week of distraction fails to improve the callus formation. Repeat corticotomy is performed in patients with premature consolidation. Raney EM: Limb-length discrepancy, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1519-1526.
Question 38
A 35-year-old man sustained the closed injury shown in Figure 52 in his dominant extremity. Neurologic function is normal. Treatment should consist of

Explanation
Functional bracing has been demonstrated to have a very high rate of healing without any functional limitations in a large series of patients. Surgery is reserved for "floating elbows," open injuries, neurovascular injuries, and those fractures that go on to nonunion. Sarmiento A, Zagorski JB, Zych GA, et al: Functional bracing for the treatment of fractures of the humeral diaphysis. J Bone Joint Surg Am 2000;82:478-486.
Question 39
Which of the following structures are found in the anterior tarsal tunnel?
Explanation
The contents of the anterior tarsal tunnel are the extensor hallucis longus, tibialis anterior, extensor digitorum longus, dorsalis pedis artery, and the deep peroneal nerve. The term "anterior tarsal tunnel syndrome" is used to specifically describe the compression of the deep peroneal nerve under the inferior extensor retinaculum. With nerve compression, patients report a burning sensation across the dorsum of the foot with paresthesias in the first web space. There also may be wasting and weakness of the extensor digitorum brevis. Kuritz HM: Anterior entrapment syndromes. J Foot Surg 1976;15:143-148.
Question 40
An 18-year old man has a simple oblique fracture of the humeral shaft that requires surgical stabilization to maintain reduction and facilitate mobilization. Which of the following methods will provide the best outcome?

Explanation
The patient has a simple fracture pattern that can be reduced anatomically and stabilized with absolute stability by interfragmental compression and protection plating. This will guarantee a 95% to 98% union rate with no radial nerve palsy. Intramedullary nailing does not equal these results in a simple fracture pattern in the humerus. Bridge plating is indicated for multifragmented fracture patterns when anatomic reduction and absolute stability cannot be achieved. External fixation is reserved for severe open fractures. Chapman JR, Henley MP, Agel J, Benca PJ: Randomized prospective study of humeral shaft fracture fixation: Intramedullary nails versus plates. J Orthop Trauma 2000;14:162-166. Farragos AF, Schemitsch EH, McKee MD: Complications of intramedullary nailing for fractures of the humeral shaft: A review. J Orthop Trauma 1999;13:258-267.
Question 41
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?

Explanation
Pollak and associates found that the average SF-36 score for patients who sustained a pilon fracture was significantly lower than patients with diabetes mellitus, AIDS, hypertension, asthma, migraines, pelvic fracture, polytrauma, and AMI. Moreover, patients having undergone pilon fixation scored lower on all but three of the SF-36 scales (vitality, mental health, and emotional health).
Question 42
A 75-year-old woman reports foot pain and states that her foot has become progressively "flatter" in the past 3 years. Custom inserts and physical therapy have failed to provide relief. Examination reveals a flexible hindfoot and mild heel cord contracture. The patient is able to perform a single limb heel rise. Weight-bearing radiographs are shown in Figures 21a through 21d. What is the most appropriate surgical management?




Explanation
The patient has end-stage midfoot arthritis, with a secondary flatfoot deformity through the midfoot. The ability to perform a single limb heel rise indicates that the posterior tibial tendon is functioning, and the weight-bearing radiographs show normal calcaneal pitch and talar head coverage, thus confirming that the flatfoot deformity is isolated to the midfoot. Therefore, the most appropriate treatment is medial column arthrodesis and heel cord lengthening. The other listed procedures are not indicated because they are used in the management of adult flatfoot from posterior tibial tendon insufficiency. Toolan BC: Midfoot arthrodesis: Challenges and treatment alternatives. Foot Ankle Clin 2002;7:75-93.
Question 43
Examination of a 28-year-old woman reveals a moderate hallux valgus deformity and a prominence of the medial eminence. She reports that she can participate in all activities, wear 3-inch heels with minimal discomfort, and walk in a 1-inch heel with no pain. However, she is concerned that the deformity will get worse and requests recommendations regarding surgical correction. What is the best course of action?
Explanation
Because the patient is essentially asymptomatic, the most appropriate course of action is observation. Prophylactic hallux valgus surgery is not medically indicated. Steroid injection would only risk infection, as well as joint and capsule damage. There are no data to support the use of a custom orthosis to delay the progression of a hallux valgus deformity. Special shoe wear or an extra-depth shoe is not necessary and is unlikely to be accepted by the patient. Donley BG, Tisdel CL, Sferra JJ, Hall JO: Diagnosing and treating hallux valgus: A conservative approach for a common problem. Cleve Clin J Med 1997;64:469-474.
Question 44
A 39-year-old man reports low back pain, lower extremity numbness, and urinary retention after being injured in a motor vehicle accident 1 day ago. He is able to walk but is in pain. A straight leg raise results in increased back pain, and examination reveals that perianal sensation is decreased. Placement of a urinary catheter results in 500 mL of urine. What is the next most appropriate step in management?
Explanation
Acute cauda equina syndrome, including saddle hypesthesia and bowel/bladder incontinence, is a red flag that demands emergent evaluation with MRI and urgent surgery if compression is confirmed. Results appear to be improved if surgery is performed within 48 hours. The other treatment approaches listed are not indicated if a cauda equina syndrome is present. Ahn UM, Ahn NU, Buchowski JM, et al: Cauda equina syndrome secondary to lumbar disc herniation: A meta-analysis of surgical outcomes. Spine 2000;25:1515-1522. Shapiro S: Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine 2000;25:348-351.
Question 45
A 21-year-old football player had severe pain and immediate swelling in the left anteromedial chest wall while bench pressing near maximal weights several days ago. Examination at the time of injury revealed a mass on the anteromedial chest wall. Follow-up examination now reveals decreased swelling, and axillary webbing is observed. The patient has weakness to adduction and forward flexion. The injured muscle originates from the
Explanation
The patient has a pectoralis major rupture, an injury that occurs most commonly during weight lifting. Grade III injuries represent complete tears of either the musculotendinous junction or an avulsion of the tendon from the humerus, the most common injury site. Examination will most likely reveal ecchymoses and swelling in the proximal arm and axilla, and strength testing will show weakness with internal rotation and in adduction and forward flexion. Axillary webbing, caused by a more defined inferior margin of the anterior deltoid as the result of rupture of the pectoralis, can be seen as the swelling diminishes. Surgical repair is the treatment of choice for complete ruptures. Nonsurgical treatment is associated with significant losses in adduction, flexion, internal rotation, strength, and peak torque. The pectoralis major originates from the proximal clavicle and the border of the sternum, including ribs two through six. The pectoralis major inserts (rather than originates) on the humerus. The coracoid process is the insertion site for the pectoralis minor, as well as the origin for the conjoined tendon. The pectoralis major has no attachment or origin from the scapula. The anterior deltoid originates from the lateral one third of the clavicle and the anterior acromion. Miller MD, Johnson DL, Fu FH, Thaete FL, Blanc RO: Rupture of the pectoralis major muscle in a collegiate football player: Use of magnetic resonance imaging in early diagnosis. Am J Sports Med 1993;21:475-477.
Question 46
In the spine, osteoblastomas usually originate in the

Explanation
Osteoblastomas are benign lesions that represent less than 5% of benign bone tumors. Most lesions are located in the spine, followed by the femur, tibia, and skull. Patients with spinal lesions usually have pain that may be associated with scoliosis. The most common location in the spine is within the posterior elements.
Question 47
A 55-year-old man reports increasing weakness in his arms that has progressed to his lower limbs, resulting in frequent tripping and falling. Examination reveals weakness in shoulder abduction and external and internal rotation bilaterally. Fasciculation is noted. He also has weakness in elbow flexion and extension bilaterally, and his grip strength is diminished. An electromyogram and nerve conduction velocity studies show decreased amplitude of compound motor action potential, slightly slowed motor conduction velocity, and denervation signs with decreased recruitment in all extremities. The sensory study is normal. Based on these findings, what is the most likely diagnosis?

Explanation
The major determinant of ALS (Lou Gehrig disease) is progressive loss of motor neurons. The loss usually begins in one area, is asymmetrical, and later becomes evident in other areas. The first signs of ALS may include either upper or lower motor neuron loss. Recognition of upper motor neuron involvement depends on clinical signs, but electromyography and nerve conduction velocity studies can help identify lower motor neuron involvement. Electrodiagnostic abnormalities in three or more areas are required to make a definitive diagnosis. The motor unit potentials (MUPs) changes in ALS include impaired MUPs recruitment, unstable MUPs, and abnormal MUPs size and configuration. A number of abnormal spontaneous discharges can occur with ALS, especially fibrillation potentials and fasciculation potentials. In ALS, the motor nerve conduction study will be abnormal, but a co-existing normal sensory study is definitive for this disease. de Carvalho M, Johnsen B, Fuglsang-Frederiksen A: Medical technology assessment: Electrodiagnosis in motor neuron diseases and amyotrophic lateral sclerosis. Neurophysiol Clin 2001;31:341-348. Daube JR: Electrodiagnostic studies in amyotrophic lateral sclerosis and other motor neuron disorders. Muscle Nerve 2000;23:1488-1502.
Question 48
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child's ability to walk in the future?
Explanation
For the parachute test, the examiner holds the child prone and then lowers the child rapidly toward the floor. The parachute reaction is normal or positive if the child reaches toward the floor. The Moro or startle reflex should not be present beyond age 6 months. Asymmetric tonic neck reflex, extensor thrust, and absent foot placement are abnormal findings at any age. Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Question 49
A 54-year man has left shoulder pain and weakness after falling while skiing 4 months ago. Examination reveals full range of motion passively, but he has a positive abdominal compression test and weakness with the lift-off test. External rotation strength with the arm at the side and strength with the arm abducted and internally rotated are normal. MRI scans are shown in Figures 1a and 1b. Treatment should consist of


Explanation
The examination findings are consistent with subscapularis muscle weakness but normal supraspinatus and infraspinatus strength. The lift-off test and abdominal compression test are specific for subscapularis function. The MRI scan reveals a chronic avulsion and retraction of the subscapularis. The transverse image reveals a normal infraspinatus muscle, and the sagittal image reveals an atrophic subscapularis. Surgical repair of the isolated subscapularis tendon is indicated. Iannotti JP, Williams GR: Disorders of the Shoulder: Diagnosis and Management, ed 1. Philadelphia, PA, Lippincott Williams & Wilkins, 1999, pp 31-56.
Question 50
Figures 15a and 15b show the radiographs of an 18-year-old mountain biker who came off of a 15-foot ramp and sustained an injury to his ankle. Because the local rural hospital had no orthopaedic surgeon available, he was transported to a Level 1 emergency department 10 hours after his initial injury. Examination reveals that the injury remains closed. Management should consist of


Explanation
High-energy tibial pilon fractures involve disruption of the soft-tissue envelope with significant lower extremity edema. Definitive reconstruction of the comminuted distal tibia should be delayed for at least 7 days to allow edema to dissipate, lowering the risk of skin necrosis. An external fixator is the best method to keep the ankle at anatomic length while preventing skin necrosis. Ligamentotaxis will hold the fragments reduced to allow the edema to dissipate. CT may be obtained in traction to localize the individual fragments and plan surgical incisions and subsequent fixation. Short leg casting will not provide adequate ligamentotaxis to hold the fragments reduced and prevent skin compromise. Primary fusion of the ankle in an unstable tibial pilon fracture is prone to a poor result from nonunion or malunion. Tornetta P III, Weiner L, Bergman M, et al: Pilon fractures: Treatment with combined internal and external fixation. J Orthop Trauma 1993;7:489-496.
Question 51
The correct starting point for an external fixation half pin placed into the anterior inferior iliac spine (AIIS) is labeled by what letter in Figure 3?

Explanation
Half pins placed in the AIIS are an alternative to pins placed in the iliac crest. A strong pillar of bone runs from the AIIS to the posterior iliac crest and less soft tissue is typically present in this area. The starting point is best seen on an obturator outlet view. The obturator outlet view is a combination of the pelvic outlet view and the obturator view of Judet and Letournel. The beam is rotated "over the top" of the patient since the iliac wing is externally rotated as well as cephalad to best visualize this column of bone running from the AIIS to the posterior iliac spine. This corridor of bone will appear as a teardrop. Once the correct view is obtained, the pin should be started at least 2 cm proximal to the hip joint to avoid placing a pin within the hip capsule. Blunt dissection and a guide sleeve should be used to prevent damage to the lateral femoral cutaneous nerve. An iliac oblique view is used after the pin has been partially inserted to make sure the pin is passing superior to the superior gluteal notch, and an obturator inlet view can be used at the completion of the procedure to make sure the pin is contained within the bone for its entire length. Gardner MJ, Nork SE: Stabilization of unstable pelvic fractures with supra-acetabular compression external fixation. J Orthop Trauma 2007;21:269-273. Haidukewych GJ, Kumar S, Prpa B: Placement of half-pins for supra-acetabular external fixation: An anatomic study. Clin Orthop Relat Res 2003;411:269-273.
Question 52
A 12-year-old girl has bilateral developmentally dislocated hips. History reveals no previous treatment, and she reports no discomfort. Good long-term clinical results are most likely to occur with
Explanation
The natural history of complete developmental dislocation of the hip is dependent on two factors: bilaterality and the presence or absence of a false acetabulum. Patients with bilateral dislocations may have low back pain because of hyperlordosis, but they tend to have less disability than patients with unilateral dislocations who have secondary problems related to limb-length inequality. Degenerative joint disease and clinical disability are most likely to develop in patients with completely dislocated hips and well-developed false acetabula. In a 12-year-old child who has bilateral developmental hip dislocations, it would be difficult to obtain surgical treatment results that are better than the natural history of the disorder. Abductor strengthening exercises are unlikely to influence the long-term outcome in this disorder. Surface replacements are not indicated in young asymptomatic patients. Weinstein SL: Natural history of congenital hip dislocation (CDH) and hip dysplasia. Clin Orthop 1987;225:62-76.
Question 53
The use of posting (a wedge added to the medial or lateral side of an insole) is useful to balance forefoot or hindfoot malalignment. Assuming normal subtalar joint pronation, what is the maximum amount of recommended hindfoot posting?

Explanation
Generally, patients cannot tolerate more than 5 degrees of hindfoot posting. Donatelli RA, Hurlbert C, Conaway D, et al: Biomechanics foot orthotics: A retrospective study. J Orthop Sports Phys Ther 1988;10:205-212. Michaud TM: Foot Orthoses and Other Forms of Conservative Foot Care. Baltimore, MD, Williams & Wilkins, 1993, pp 61-65, 186.
Question 54
Myositis ossificans is a recognized complication of contusion to the quadriceps muscle. During early rehabilitation, this condition is most likely to be exacerbated by
Explanation
Passive stretching is contraindicated during rehabilitation as it may potentiate the severity of the myositis ossificans. Electrical stimulation, iontophoresis, isometric exercise, and ice/heat contrast are not known to exacerbate this process. Brunet ME, Hontas RB: The thigh, in DeLee JC, Drez D (eds): Orthopaedic Sports Medicine. Philadelphia, PA, WB Saunders, 1994, pp 1086-1112.
Question 55
Figure 53 shows the arteriogram of a 45-year-old man who has severe vasculitis. What do the findings show?

Explanation
The arterial supply to the hand is abundant and normally duplicated. The deep palmar arch as shown in this arteriogram typically receives its primary contribution from the radial artery which travels deep to the first dorsal compartment tendons and then returns to the volar aspect of the palm through the first web space. The superficial palmar arch receives its supply from the ulnar artery and is not visualized in this patient.
Question 56
What is the most commonly reported complication following elbow arthroscopy?

Explanation
The complication rate following elbow arthroscopy is reported at 5%. The most commonly reported complication is transient neurapraxia, with nerve transection remaining an unfortunate and rare event. While infection remains the most common serious complication, it is uncommon (0.8%). Synovial cutaneous fistula and compartment syndrome, while reported, are the least frequent complications of elbow arthroscopy. Kelly EW, Morrey BF, O'Driscoll SW: Complications of elbow arthroscopy. J Bone Joint Surg Am 2001;83:25-34.
Question 57
Patients with tarsal tunnel syndrome are most likely to obtain a favorable outcome from decompression of the posterior tibial nerve if which of the following conditions is present?
Explanation
In one series, only 44% of patients demonstrated good results from tarsal tunnel decompression if they did not have a mass in the tarsal tunnel. Conditions that produce a traction neuropathy of the posterior tibial nerve are unlikely to respond to neurolysis. The most favorable condition associated with a good response to decompression is when a compressing anatomic structure can be removed from the tarsal tunnel. Frey C, Kerr R: Magnetic resonance imaging and the evaluation of tarsal tunnel syndrome. Foot Ankle 1993;14:159-164. Garrett AL: Poliomyelitis, in Nickel VL (ed): Orthopaedic Rehabilitation. New York, NY, Churchill Livingston, 1982, pp 449-458.
Question 58
The injection shown in Figures 1a and 1b would most benefit a patient who reports which of the following symptoms?


Explanation
The images demonstrate a L5 selective root block as it exits the L5-S1 foramen. This root block best helps relieve pain or paresthesias in the L5 distribution, which is the dorsal first web space and the great toe. The lateral foot is an S1 distribution and would need to be blocked through the posterior first sacral foramen. The anterior shin and thigh represent the L4 root which exits a level above this at the L4-5 foramen. A stocking distribution is nonanatomic and not indicative of a specific root. Magee D: Principles and concepts, in Orthopaedic Physical Assessment, ed 3. Philadelphia, PA, WB Saunders, 1997, pp 1-18.
Question 59
A 21-year-old hockey player who has recurrent shoulder subluxations undergoes an anterior capsulorrhaphy under general anesthesia, and an interscalene block is used to relieve postoperative pain. At the 1-week follow-up examination, he reports loss of sensation over the lateral region of the shoulder and is unable to actively contract the deltoid muscle. The remainder of the examination is normal. What is the best course of action at this time?
Explanation
The patient has an axillary nerve injury, which is relatively uncommon after surgery for instability. This type of injury generally is the result of a stretch injury rather than transection or a hematoma. Therefore, observation is indicated in the early postoperative period. After approximately 6 weeks, electromyography can be used to confirm and document the point of injury. Interscalene blocks can cause prolonged nerve injury but usually are not limited to the axillary nerve.
Question 60
Which of the following findings is likely to be pathologic in a thin, well-conditioned endurance athlete?
Explanation
Left ventricular hypertrophy by voltage is a nonspecific diagnosis, especially in athletes with an asthenic body habitus. High vagal tone in endurance athletes may result in first degree or even type I second degree (ie, Wenckebach) AV block in endurance athletes. High vagal tone results in resting sinus bradycardia in many trained athletes. A I-II/IV systolic ejection murmur is occasionally found in healthy athletes; however, when the murmur increases in intensity with maneuvers that decrease ventricular filling, such as standing or the Valsalva maneuver, dynamic obstruction that is the result of hypertrophic obstructive cardiomyopathy should be suspected. Nonspecific STT wave changes in the lateral leads on ECG are not uncommon in highly trained athletes; thus, they are nonspecific for ischemic heart disease. Pelliccia A, Maron BJ, Culasso F, DiPaolo FM, et al: Clinical significance of abnormal electrocardiographic patterns in trained athletes. Circulation 2000;102:278-284.
Question 61
The arrow in Figure 11 points toward a finding consistent with which of the following?

Explanation
The finding of a unilateral absent pedicle is often referred to as a winking owl sign and is a manifestation of pedicle destruction from metastatic disease. As the vertebral body is destroyed from the neoplastic process, it extends into the pedicle and destroys the cortical rim that normally creates the oval ring of the pedicle on an AP image. McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Question 62
A 50-year-old woman who underwent a joint replacement of the hallux metatarsophalangeal joint 6 months ago now has pain and swelling about the great toe. Radiographs are shown in Figures 39a and 39b. What is the next most appropriate step in management?


Explanation
The radiographs show displacement of the prosthesis, and there has been large amounts of bone resected to insert the implant. Arthrodesis is indicated with interposition bone graft to stabilize the joint and restore length to the first ray.
Scientific References
-
:
Question 63
A 70-year-old woman is brought to the emergency department with a two-part greater tuberosity fracture with an anterior subcoracoid dislocation. One day after successful closed reduction, examination reveals marked swelling of the involved arm, forearm, and hand, as well as large amounts of "weeping" serous fluid but no obvious lacerations. The fingers are warm and pink, and the pulses are normal distally with good refill. Edema is present. There is no pain with passive and active motion of the elbow, wrist, and fingers. What is the next most appropriate step in management?
Explanation
Although not as common as arterial injury, venous thrombosis secondary to trauma of the subclavian or axillary vein can be problematic; therefore, venous duplex ultrasound scanning is the diagnostic study of choice. Arteriography may not show venous thrombosis in the venous run-off phase. The clinical history does not fit the usual presentation of a compartment syndrome or complex regional pain syndrome.
Question 64
Examination of a 7-year-old boy reveals 20 degrees of valgus following a lawn mower injury to the lateral femoral epiphysis. Treatment consists of total distal femoral epiphyseodesis and varus osteotomy. Following surgery, he has a limb-length discrepancy of 3 cm and 5 degrees of genu valgum. Assuming that he undergoes no further treatment, the patient's predicted limb-length discrepancy at maturity would be how many centimeters?
Explanation
The distal femoral epiphysis grows approximately 1 cm per year and in boys, growth ceases at approximately age 16 years. Therefore, the patient's limb-length discrepancy at maturity would be 12 cm (9 cm plus the 3-cm discrepancy he has from the previous surgery). Little DG, Nigo L, Aiona MD: Deficiencies of current methods for the timing of epiphyseodesis. J Pediatr Orthop 1996;16:173-179.
Question 65
A 52-year-old woman reports the sudden onset of intense pain in the right shoulder. She denies any history of injury or previous shoulder problems. At a 2-week follow-up examination, she notes that the pain has decreased, but she now has severe weakness of the external rotators and abductors. Her cervical spine and remaining shoulder examination are otherwise unremarkable. Radiographs of the shoulder and neck are normal. What is the most likely diagnosis?

Explanation
Patients with brachial neuritis or Parsonage-Turner syndrome usually report the sudden onset of intense pain that subsides in 1 to 2 weeks, followed by weakness for a period of up to 1 year in the muscle that is supplied by the involved nerve. Calcific tendinitis usually can be diagnosed radiographically, with calcium deposits seen in the rotator cuff. Bursitis and rotator cuff tendinosis usually are seen after an increase in activity, and both decrease with rest and medication. Glenohumeral arthritis is a slow, progressive problem that results in a loss of range of motion. Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
Question 66
Which of the following is a true statement regarding thoracic disk herniations?
Explanation
Symptomatic herniations of the thoracic spine are much less common than those of the cervical or lumbar region. They tend to occur most commonly during the third to fifth decades of life and although they can be found at all levels, they are most common in the lower third near the thoracolumbar region. Posterior laminectomy and disk excision has the highest rate of neurologic deterioration and is not recommended. Multiple studies have shown that herniated thoracic disks can be found at one or more levels in 40% of asymptomatic individuals. Shah RP, Grauer JN: Thoracoscopic excision of thoracic herniated disc, in Vaccaro AR, Bono CM (eds): Minimally Invasive Spine Surgery. New York, NY, Informa Healthcare, 2007, pp 73-80.
Question 67
Metal-on-metal articulation has been reintroduced because of concern about polyethylene wear. This type of articulation is considered favorable because
Explanation
The improvements in metal-on-metal bearing surfaces come from the nonlinear wear rate and smaller particle size of the high carbon wrought material. Extremely low rates of wear have been demonstrated with high carbon metal-on-metal implants. There is no significant electrochemical effect of mating two like materials in vivo.
Question 68
What nerve is at greatest risk of harm from the portal shown in Figure 36?

Explanation
The figure shows the anterolateral portal for elbow arthroscopy, and injury to the radial nerve has been reported in conjunction with this portal site. Studies have shown that closer proximity to the radial nerve is associated with more distal portal sites. The lateral and posterior antebrachial cutaneous nerves are both at less risk of injury. The ulnar and median nerves are both fairly remote to this location. Field LD, Altchek DW, Warren RF, O'Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607. Papilion JD, Neff RS, Shall LM: Compression neuropathy of the radial nerve as a complication of elbow arthroscopy: A case report and review of the literature. Arthroscopy 1988;4:284-286.
Question 69
Figures 44a and 44b show the radiographs of a 28-year-old woman who has had progressive hip pain for the past 3 months. What is the most likely diagnosis?


Explanation
The patient has multiple hereditary exostoses and a secondary chondrosarcoma arising from a proximal femoral exostosis. The radiograph of the knee shows multiple osteochondromas typical in a patient with multiple hereditary exostoses. Patients with this diagnosis are at an increased risk for malignant degeneration of an osteochondroma. The lateral radiograph of the hip shows a bony lesion emanating from the anterior aspect of the femoral neck that is not well defined in the surrounding soft tissues. There are punctate calcifications and a large soft-tissue mass. The most likely diagnosis is a secondary chondrosarcoma developing from a benign osteochondroma. An enchondroma is an intramedullary benign cartilage lesion. Ollier's disease and Maffucci's syndrome involve multiple enchondromas. Scarborough M, Moreau G: Benign cartilage tumors. Orthop Clin North Am 1996;27:583-589.
Question 70
A 28-year-old hockey player has a shoulder deformity after being checked into the boards. Examination reveals that swelling has improved, but there is tenderness along the distal clavicle. Radiographs reveal a grade II acromioclavicular joint separation. Initial management should consist of
Explanation
The most common shoulder injury in hockey players is to the acromioclavicular joint. Early rest and control of pain and inflammation is the preferred management. Surgery is reserved for patients with significant coracoclavicular disruption that has failed to respond to nonsurgical management. Cross-chest stretches and overhead exercises may increase symptoms. A cortisone injection within the glenohumeral joint will have little effect. Nuber GW, Bowen MK: Acromioclavicular joint injuries and distal clavicle fractures. J Am Acad Orthop Surg 1997;5:11-18.
Question 71
A 13-year-old boy has pain and a firm mass in his left knee. A radiograph and MRI scan are shown in Figures 2a and 2b, and a biopsy specimen is shown in Figure 2c. Based on these findings, what is the most likely diagnosis?



Explanation
The most likely diagnosis is osteosarcoma. The imaging studies show an aggressive primary tumor of bone, and the histology slide shows a typical chondroblastic osteosarcoma, with osteoid deposited along the surface of bone trabeculae. Ewing's sarcoma histologically consists of small round blue cells. Osteochondroma and periosteal chondroma can occur near the knee but have different radiographic and histologic patterns. Chondrosarcoma rarely occurs in children. Simon M, Springfield D, et al: Osteogenic sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 267.
Question 72
Figure 49 shows the radiograph of a 3-year-old child with progressive bowlegs. Laboratory studies show a calcium level of 9.5 mg/dL (normal 9.0 to 11.0 mg/dL), a phosphorus level of 4.2 mg/dL (normal 3 to 5.7 mg/dL), and an alkaline phosphatase level of 305 IU/L (normal 104 to 345 IU/L). What is the most likely diagnosis?

Explanation
The patient has bowlegs associated with very wide physes, particularly noted at the hips. The widening of the growth plates is a classic sign of rickets; however, the normal levels of calcium, phosphorus, and alkaline phosphatase rule out both nutritional and hypophosphatemic rickets. Patients with nutritional rickets or hypophosphatemic rickets have hypophosphatemia and increased alkaline phosphatase levels. Jansen metaphyseal dysostosis has very severe radiographic findings that are not found in this patient; however, these radiographic findings are classic for Schmid metaphyseal dysostosis. This disorder is caused by a mutation in the gene for type X collagen, which is found only in the growth plates of growing children. Lachman RS, Rimoin DL, Spranger J: Metaphyseal chondrodysplasia - Schmid type: Clinical and radiographic delineation with a review of the literature. Pediatr Radiol 1988;18:93-102.
Question 73
A 54-year-old man sustained a small superficial abrasion over the left acromioclavicular joint after falling from his bicycle. Examination reveals no other physical findings. Radiographs show a displaced fracture of the lateral end of the clavicle distal to a line drawn vertically to the coracoid process. Management should consist of

Explanation
Displaced clavicular fractures lateral to the coracoid process (Neer type II and III) are best managed nonsurgically with sling immobilization and physical therapy, starting with pendulum exercises and progressing to active-assisted exercises when comfortable. Supervised therapy should be performed for 3 months or until full painless motion is achieved. In one study by Robinson and Cairns, this form of treatment provided patients with a 86% chance of avoiding a secondary reconstructive procedure. Robinson CM, Cairns DA: Primary nonoperative treatment of displaced lateral fractures of the clavicle. J Bone Joint Surg Am 2004;86:778-782.
Question 74
When an adult hip is surgically dislocated for relief of femoro-acetabular impingment, what is the risk of postoperative iatrogenic osteonecrosis?

Explanation
In a report of more than 70 hips treated by surgical dislocation, iatrogenic osteonecrosis failed to develop in any of the hips.
Question 75
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?

Explanation
The tibia has grown into valgus secondary to the proximal fracture. This occurs in about one half of these injuries, and maximal deformity occurs at 18 months postinjury. The deformity gradually improves over several years, with minimal residual deformity. Therefore, treatment at this age is unnecessary as there is a high rate of recurrence and complications regardless of technique. The valgus deformity is not a result of physeal injury or growth arrest. Medial proximal tibial hemiepiphysiodesis is an excellent method of correcting the residual deformity but is best reserved until close to the end of growth. Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482. McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Question 76
A 17-year-old high school football player reports wrist pain after being tackled. Radiographs are shown in Figures 22a through 22c. What is the recommended intervention?



Explanation
The patient has an acute fracture of the proximal pole. A 100% healing rate has been reported for open reduction and internal fixation of proximal pole fractures via a dorsal approach. This allows for direct viewing of the fracture line, facilitates reduction, and bone grafting can be done through the same incision if necessary. A vascularized or corticocancellous graft is reserved for nonunions. Proximal fractures are very slow to heal with a cast, if they heal at all. As a small fragment, percutaneous fixation is very difficult and has been reported for waist fractures. Rettig ME, Raskin KB: Retrograde compression screw fixation of acute proximal pole scaphoid fractures. J Hand Surg Am 1999;24:1206-1210.
Question 77
What is the mechanism of action of an intramuscular injection of botulinum type A toxin in reducing spasticitiy?
Explanation
The use of intramuscular botulinum type A toxin has been shown to be a useful adjuvant in the management of dynamic deformity in patients with cerebral palsy. Botulinum type A toxin is a neurotoxin produced by Clostridium botulinum that works by interfering with presynaptic acetylcholine release at cholinergic nerve terminals. At the cellular level, the mechanism involves endocytosis of the intact botulinum toxin molecule by cells in the end plate, followed by disulfide cleavage and translocation of the light chain into the cytosol where it disrupts the normal binding of the synaptosomal vesicles to the axon terminal membrane. Neither the nerve terminal nor the neuromuscular junction is damaged. The muscle paralysis is reversible and dose-dependent. Baclofen is a neuropharmacologic agent that functions as a GABA agonist. Dorsal rhizotomy is a neurosurgical procedure that reduces spasticity by dividing afferent (excitatory) fibers in the posterior rootlet of the spinal nerves. Koman LA, Mooney JF III, Smith B, Goodman A, Mulvaney T: Management of cerebral palsy with botulinum-A toxin: Preliminary investigation. J Pediatr Orthop 1993;13:489-495.
Question 78
A 12-year-old girl has scoliosis at T5-T10 that measures 62 degrees. A clinical photograph of the axilla is shown in Figure 56. Management should consist of

Explanation
Neurofibromatosis type 1 (NF-1) is an autosomal-dominant disorder affecting about 1 in 4,000 people. NF-1 causes tumors to grow along various types of nerves and affects the development of non-nervous tissues, such as bone and skin. The gene for NF-1 is located on the long arm of chromosome 17 and codes the protein neurofibromin. Research indicates that NF-1 acts as a tumor-suppressor gene and, as such, plays an important role in the control of cell growth and differentiation. Axillary and inguinal freckling is considered a good diagnostic marker for NF-1. The hyperpigmented spots that measure from 2 mm to 4 mm may be congenital, but these typically appear and increase later in life. Scoliosis is the most common musculoskeletal disorder of NF-1. The curves are frequently dystrophic, kyphotic, and have a high risk of pseudarthrosis following spinal fusion. Anterior and posterior spinal fusion with rigid posterior segmental instrumentation is the treatment of choice. Goldberg Y, Dibbern K, Klein J, Riccardi VM, Graham JM Jr: Neurofibromatosis type 1: An update and review for the primary pediatrician. Clin Pediatr 1996;35:545-561.
Question 79
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of

Explanation
Because the radiograph shows that the femoral stem is loose within the femoral canal and there is a fracture in the distal cement mantle, the stem should be revised. The Ogden-type plate and the allograft bone plates will reconstruct the femur but will not restore stability to the stem. Similarly, traction may allow the femur to heal but will not restore stability to the femoral stem within the femur. Resection arthroplasty is considered a salvage option following failure of the other procedures. Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Question 80
Figures 14a and 14b show the initial radiographs of an 18-year-old man who fell while snowboarding. Figures 14c and 14d show the radiographs obtained following closed reduction. Examination reveals that the elbow is stable with range of motion. Management should now consist of




Explanation
The initial radiographs reveal a simple elbow dislocation without associated fractures. After successful closed reduction, the range of stability should be assessed. If the elbow is stable, nonsurgical management should consist of a short period of immobilization followed by range-of-motion exercises. Immobilization for more than 3 weeks results in significant elbow stiffness. Surgical repair is indicated for dislocations that are irreducible, have associated fractures, or where stability cannot be maintained with closed treatment. Cohen MS, Hastings H II: Acute elbow dislocations: Evaluation and management. J Am Acad Orthop Surg 1998;6:15-23.
Question 81
What is the most likely long-term sequela of the injury shown in Figures 47a and 47b?


Explanation
The imaging studies show a comminuted lateral talar process fracture. This injury is often missed on plain radiographs; therefore, CT provides the best method of diagnostic evaluation. The most likely long-term sequela of this injury is subtalar joint arthrosis. Although this injury involves the fibular gutter region, progression to true ankle arthritis is unlikely. There does not appear to be any association with this injury and chronic mechanical instability of the ankle or disruption of the superior peroneal retinaculum and subsequent peroneal tendon instability. Entrapment of the flexor hallucis longus tendon may occur with fractures of the sustentaculum tali but not with injuries of the lateral talar process. Surgical management includes open reduction and internal fixation versus excision; the goal is preservation of the large articular surface fragments. In this patient, there is significant comminution and early fragment excision may be the best option for acute treatment. Tucker DJ, Feder JM, Boylan JP: Fractures of the lateral process of the talus: Two case reports and a comprehensive literature review. Foot Ankle Int 1998;19:641-646.
Question 82
A 25-year-old student sustains the injury shown in Figures 13a through 13c after falling off a curb. Initial management should consist of



Explanation
The radiographs reveal a fracture entering the 4-5 intermetatarsal articulation, consistent with a zone 2 injury. This classically is also referred to as a Jones fracture. The history and radiographic findings indicate this is an acute fracture, which guides management. A zone 1 fracture enters the fifth tarsometatarsal joint, and a zone 3 fracture is a proximal diaphyseal fracture distal to the 4-5 articulation. Initial management is usually nonsurgical and consists of non-weight-bearing in a short leg cast. This method has been shown to result in a better healing rate compared to weight bearing as tolerated. Rosenberg GA, Sterra JJ: Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg 2000;8:332-338.
Question 83
A 60-year-old woman with a history of breast cancer has progressive paraparesis. The MRI scan is shown in Figure 28. What form of management is most likely to restore or maintain ambulation?

Explanation
Surgical decompression and stabilization have been shown to be the most effective means of improving neurologic function. Decompression is most reliably done from the side of the compression, which is anterior in this patient. Harrington KD: Metastatic tumors of the spine: Diagnosis and treatment. J Am Acad Orthop Surg 1993;1:76-86.
Question 84
A 12-year-old boy sustains open comminuted midshaft tibial and fibular fractures while playing indoor soccer. The wound is grossly clean and measures 7 cm with some periosteal stripping. Antibiotics and tetanus toxoid are administered immediately in the emergency department. Following irrigation and debridement of the wound in the operating room, treatment should include

Explanation
Open fractures in children have similar rates of short-term complications such as compartment syndrome, vascular injury, and nerve injury when compared to adult fractures. Primary wound closure should be used for Gustillo and Anderson type 1 or uncomplicated type 2 fractures after surgical debridement. Skeletal stabilization may consist of external fixation, flexible nails, or casting with or without supplementary pin fixation. For an open comminuted midshaft fracture, external fixation is the treatment of choice. Reamed intramedullary nailing is contraindicated in children with an open physis. Plate fixation has a high complication rate in severe open fractures. Jones BG, Duncan RD: Open tibial fractures in children under 13 years of age-10 years experience. Injury 2003;34:776-780. Bartlett CS III, Weiner LS, Yang EC: Treatment of type II and type III open tibia fractures in children. J Orthop Trauma 1997;11:357-362. Robertson P, Karol LA, Rab GT: Open fractures of the tibia and femur in children. J Pediatr Orthop 1996;16:621-626.
Question 85
Figures 11a and 11b show the radiographs of a 50-year-old man who was struck by a car. Treatment should consist of


Explanation
The patient has a displaced femoral neck fracture. Although the treatment remains controversial, most clinicians advocate either a closed or open reduction in younger active patients. Achieving an anatomic reduction is necessary to avoid loss of reduction, nonunion, or osteonecrosis. An acceptable reduction may have up to 15 degrees of valgus angulation and 10 degrees of posterior angulation. Parallel multiple screws or pins are the most common method of internal fixation. Prosthetic replacement is generally reserved for older and less active individuals. Callaghan JJ, Dennis DA, Paprosky WG, et al (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 97-108.
Question 86
A 47-year-old man sustained a degloving injury over the pretibial surface and anterior ankle region in a motor vehicle accident. After debridement and irrigation, there is inadequate tissue for closure of the exposed anterior tibial tendon and tibia. Prior to definitive soft-tissue coverage, management should consist of
Explanation
With soft-tissue loss, local or free flap coverage may be necessary to treat exposed tendon and bone. However, a vacuum-assisted closure device is a good temporizing dressing. It prevents external contamination, reduces edema around the wound, increases oxygen tension in the wound, and promotes the formation of granulation tissue. The use of this negative pressure device has been described in both acute traumatic and in chronic wound scenarios. If sufficient granulation tissue forms, closure may be by split graft, avoiding a more complex coverage procedure. Immediate skin grafting over the exposed anterior tibial tendon and tibia would have a low likelihood of success. Dressing changes with sulfasalazine may be beneficial in a burn wound to assist with removal of skin slough; however, in a granulating wound, the material may be toxic to early epithelialization. Xenograft is a foreign body and should not be applied to an acute contaminated open wound. Historically, a cross-leg flap was a treatment alternative for lower extremity soft-tissue loss; however, its current applications are extremely limited. Webb LX: New techniques in wound management: Vacuum assisted wound closure. J Am Acad Orthop Surg 2002;10:303-311.
Question 87
A 19-year-old wrestler has numbness along the radial aspect of the forearm after undergoing an open Bankart repair through an anterior deltopectoral approach. Motor weakness would be expected along with what other finding?

Explanation
The musculocutaneous nerve may be injured by retracting the conjoined tendon medially. This nerve enters the coracobrachialis 5 cm distal to its origin. Its sensory distribution is the radial forearm, and its motor supply is to the biceps and brachialis. Bach BR, O'Brien SJ, Warren RF, et al: An unusual neurologic complication of the Bristow procedure. J Bone Joint Surg Am 1988;70:458-460.
Question 88
To avoid damage to the ascending branch of the anterior humeral circumflex artery during open reduction and internal fixation of a proximal humeral fracture, the blade plate should be placed in what position?
Explanation
The pectoralis major tendon inserts lateral to the biceps tendon, which runs in the bicipital groove. The primary vascular supply of the articular surface of the humeral head is derived from the anterior circumflex humeral artery, which continues into the arcuate artery once it enters the bone. The entry point is on the anterolateral aspect of the humerus just medial to the greater tuberosity within the bicipital groove. To avoid compromising circulation, the blade plate should be placed lateral to the bicipital groove and pectoralis major tendon insertion. Loebenberg M, Plate AM, Zuckerman J: Osteonecrosis of the humeral head. Instr Course Lect 1999;48:349-357.
Question 89
Which of the following bearing materials is most resistant to scratching from third-body debris?
Explanation
Alumina is the hardest of all the materials listed. Clinical retrieval demonstrates resistance to scratching from third-body debris.
Question 90
Figures 32a and 32b show the radiographs of a 13-year-old boy who sustained a fracture while playing football 1 week ago. Management at the time of injury included application of a cast and the use of crutches. A follow-up office visit reveals a normal neurologic examination, and the patient reports no discomfort with the cast and crutches. Management should now include


Explanation
Stable fractures and minimally displaced fractures in children can and should be treated by closed methods. Because loss of reduction is common, alignment of tibia fractures must be monitored closely for the first 3 weeks after cast application. This is most easily handled in a cooperative patient by cast wedging. Some children require application of a second cast under general anesthesia 2 to 3 weeks after injury, particularly if the subsidence of swelling has caused the cast to loosen. Surgical indications include the presence of soft-tissue injuries, unstable fracture patterns, fractures associated with compartment syndrome, and the child with multiple injuries. Surgical options in children include percutaneous pins, external fixation, plates and screws, and intramedullary nails. Heinrich SD: Fractures of the shaft of the tibia and fibula, in Rockwood CA, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1340-1346.
Question 91
A 28-year-old woman who is an avid runner reports pain about the left hip with activities. Nonsurgical management has failed to provide relief. An MRI arthrogram is shown in Figure 47. What is the most likely diagnosis?

Explanation
The MRI arthrogram reveals dye extravasation into the labrum, consistent with a labral tear. The MRI findings are not typical of osteonecrosis, stress fracture, or transient osteoporosis. There is no increase in bone marrow edema in the neck or femoral head. Guanche CA, Sikka RS: Acetabular labral tears with underlying chondralmalacia: A possible association with high-level running. Arthroscopy 2005;21:580-585.
Question 92
A 16-year-old boy has had a painful ingrown nail on his great toe for the past 3 months. When initial management consisting of soaking the foot in Epsom salts and trimming the nail failed to provide relief, his family physician recommended 2 weeks of oral antibiotics. His symptoms persist, and he is now seeking a second opinion. A clinical photograph is shown in Figure 18. Management should now consist of

Explanation
The patient has a chronic ingrown nail on his great toe, which is not an uncommon occurrence in teenagers because of improper nail care. There is local infection and a foreign body reaction because of the nail. Continued conservative management with soaks and antibiotics will not improve the clinical situation. In the presence of local chronic infection, nail matrix ablation is contraindicated. Additionally, in the absence of a history of an ingrown nail, a nail matrix ablation is not medically indicated. The appropriate treatment is partial removal of the nail plate. With nail plate removal, the inflammation and local infection will resolve rapidly. Pettine KA, Cofield RH, Johnson KA, Bussey RM: Ingrown toenail: Results of surgical treatment. Foot Ankle 1988;9:130-134.
Question 93
The third plantar intrinsic muscle layer of the foot consists of which of the following structures?
Explanation
The plantar intrinsic muscles are divided into four layers with respect to depth from the plantar fascia. They are (from superficial to deep): 1) abductor hallucis, flexor digitorum brevis, abductor digiti minimi; 2) quadratus plantae, lumbricals; 3) flexor digiti minimi, flexor hallucis brevis, adductor hallucis brevis; and 4) dorsal and plantar interosseous muscles. The flexor hallucis brevis and adductor hallucis brevis originate from the midtarsal bones, encompass the sesamoids, and insert into the base of the proximal phalanx. The adductor hallucis brevis consists of two muscle bellies forming a conjoined tendon and inserting into the lateral portion of the proximal phalanx and the lateral sesamoid. The adductor hallucis brevis is stronger than the abductor hallucis brevis, which may contribute to hallux valgus. The flexor digitorum minimi travels under the fifth metatarsal, arising at the base and inserting into the lateral base of the fifth proximal phalanx.
Question 94
A 7-year-old girl who sustained a type III posteromedial extension supracondylar fracture underwent a closed reduction at the time of injury. Figure 27a shows the position of the fracture fragments prior to percutaneous medial and lateral pin fixation. Following surgery, healing was uneventful and the patient regained a full painless range of motion. Fifteen months after the injury, she now reports loss of elbow motion and moderate pain with activity. A current AP radiograph is shown in Figure 27b. What is the most likely cause of her symptoms?


Explanation
The patient sustained a very distal supracondylar fracture of the humerus. Fractures in this area can disrupt the blood vessels supplying the lateral ossification center of the trochlea. With disturbance of the blood supply in this area, local osteonecrosis occurs and disrupts the support for the overlying articular surface, producing joint incongruity and localized degenerative arthritis. Haraldsson S: The interosseous vasculature of the distal end of the humerus with special reference to the capitellum. Acta Orthop Scand 1957;27:81-93.
Question 95
A patient undergoes an arthroscopic debridement for lateral epicondylitis. Postoperatively she reports pain and a sense of clicking of the elbow. Examination reveals apprehension to supination, load, and extension. What structure has been injured resulting in the clinical presentation?
Explanation
The patient has an iatrogenic injury to the lateral ulnar collateral ligament following the arthroscopic procedure. Failure to adhere to known anatomic landmarks can lead to this devastating complication. The examination findings are classic for posterolateral elbow instability. Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 318.
Question 96
Figure 2 shows the radiograph of a 72-year-old woman who reports pain after a fall. History includes several years of increasing thigh pain and limb shortening. Management consisting of an extensive work-up for infection reveals normal laboratory studies, a positive bone scan, and a negative hip aspiration. What is the most likely etiology of this complication?

Explanation
The patient has a midstem periprosthetic fracture, which commonly results in loosening of the prosthesis. Patients who have a large amount of bone loss may require an allograft with the surgical reconstruction. Although the patient reported a fall, her history is also consistent with preexisting loosening of the prosthesis. Chronic infection has been shown in up to 16% of these fractures; however, the patient's work-up revealed no infection. Garbuz DS, Masri BA, Duncan CP: Periprosthetic fractures of the femur: Principles of prevention and management, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 237-242. Bethea JS III, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 97
What complication is frequently associated with the Weil lesser metatarsal osteotomy (distal, oblique) in the treatment of claw toe deformities?
Explanation
Weil osteotomies are useful in achieving shortening of a lesser metatarsal with preservation of the distal articular surface. The osteotomy is oriented from distal-dorsal to proximal-plantar; therefore, proximal displacement of the distal fragment is associated with plantar (not dorsal) displacement as well. Plantar displacement can result in the intrinsics acting dorsal to the center of the metatarsophalangeal joint and the development of an extended or "floating toe." Nonunion, osteonecrosis, and inadequate shortening are infrequent complications associated with the Weil lesser metatarsal osteotomy. Trnka HJ, Nyska M, Parks BG, et al: Dorsiflexion contracture after the Weil osteotomy: Results of cadaver study and three-dimensional analysis. Foot Ankle Int 2001;22:47-50.
Question 98
Figure 30 shows an axial cross section of extensor tendon anatomy in zone 7 of the wrist. What letter best depicts the location of the posterior interosseous nerve?

Explanation
The posterior interosseous nerve in contained in the floor of the fourth dorsal compartment of the wrist, which is labelled C in this diagram. Tubiana R, McCullough CJ, Masquelet AC: An Atlas of Surgical Exposures of the Upper Extremity. Philadelphia, PA, JB Lippincott, 1990, p 224.
Question 99
Osteonecrosis of the humeral head is a rare complication seen after dislocation of the glenohumeral joint in skeletally immature patients. When this complication is encountered, treatment should consist of

Explanation
This rare complication occurs after fracture-dislocation and has been seen after surgical stabilization in the adolescent. In most reported cases, prolonged observation has been shown to result in revascularization. Pateder DB, Park HB, Chronopoulos E, et al: Humeral head osteonecrosis after anterior shoulder stabilization in an adolescent: A case report. J Bone Joint Surg Am 2004;86:2290-2293.
Question 100
A 19-year-old man has had back pain with activity, especially running in soccer and baseball, for the past 4 months. He denies any history of trauma. Examination reveals no motor weakness or sensory changes in the lower extremities. Range of motion shows increased pain with extension and mild limitation with flexion. A sitting straight leg raising test is limited at approximately 60 degrees bilaterally by back and buttocks pain. Plain radiographs are normal. MRI scans are shown in Figures 13a through 13e. What is the most likely diagnosis?





Explanation
The patient has an isthmic spondylolysis. The plain radiographs are normal, but the MRI scans show increased marrow edema and signal at the L5 pars interarticularis. Findings of bilateral hamstring tightness and increased pain with extension over flexion suggests spondylolysis. The MRI scans do not show any signs of the other conditions. Wiltse LL, Rothman SL: Spondylolisthesis: Classification, diagnosis and natural history. Sem Spine Surg 1993;5:264-280.
