Full Question & Answer Text (for Search Engines)
Question 1:
A 20-year-old collegiate volleyball player has vague left, nondominant elbow pain. Five years ago, he sustained a dislocation of the same joint and, while he could participate in his sport, he notes that the elbow 'never felt quite right.` The pain is not severe but prevents him from playing sports and he cannot localize the pain to any specific location. Occasionally he will perceive a catching when pushing himself out of a chair but the elbow never locks in one position. Examination reveals full passive and active range of motion in flexion, extension, supination, and pronation. There is tenderness of the lateral elbow during elbow extension with the forearm supinated and a momentary painful `clunk` is noted. Radiographs and MRI scans are normal. What is the most likely instability? Review Topic
Options:
- Varus
- Valgus
- Longitudinal forearm
- Posteromedial rotatory
- Posterolateral rotatory
Correct Answer: Posterolateral rotatory
Explanation:
Posterolateral rotatory instability of the elbow is seen in athletes and frequently follows a previous injury such as a dislocation where the lateral ulnar collateral ligament becomes weakened and attenuated. The ulna supinates away from the humerus and the radius subluxates posteriorly on the capitellum with the forearm supinated and the elbow in extension. Posteromedial rotatory instability is more often seen in association with fracture of the coronoid process following a varus stress to the elbow. Valgus instability occurs due to an injury to the medial ulnar collateral ligament seen most commonly in throwers from overuse. Varus instability is rare but results in lateral gapping of the elbow. Longitudinal forearm instability is seen after an Essex-Lopresti injury.
Question 2:
A 12-month-old boy has right congenital fibular intercalary hemimelia with a normal contralateral limb. A radiograph of the lower extremities shows a limb-length discrepancy of 2 cm. All of the shortening is in the right tibia. Assuming that no treatment is rendered prior to skeletal maturity, the limb-length discrepancy will most likely
Options:
- remain 2 cm at maturity.
- decrease slowly until the limb lengths equalize.
- increase at a constant rate of 2 cm per year.
- increase markedly because of complete failure of tibial growth.
- increase slowly, with the right lower extremity remaining in proportion to the left lower extremity.
Correct Answer: increase slowly, with the right lower extremity remaining in proportion to the left lower extremity.
Explanation:
DISCUSSION: Many congenital limb deficiencies and bowing deformities result in growth retardation. If unilateral, a gradually progressive limb-length discrepancy will result; however, the proportional lengths of the lower extremities will remain at a relatively constant ratio. For example, if the right foot is at the level of the left knee at birth, this will still be true at maturity. This concept can be useful for early prediction of limb-length discrepancy by using a “multiplier method,” as described by Paley and associates. This method can facilitate early treatment decisions, such as the need for amputation, without having to wait for serial scanography measurements.
REFERENCES: Paley D, Bhave A, Herzenberg JE, et al: Multiplier method for predicting
limb-length discrepancy. J Bone Joint Surg Am 2000;82:1432-1446.
Moseley CF: A straight-line graph for leg length discrepancies. Clin Orthop 1978;136:33-40.
Question 3:
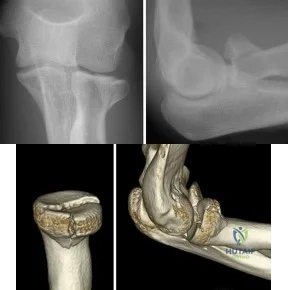
Figures 75a and 75b are the radiographs after attempted reduction of an injury in a 9-year-old girl. Which anatomic structure is most likely to be interposed?
Options:
- Brachialis muscle
- Radial nerve
- Median nerve
- Ulnar nerve
Correct Answer: Ulnar nerve
Explanation:
DISCUSSION
The injury shown is a flexion-type supracondylar humerus fracture. The most commonly interposed anatomic structure is the ulnar nerve. The brachialis muscle is often interposed in extension-type fractures, as are the median nerve and radial artery. The radial nerve is at risk for entrapment in a humeral shaft fracture or distal third humeral fracture.
CLINICAL SITUATION FOR QUESTIONS 76 THROUGH 80
Figure 76 is the clinical photograph of an infant with foot deformities.
Question 4:
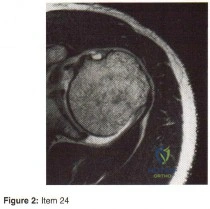
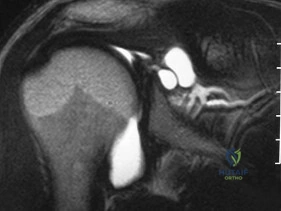
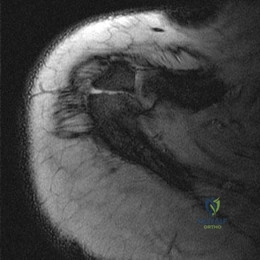
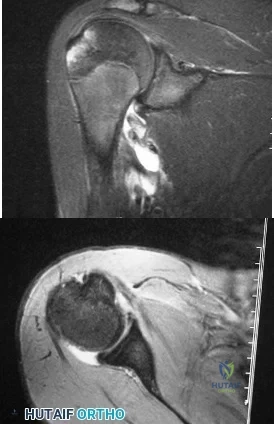
A 25-year-old volleyball player reports pain and clicking in his dominant shoulder during overhand serving. Three months of physical therapy fail to provide relief. Radiographs are normal, and an MRI scan is shown in figures 18a and 18b. Atrophy and weakness are most likely to be localized to which of the following muscles?
Options:
- Deltoid
- Supraspinatus
- Subscapularis Infraspinatus
- Infraspinatus
- Infraspinatus and teres minor
Correct Answer: Infraspinatus
Explanation:
The MRI of the shoulder shows multiple ganglion type cysts of the genoid labrum. These cyst have a correlation with overhead type repeative motion. It has been suggested in the volleyball players that the rapid deceleration after a spike can lead to a SLAP(superior labral) lesion. This in turn can lead to genoid cyst formation. Now remember that the suprascapular nerve comes off the superior trunk of the Brachial plexus, goes under the superortransverse scapular ligament (in the scapular notch, nerve under artery above). It then descends right behind the posterior glenoid/labrum. Therefore, a large cyst in this area will impinge/entrap the nerve. This nerve supplies the infraspinatus muscle and over time will give you atrophy/ pain of this muscle. 87.
Question 5:
The use of nonsteroidal anti-inflammatory drugs following femoral nailing has been associated with which of the following?
Options:
- Increased rate of nonunion
- Decreased narcotic requirements
- Faster time to union
- Increased rate of heterotopic ossification
- Decreased rate of revision surgery
Correct Answer: Increased rate of nonunion
Explanation:
DISCUSSION: The risk of femoral nonunion after intramedullary nailing is significantly increased when NSAIDs are administered post-operatively.
Giannoudis et al assessed factors which could affect union in 32 patients with nonunion of a fracture of the diaphysis of the femur and 67 matched patients whose fracture had united. They found that there was no relationship between the rate of union and the type of implant, mode of locking, reaming, distraction or smoking. They also concluded that there was a marked association between nonunion and the use of NSAIDs after injury and delayed healing was noted in patients who took NSAIDs and whose fractures had united.
Burd et al performed a study to determine if patients with an acetabular fracture, who received indomethacin for prophylaxis against HO, were at risk of delayed healing or nonunion of any associated fractures of long bones. The study group consisted of 112 patients who had sustained at least one concomitant fracture of a long bone; of which 36 needed no prophylaxis, 38 received focal radiation and 38 received indomethacin. When comparing patients who received indomethacin with those who did not, a significant difference was noted in the rate of long bone nonunion (26% vs 7%).
Question 6:
A 19-year-old female field hockey player sustains a right ankle injury last night during a game. The patient is on crutches and reports that she has not been able to put any weight on her right ankle since the injury. She was running alongside with another player when her right ankle “gave out” and she twisted it, falling to the ground. Physical examination reveals discoloration similar to a hematoma and significant swelling around the lateral ankle area. Pain is elicited during palpation of the anterior talofibular ligament. What test should be performed to aid in this diagnosis?
Options:
- Thompson test
- External rotation stress test
- Anterior drawer test
- Squeeze test
Correct Answer: Anterior drawer test
Explanation:
The anterior drawer test is performed with the ankle in 10° of plantar flexion, which results in the greatest amount of translation. The test investigates the integrity of the anterior talofibular ligament with a key distance of translation being 8 to 10 mm. While the patient is sitting and has her knees flexed over the edge of a table or bench, the physician uses one hand to stabilize the distal leg and with the other hand applies an anterior force to the heel in an attempt to gap the talus anteriorly from under the tibia. The anterior talofibular ligament and calcaneofibular ligament are both compromised based on the examination findings. The anterior drawer test result reflects injury to the anterior talofibular ligament and a possible injury to the calcaneofibular ligament. A lateral talar tilt test angle measurement >15° degrees reflects a rupture of both anterior talofibular ligament and calcaneofibular ligaments. The diagnosis is a severe lateral ligament complex sprain. This is optimally managed with early mobilization and a guided rehabilitation program that emphasizes proprioceptive stability.
Question 7:
A 45-year-old man is seeking evaluation of an injury sustained in a motor vehicle accident 10 weeks ago. Current radiographs are shown in Figures 2a and 2b. Based on the radiographic findings, what is the most likely diagnosis?
Options:
- Varus malreduction of the talar neck
- Osteonecrosis of the talar body
- Subtalar traumatic arthropathy
- Nonunion of the talar neck
- Occult infection
Correct Answer: Osteonecrosis of the talar body
Explanation:
DISCUSSION: An increased density of the talar body compared to the distal tibia following fracture of the talar neck is highly suggestive of vascular compromise of the talar body. Subchondral osteopenia of the talus at 6 to 8 weeks (Hawkins sign) is a favorable sign but does not eliminate the possibility of osteonecrosis.
REFERENCES: Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J: Fractures of the talus: Experience of two level 1 trauma centers. Foot Ankle Int 2000;21:1023-1029.
Berlet GC, Lee TH, Massa EG: Talar neck fractures. Orthop Clin North Am 2001;32:53-64.
Question 8:
Injury to the popliteal artery during total knee arthroplasty (TKA) is most likely to occur when placing a sharp retractor
Options:
- directly posterior to the posterior cruciate ligament (PCL).
- posteromedial to the PCL.
- posterolateral to the PCL.
- in the posteromedial corner of the knee.
Correct Answer: posterolateral to the PCL.
Explanation:
DISCUSSION:
Vascular complications during TKA are rare but do occur. Traditionally, it was taught that the popliteal artery was situated posterior to the PCL; however, more recent anatomic dissections have demonstrated that this artery is usually located posterolateral to the PCL.
Question 9:
An operating room intervention that should be undertaken by anesthesia staff during the cementing of a femoral stem is to
Options:
- decrease the fraction of inspired oxygen (FiO2).
- decrease the intravenous (IV) fluid rate.
- have phenylephrine on standby.
- redose epidural anesthesia.
Correct Answer: have phenylephrine on standby.
Explanation:
DISCUSSION
Young age is a risk factor for early failure of cementless femoral components. Surgeons could consider cementing for patients older than 80 years of age. The Dorr classification has been shown to favor a cemented femoral stem in Dorr type C bone. Dorr type B bone can potentially sustain a proximally porous ingrowth stem. Osteoporosis is a risk factor for early failure of cementless femoral components.
Earlier designs for cemented femoral stems used microtexture to interlock the stem into the cement mantle. If these stems became loose, they would abrade the cement and loosen the stem further. Successful cemented femoral components are polished and have smooth edges with tapered bodies. Collars do not add to the design of femoral stems.
Patients are at risk for hypotension during the femoral pressurization process. With that in mind, the surgeon should make sure the anesthesiologist is ready to respond to hypotension. The FiO2 should be increased. The IV fluid rate also should be increased, and the anesthesiologist should be prepared with phenylephrine to support the patient’s blood pressure if he or she becomes hypotensive.
Question 10:
A 6-year-old child sustained a closed nondisplaced proximal tibial metaphyseal fracture 1 year ago. She was treated with a long leg cast with a varus mold, and the fracture healed uneventfully. She now has a 15-degree valgus deformity. What is the next step in management?
Options:
- Proximal tibial/fibular osteotomy with acute correction and pin fixation
- Proximal tibial/fibular osteotomy with gradual correction and external fixation
- MRI of the proximal tibial physis
- Medial proximal tibial hemiepiphysiodesis
- Continued observation
Correct Answer: Continued observation
Explanation:
DISCUSSION: The tibia has grown into valgus secondary to the proximal fracture. This occurs in about one half of these injuries, and maximal deformity occurs at 18 months postinjury. The deformity gradually improves over several years, with minimal residual deformity. Therefore, treatment at this age is unnecessary as there is a high rate of recurrence and complications regardless of technique. The valgus deformity is not a result of physeal injury or growth arrest. Medial proximal tibial hemiepiphysiodesis is an excellent method of correcting the residual deformity but is best reserved until close to the end of growth.
REFERENCES: Brougham DI, Nicol RO: Valgus deformity after proximal tibial fractures in children. J Bone Joint Surg Br 1987;69:482.
McCarthy JJ, Kim DH, Eilert RE: Posttraumatic genu valgum: Operative versus nonoperative treatment. J Pediatr Orthop 1998;18:518-521.
Robert M, Khouri N, Carlioz H, et al: Fractures of the proximal tibial metaphysis in children: Review of a series of 25 cases. J Pediatr Orthop 1987;7:444-449.
Question 11:
A 57-year-old woman experiences pain 1 year after total knee arthroplasty (TKA). She reports sharp anterior pain and a painful catching sensation that is aggravated by rising from a chair or climbing stairs. Physical examination reveals a mild effusion and a range of motion of 2° to 130°, with patellar crepitus. The symptoms are reproduced by resisted knee extension. Radiographs show a well-aligned posterior- stabilized TKA without evidence of component loosening. What is the recommended treatment for this patient?
Options:
- Physical therapy
- Arthroscopic synovectomy
- Tibial insert revision
- Femoral component revision
Correct Answer: Arthroscopic synovectomy
Explanation:
DISCUSSION:
Patellar clunk syndrome is caused by the development of a fibrous nodule on the posterior aspect of the quadriceps tendon at its insertion into the patella. It causes a painful catching sensation when the extensor
mechanism traverses over the trochlear notch as the knee extends from 45° of flexion to 30° from full extension. It characteristically occurs in posterior stabilized total knee arthroplasties and appears to be related to femoral component design. The syndrome can usually be prevented by excising the residual synovial fold just proximal to the patella. Flexion gap instability can also cause a painful total knee arthroplasty but is less common in posterior stabilized implants. Femoral component malrotation can cause pain attributable to a flexion gap imbalance or patellar tracking problems. Polyethylene wear would be unlikely after just 1 year. Patellar clunk syndrome can usually be addressed successfully with arthroscopic synovectomy. Recurrence is uncommon. Physical therapy may help to strengthen the quadriceps following synovectomy but would not resolve the clunk syndrome symptoms. Femoral or tibial insert revision is not indicated if patellar clunk syndrome is the only problem resulting in a painful
total knee arthroplasty.
Question 12:
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should
Options:
- insert a standard humeral prosthesis with cerclage wires at the fracture site and autologous cancellous bone graft.
- insert a standard humeral component and apply a humeral orthosis postoperatively.
- cement a long-stemmed humeral component to bypass the fracture site and supplement with cerclage wires.
- remove all instrumentation, perform an open reduction and internal fixation of the fracture, and delay completion of replacement surgery until the fracture has healed.
- discontinue the procedure and return for completion of total shoulder replacement when the fracture has healed.
Correct Answer: cement a long-stemmed humeral component to bypass the fracture site and supplement with cerclage wires.
Explanation:
DISCUSSION: The risk of intraoperative fracture in osteopenic rheumatoid bone is significant. Fractures may occur with dislocation of the head and canal reaming, especially while extending and externally rotating the shoulder. If the fracture occurs at the distal tip of the prosthesis, the use of a long-stemmed prosthesis to bypass the fracture site and supplementation with wire cables has been reported with good results.
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 13:
A 50-year-old man reports the onset of back pain and incapacitating pain radiating down his left leg posterolaterally and into the first dorsal web space of his foot 1 day after doing some yard work. He denies any history of trauma. Examination reveals ipsilateral extensor hallucis longus weakness. MRI scans are shown in Figures 19a through 19c. What nerve root is affected?
Options:
- Left L4
- Right L4
- Left L5
- Right L5
- Left S1
Correct Answer: Left L5
Explanation:
DISCUSSION: The MRI scans clearly show an extruded L4-5 disk that is affecting the L5 root on the left side. In addition, the L5 root has a cutaneous distribution in the first dorsal web space. S1 affects the lateral foot, and L4 affects the medial calf.
REFERENCES: An HS: Principles and Techniques of Spine Surgery. Baltimore, MD, Williams and Wilkins, 1998, pp 98-100.
Hoppenfeld S: Orthopaedic Neurology. Philadelphia, PA, JB Lippincott, 1977, pp 7-49.
Question 14:
Clinical studies on the use of topical and intravenous (IV) forms of tranexamic acid (TXA) administration demonstrate which results?
Options:
- IV administration of TXA is substantially more efficacious in minimizing blood loss than topical administration.
- IV administration of TXA places high-risk patients such as those with coronary stents at an unacceptable risk for a cardiac event during the perioperative period.
- IV administration of TXA decreases intrasurgical blood loss but has not been shown to decrease postsurgical transfusion rates.
- Both IV and topical administration of TXA decrease intrasurgical blood loss and postsurgical transfusion rates.
Correct Answer: Both IV and topical administration of TXA decrease intrasurgical blood loss and postsurgical transfusion rates.
Explanation:
DISCUSSION
Numerous studies have demonstrated efficacy of both IV and topical administration of TXA for decreasing blood loss and transfusion rates. Several studies have shown no significant difference between TXA IV and topical administration in decreasing blood loss or lowering transfusion rates. Inconclusive evidence shows that IV administration of TXA places individuals at higher risk for a thromboembolic event. Both IV and topical TXA are equally effective in decreasing blood loss and minimizing transfusion rates.
Question 15:
You are staffing the prison clinic in a large public hospital when a 55-year-old African American male presents complaining of severe right hip pain. His pain has been ongoing for the past five years and limits his ambulation. He has never used medications for pain control or physical therapy. A radiograph is shown in figure
Options:
- When formulating his treatment plan, it is important to:
- Guarantee the success of total hip arthroplasty
- Recommend simultaneous bilateral total hip arthroplasty
- Understand the role of implicit bias as a determinant of health care delivery disparity
- Request the patient reveal the reason for his incarceration
- Suggest referral to a pain management clinic
Correct Answer: When formulating his treatment plan, it is important to:
Explanation:
The patient is an African American male prisoner with symptomatic right hip osteoarthritis. When formulating a treatment plan, it is important to understand the role of physician implicit bias in delivery of care and in creating disparities in
healthcare delivery.
Physician bias, prejudice, discrimination, and clinical uncertainty are all factors that contribute to health care disparities in the United States. Implicit and explicit attitudes are cognitive traits that influence physician delivery of care, and sometimes these attitudes do not perfectly correspond. It is important for a physician to understand that his implicit attitudes about a patient may unintentionally influence care despite his explicit attitudes. Physicians should be aware of their implicit biases in order to provide more effective decision-making and quality of care.
Stone et al. write about the issue of culturally competent delivery of care and the avoidance of unconscious bias in medical decision making. They argue that because unconscious stereotypes and prejudices can trigger biased medical decisions against specific groups, leading to the creation of differential diagnoses, disparities in treatment, and causing minorities to feel uncomfortable with seeking or complying with treatment plans. The authors suggest the integration of cultural competency training into medical education in order to help understand the perspective of the minority group patient.
Sabin et. al. compared the implicit and explicit biases of physicians with respect to race, gender, and age. They found that medical doctors showed an implicit bias of preferentially caring for White Americans relative to Black Americans, independent of the doctors’ self-report (explicit biases). Doctors'implicit biases exceeded their explicit biases in all race groups studied, except for African American physicians, who did not show an implicit bias toward patients.
Figure A demonstrates an AP pelvis x-ray with severe arthrosis of the right hip. The left hip demonstrates moderate disease.
Incorrect Answers:
Question 16:
A 38-year-old man is three quarters of the way through the Hawaiian Ironman events run in a temperature of 60 degrees F. He is sweating profusely and suddenly collapses. Prior to this he had been drinking large amounts of bottled water at every water stop. What is the most likely diagnosis? Review Topic
Options:
- Hypernatremia
- Hypothermia
- Hyponatremia
- Subendocardial myocardial infarction
- Ruptured berry aneurysm
Correct Answer: Hyponatremia
Explanation:
Hyponatremia is often seen in endurance athletes such as triathloners, ultramarathoners, and marathoners after prolonged exertion. It is commonly attributed to excess free water intake that fails to replete massive sodium losses that result from sweating as reported by O'Connor. Exercise-induced hyponatremia is generally asymptomatic, particularly in patients in whom the sodium is only mildy reduced. Up to 10% of ultradistance athletes have a sodium level of 135 mEq/L or less, but those who are symptomatic usually have a sodium level of 125 mEq/L as reported by Noakes and O'Connor. The best way to prevent hyponatremia is to maintain the proper volume and types of fluid intake to ensure fluid balance during exercise. Beverages containing carbohydrates in concentrations of 4% to 8% (ie, "sports drinks") are recommended for athletes participating in exercise lasting more than an hour (eg, marathon runners, etc.) To avert brainstem herniation and death, severe, acute hyponatremia requires rapid correction. Oral rehydration with salty solutions is safe and effective in patients with mild symptoms. Too rapid correction has been reported to cause central pontine myelinolysis; therefore, correction ought to be performed slowly. Hypernatremia, hypothermia, subendocardial myocardial infarction, or ruptured berry aneurysm are unlikely in this scenario.
Question 17:
While performing a total shoulder arthroplasty, excessive retraction is placed on the "strap muscles" (short head of biceps and coracobrachialis). Neurovascular examination would reveal weakness of which of the following? Review Topic
Options:
- Shoulder abduction
- Shoulder external rotation
- Shoulder internal rotation
- Elbow extension
- Forearm supination
Correct Answer: Forearm supination
Explanation:
The musculocutaneous nerve can be as close as 3 cm to the coracoid process; therefore, this relationship is important to keep in mind when performing surgery in
this area. Excessive traction on the musculocutaneous nerve could lead to a neurapraxia with resultant weakness of elbow flexion and forearm supinaton because of the loss of biceps function.
Question 18:
A 56-year-old woman undergoes an arthroscopic rotator cuff repair for a two-tendon retracted tear (supraspinatus and infraspinatus), requiring the use of four suture anchors placed in a double row technique. At her 1 month follow-up visit, what is the appropriate recommendation for her continued rehabilitation program? Review Topic
Options:
- Initiate isometric external rotation strengthening and continue passive range of motion.
- Initiate eccentric supraspinatus strengthening and continue passive range of motion.
- Initiate light resistance training to minimize atrophy and continue passive range of motion.
- Continue passive range of motion and initiate concentric deltoid strengthening.
- Continue passive range of motion with no active strengthening of the shoulder muscles.
Correct Answer: Continue passive range of motion with no active strengthening of the shoulder muscles.
Explanation:
Regardless of the technique of rotator cuff repair, the biology of tendon healing remains the same. Therefore, the repaired muscle tendon(s) must be protected from stress for a minimum of 6 weeks and more likely 8 weeks in a large two-tendon tear such as this patient had repaired. Therefore, at the 1 month follow-up visit, the patient should continue strict passive motion exercises and should perform no strengthening activities. Deltoid strengthening cannot be isolated from rotator cuff strengthening; therefore, deltoid strengthening is inappropriate as well. Because the infraspinatus is the primary shoulder external rotator, it should not be strengthened for 6 to 8 weeks. Supraspinatus strengthening at this time frame would likely ensure its disruption and result in failure of the surgery. Any resistance training at 1 month from surgery would likely result in tendon failure at the tendon-bone interface. The obligatory need to protect the muscles during healing will predictably result in atrophy but it is easier to strengthen healed muscles than it is to strengthen muscle/tendon units that have failed to heal.
Question 19:
EXT1
Options:
- This patient has multiple hereditary exostoses. Widening of the metaphysis is characteristic of multiple hereditary exostoses. Large sessile osteochondromas arise from the metaphysis and a large osteochondroma arises from the medial metaphysis with a characteristic cartilaginous cap. The computed tomography scan shows the widening and abnormal tubulation of the bone.
- No evidence of malignancy exists in this large osteochondroma. The cartilage cap is regular with no areas of bone destruction. One should also look for a soft tissue mass, which often shows areas of focal calcifications. No soft tissue masses are present in this patient.
- It is important to remember that this condition is autosomal dominant. The putative tumor suppressive gene mutation is EXT1, EXT2. The risk of low-grade chondrosarcoma occurring in this condition is approximately 10%.
Correct Answer: It is important to remember that this condition is autosomal dominant. The putative tumor suppressive gene mutation is EXT1, EXT2. The risk of low-grade chondrosarcoma occurring in this condition is approximately 10%.
Explanation:
slide 1 slide 2 slide 3
A patient presents with a hard leg mass and pain with activity. The anteroposterior and lateral radiographs are shown in Slide 1 and Slide 2. An axial computed tomography scan is shown in Slide 3. Which of the following would be the most appropriate treatment:
Question 20:
An 8-year-old boy with severe hemophilia A (factor VIII) and no inhibitor is averaging eight transfusions per month for bleeding into the right ankle. Examination shows synovial hypertrophy; range of motion consists of 0° of dorsiflexion and 20° of plantar flexion. The patient’s knees, elbows, and left ankle have no restriction of motion. Standing radiographs of the right ankle are shown in Figure 18. Management should consist of
Options:
- prophylactic transfusions three times per week.
- application of ankle-foot orthoses.
- ankle synovectomy.
- ankle arthrodesis performed with physeal protection.
- pantalar arthrodesis.
Correct Answer: ankle synovectomy.
Explanation:
DISCUSSION: The patient has bilateral hypertrophic synovitis that is causing repeated hemarthroses and progressive arthropathy. Ankle synovectomy in patients with hemophilia is effective in significantly reducing the rate of joint bleeding and in slowing the progression of the arthropathy; therefore, bilateral synovectomies is the treatment of choice. Range of motion can be effectively maintained after ankle synovectomy. Bracing and prophylactic transfusions would be ineffective at this time. Ankle arthrodesis should be reserved for patients with severe pain. Compared with patients who have juvenile rheumatoid arthritis, patients with hemophilia generally do not have involvement of the subtalar joint and rarely require a pantalar arthrodesis.
REFERENCES: Greene WB: Synovectomy of the ankle for hemophilic arthropathy. J Bone Joint Surg Am 1994;76:812-819.
Greene WB: Chronic inflammatory arthridities and diseases related to the hematopoietic system, in Drennan JC (ed): The Child’s Foot and Ankle, New York, NY, Raven Press, 1992, pp 461-482.
Question 21:
What is the most specific physical examination finding? Review Topic
Options:
- Positive impingement sign
- Positive apprehension
- Positive active compression
- Weakness of external rotation
- Weakness of abduction
Correct Answer: Weakness of external rotation
Explanation:
Overhead athletes are prone to a number of problems involving the shoulder. Pitchers and volleyball players are susceptible to posterior superior labral tears and internal impingement. These patients will have posterior superior shoulder pain, a positive relocation sign, and a positive active compression test. Occasionally, these posterior superior labral tears are associated with a spinoglenoid cyst as seen in the MRI scan. These cysts cause compression of the suprascapular nerve which manifests primarily as weakness of the infraspinatus, resulting in weakness of external rotation.
Question 22:
A 29-year-old woman is seen in the emergency department with a 24-hour history of severe back and leg pain precipitated by weight-lifting. The patient reports bilateral leg pain and is unable to urinate. She has dense anesthesia in the perineal region on examination. A MRI scan is shown in Figure 38. The patient is taken to surgery urgently. What is her prognosis for recovery? Review Topic
Options:
- Improvement in her pain and sensory symptoms following surgery but may have residual bladder dysfunction
- Decreased pain following surgery; sensory deficits and bladder function are not likely to improve
- No change in her symptoms following surgery
- Complete resolution of pain and will have normal sensation and bladder function following surgery
- Improvement in her pain and complete return of bladder function following surgery; sensation may not return
Correct Answer: Improvement in her pain and sensory symptoms following surgery but may have residual bladder dysfunction
Explanation:
The patient with cauda equina syndrome should be taken to surgery urgently to provide the best chance of symptom resolution. However, many studies indicate that patients with cauda equina syndrome do not return to a completely normal status even following urgent surgery. Whereas pain is typically relieved after surgery, other deficits, especially bladder and sexual dysfunction, may persist. Particularly in light of the patient's severe saddle anesthesia, she may have a poor prognosis for recovery of normal bladder function.
Question 23:
A radiograph of a 12-year-old boy who has had an insidious onset of pain in the right hip for the past 6 weeks shows diffuse narrowing of the joint space. Examination reveals that he is afrebile, and the range of motion of the hip is less than 50% of normal in all planes. Laboratory studies show an erythrocyte sedimentation rate of 21 mm/hr and a WBC of 11,000/mm3. What is the most likely diagnosis?
Options:
- Sickle cell crisis
- Idiopathic chondrolysis
- Hemophilic arthropathy
- Osteoid osteoma of the femoral neck
- Legg-Calve-Perthes disease
Correct Answer: Idiopathic chondrolysis
Explanation:
First, sickle cell crisis is a localized area of bone marrow infarction with excruciating pain. Swelling of the extremity and limitation of motion are usually mild. Temperature elevation is usually mild but is >39 degrees celsius in 29% of patients. It is also limited to 3-5 days in duration.
This patient has no history of hemophilia given. Hemophilic arthropathy begins with a hemarthrosis.
In osteoid osteoma the pain is typically unrelenting, sharp, boring, worse at night, and relieved with aspirin. It is not associated with joint space narrowing.
The most common age for Legg-Calve-Perthes disease is 4-8 years. It causes AVN of the femoral head and widening of the medial joint space is an early radiographic finding.
In Bleck’s report on Idiopathic Chondrolysis JBJS 1983 nine cases were seen at the reporting institution between 1973 and 1978. The average age was 11.5 years. All the patients were otherwise healthy and had no history of systemic illness of previous trauma. All the patients reported the insidious onset of pain in the anterior part of the hip. All had a decreased passive ROM. Radiographic examination showed regional osteoporosis, premature closure of the femoral capital physis, narrowing of the joint space, and lateral overgrowth of the femoral head on the neck. All laboratory examinations were negative for evidence of infection or rheumatoid arthritis. Treatment consists of administration of aspirin, active non-loading exercise of the hip, and protected weight-bearing with crutches.
Question 24:
A 12-year-old girl has a 4-cm limb-length discrepancy following a fracture of the left distal femur 2 years ago. Examination reveals 18 degrees of genu valgum on the involved side, with 7 degrees of genu valgum on the opposite side. Radiographs show that the left distal femoral growth plate is now closed; however, the tibial growth plate is still open. Her bone age matches her chronologic age. Management should consist of
Options:
- closed right femoral shortening.
- left femoral lengthening.
- left tibial lengthening.
- a left 3-cm shoe lift.
- epiphyseodesis of the right distal femur and proximal tibia.
Correct Answer: left femoral lengthening.
Explanation:
DISCUSSION: The patient has a projected limb-length discrepancy of 7 cm. This includes the 4 cm she already has, plus 3 cm expected growth of the uninvolved distal femur during the 3 years of growth she has remaining. She also has moderate limb deformity. Femoral lengthening is considered the treatment of choice because it can address both the limb-length discrepancy and the deformity. Epiphyseodesis will not result in limb-length equality at maturity, with only approximately 1.8 cm of equalization expected from this procedure. Use of closed femoral shortening of 7 cm runs the risk of weakening the quadriceps on the normal side and will leave the patient with a remaining residual valgus deformity. Tibial lengthening will leave the knees at different levels. A shoe lift can be prescribed as a temporary measure but is not a good
long-term solution.
REFERENCES: Westh RN, Menelaus MB: A simple calculation for the timing of epiphyseal arrest: A further report. J Bone Joint Surg Br 1981;63:117-119.
Sasso RC, Urquhart BA, Cain TE: Closed femoral shortening. J Pediatr Orthop 1993;13:51-56.
Nordsletten L, Holm I, Steen H, Bjerkreim I: Muscle function after femoral shortening osteotomies at the subtrochanteric and mid-diaphyseal level: A follow-up study. Arch Orthop Trauma Surg 1994;114:37-39.
Question 25:
During treatment of rupture of the subscapularis tendon with associated biceps instability, treatment of the biceps tendon should include which of the following? Review Topic
Options:
- Tenosynovectomy
- Recentering
- Deepening of the bicipital groove
- Tenodesis or tenotomy
- Lysis of sheath adhesion
Correct Answer: Tenodesis or tenotomy
Explanation:
With subscapularis tendon ruptures that have biceps tendon pathology, treatment with tenodesis or tenotomy has improved clinical results. Subluxation or dislocation of the biceps tendon is common with subscapularis rupture. Dislocation of the biceps can occur either beneath the tendon, within the tendon, or extra-articularly. In all cases,
the restraints to medial translations of the biceps have been disrupted. Attempts at recentering the biceps have not been successful, and clinical results appear to be improved when tenodesis or tenotomy is employed in the treatment of the unstable biceps associated with subscapularis tears.
Question 26:
-A 16-year-old girl was seen after a motor vehicle collision. Imaging studies including plain radiographs,MRI scans, and CT scans confirm bilateral jumped facets at C5-6 without disk herniation. She is alert,oriented, and neurologically intact. What is the most appropriate next step?
Options:
- Awake closed reduction
- Application of a halo orthosis
- Placement of a cervical collar
- Open reduction under anesthesia
- Closed reduction under anesthesia
Correct Answer: Awake closed reduction
Question 27:
Which of the following complications is uniquely associated with an anterior approach to the lumbosacral junction?
Options:
- Nerve root injury
- Erectile dysfunction
- Dural tear
- Pulmonary embolism
- Retrograde ejaculation
Correct Answer: Retrograde ejaculation
Explanation:
DISCUSSION: Retrograde ejaculation is a sequela of injury to the superior hypogastric plexus. The structure needs protection, especially during anterior exposure of the lumbosacral junction. The use of monopolar electrocautery should be avoided in this region. The ideal exposure starts with blunt dissection just to the medial aspect of the left common iliac vein, sweeping the prevertebral tissues toward the patient’s right side. Although erectile dysfunction can be seen after spinal surgery, it is not typically related to the surgical exposure because erectile function is regulated by parasympathetic fibers derived from the second, third, and fourth sacral segments that are deep in the pelvis and are not at risk with the anterior approach. The other choices are complications of spinal surgery but are not uniquely associated with an anterior L5-S1 exposure.
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Watkins RG (ed): Surgical Approaches to the Spine, ed 1. New York, NY, Springer-Verlag, 1983, p 107.
An HS, Riley LH III: An Atlas of Surgery of the Spine. New York, NY, Lippincott Raven, 1998, p 263.
Question 28:
Which modality has the broadest application for the reduction of postsurgical transfusion?
Options:
- Regional anesthesia
- Tranexamic acid (TXA) administration
- Reduced transfusion trigger
- Hypotensive anesthesia
Correct Answer: Tranexamic acid (TXA) administration
Explanation:
DISCUSSION:
TXA is easy to administer, inexpensive, and safe for virtually all patients. Multiple studies have demonstrated transfusion rates lower than 3% for total knee arthroplasty and lower than 10% for total hip arthroplasty. Regional and hypotensive anesthesia effectively reduce transfusion; however, they cannot be used in as wide a range of patients as can TXA. A reduced transfusion trigger must be considered along with patient symptoms when determining the need for transfusion.
Question 29:
A 52-year-old woman reports the sudden onset of intense pain in the right shoulder. She denies any history of injury or previous shoulder problems. At a 2-week follow-up examination, she notes that the pain has decreased, but she now has severe weakness of the external rotators and abductors. Her cervical spine and remaining shoulder examination are otherwise unremarkable. Radiographs of the shoulder and neck are normal. What is the most likely diagnosis?
Options:
- Calcific tendinitis
- Rotator cuff tendinosis
- Bursitis
- Brachial neuritis
- Glenohumeral arthritis
Correct Answer: Brachial neuritis
Explanation:
DISCUSSION: Patients with brachial neuritis or Parsonage-Turner syndrome usually report the sudden onset of intense pain that subsides in 1 to 2 weeks, followed by weakness for a period of up to 1 year in the muscle that is supplied by the involved nerve. Calcific tendinitis usually can be diagnosed radiographically, with calcium deposits seen in the rotator cuff. Bursitis and rotator cuff tendinosis usually are seen after an increase in activity, and both decrease with rest and medication. Glenohumeral arthritis is a slow, progressive problem that results in a loss of range of motion.
REFERENCES: Misamore GW, Lehman DE: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg Am 1996;78:1405-1408.
Dillin L, Hoaglund FT, Scheck M: Brachial neuritis. J Bone Joint Surg Am 1985;67:878-880.
Question 30:
- Which of the following events is most likely to occur following a complete transection of a peripheral nerve?
Options:
- The cell body nucleus migrates centrally
- Schwann cells distal to the transection die
- Axoplasm in the proximal stump drains out
- Myelin distal to the transection is phagocytized
- Cell body protein synthesis decreases for the first 10 to 14 days
Correct Answer: Myelin distal to the transection is phagocytized
Explanation:
Reference-Within a few hours of injury to a nerve fiber the cell body swells and Nissl granules disappear. The axon distal to the site of injury rapidly undergoes Wallerian degeneration with the loss of the axon and breakup of the surrounding myelin.
Question 31:
Which of the following prophylactic regimens for the prevention of deep venous thrombosis after knee arthroplasty has received a grade 1A recommendation in favor of its use from the American College of Chest Physicians (ACCP) in the 2004 guidelines?
Options:
- Warfarin with a targeted international normalized ratio (INR) of 2.0 to 3.0 for 10 to 14 days
- Low-molecular-weight heparin used for at least 3 days
- Pneumatic compression sleeves used while the patient is in the hospital
- Fondaparinux used for 5 to 7 days
- Aspirin for 4 weeks
Correct Answer: Warfarin with a targeted international normalized ratio (INR) of 2.0 to 3.0 for 10 to 14 days
Explanation:
DISCUSSION: In the 2004 ACCP guidelines, there were three prophylactic regimens that received a grade 1A favorable recommendation. These included low-molecular-weight heparin, warfarin, or fondaparinux, as long as they are used for at least 10 days. If warfarin is used, the target INR should be 2.0 to 3.0, according to the guidelines. Pneumatic compression sleeves have gained popularity in the orthopaedic community but have not received a grade 1A rating from the ACCP at this time. Use of aspirin by itself is discouraged by the ACCP.
REFERENCE: Geerts WH, Pineo GF, Heit JA, et al: Prevention of venous thromboembolism: The seventh ACCP Conference on antithrombotic and thrombolytic therapy. Chest 2004;126:338S-400S.
Question 32:
In the anterior forearm approach to the distal radius (Henry approach), the radial artery is located between what two structures?
Options:
- Flexor carpi radialis tendon and flexor digitorum superficialis muscle
- Flexor carpi radialis and brachioradialis tendons
- Flexor carpi radialis and palmaris longus tendons
- Brachioradialis and flexor pollicis longus tendons
- Brachioradialis tendon and flexor digitorum superficialis muscle
Correct Answer: Flexor carpi radialis and brachioradialis tendons
Explanation:
DISCUSSION: The standard approach to the volar aspect of the distal radius is the Henry approach. Following incision of the skin and subcutaneous tissues, the forearm fascia is incised. The radial artery and venae comitantes lie in the interval between the tendons of the flexor carpi radialis muscle and the brachioradialis muscle. This interval is developed, and the radial artery and veins are retracted in a radial direction.
REFERENCES: Hoppenfeld S, deBoer P: Surgical Exposures in Orthopaedics, ed 2. Philadelphia, PA, Lippincott-Raven, 1994, pp 118-131.
Henry A: Extensile Exposure, ed 3. Edinburgh, UK, Churchill Livingstone, 1995, pp 100-107.
Question 33:
A 72-year-old man who underwent total shoulder arthroplasty 2 years ago slipped on ice and fell on his shoulder 3 weeks ago. Immediately after falling he was unable to elevate his arm. Motor examination reveals deltoid 5-/5, subscapularis 5-/5, external rotation 4-/5, and supraspinatus 2/5. Radiographs are shown in Figures 8a and 8b. What is the most likely diagnosis? Review Topic
Options:
- Anterior shoulder dislocation
- Humeral component loosening
- Glenoid component loosening
- Glenoid component catastrophic fracture
- Rotator cuff tear
Correct Answer: Rotator cuff tear
Explanation:
The patient has a traumatic rotator cuff tear. The history of the fall, the weakness on examination, and normal radiographic findings make a traumatic rotator cuff tear the most likely diagnosis. An MRI scan can be obtained to further evaluate the integrity of the rotator cuff. The axillary radiograph shows a reduced, nondislocated total shoulder arthroplasty. His radiographs show a well-seated humeral stem and no signs of loosening. The glenoid is a cemented all-polyethylene component with no evidence of radiolucent lines surrounding the cemented pegs. The polyethylene glenoid component is radiolucent; however, the space between the metallic humeral head and the glenoid bone is the thickness of the polyethylene glenoid component. If the humeral head were directly against the glenoid bone, then catastrophic fracture of the glenoid would be the working diagnosis.
Question 34:
In a patient who has had low back pain for less than 2 weeks, which of the following findings is an indication for continued observation and symptomatic treatment rather than more aggressive evaluation and/or treatment?
Options:
- Inability to control urinary function
- Inability to participate in athletics
- Decreased sphincter tone and function
- History of previous malignancy
- History of a fall preceding the pain
Correct Answer: Inability to participate in athletics
Explanation:
DISCUSSION: An inability to participate in athletics generally is considered an indication for continued symptomatic treatment only. All of the other answers suggest the possibility of more significant pathology that may require more urgent treatment.
REFERENCES: Frymoyer JW: Back pain and sciatica. N Engl J Med 1988;318:291-300.
McCullough JA, Transfeldt EE: Macnab’s Backache, ed 3. Baltimore, MD, Williams and Wilkins, 1997, pp 240-357.
Question 35:
A surgeon prepares a medial gastrocnemius rotational flap to cover a medial proximal tibia defect at the time of revision knee replacement surgery. To optimize coverage, the surgeon must optimally mobilize which artery?
Options:
- Profunda femoris B. Middle genicular C. Medial sural
- Inferior medial genicular
Correct Answer: Profunda femoris B. Middle genicular C. Medial sural
Explanation:
DISCUSSION:
The medial sural arteries vascularize the gastrocnemius, plantaris, and soleus muscles proximally. These arteries arise from the popliteal artery. If this artery is not adequately mobilized, a gastrocnemius soleus flap can be devascularized.
Question 36:
Following an acute dislocation of the patella, the risk of a recurrent dislocation is greater if the patient has which of the following findings?
Options:
- Bipartite patella
- Age greater than 15 years at the time of the initial dislocation
- Persistent atrophy of the vastus lateralis
- Low-lying position of the patella (patella baja)
- Passive lateral hypermobility of the unaffected knee
Correct Answer: Passive lateral hypermobility of the unaffected knee
Explanation:
DISCUSSION: Recurrent dislocations may follow an earlier dislocation. One study found that in patients who had a patellar dislocation between the ages of 11 to 14 years, 60% had a recurrent dislocation. The incidence of recurrent dislocation dropped to 33% in patients who had a patellar dislocation between the ages of 15 to 18 years. The authors also found that the incidence of recurrence was greater in patients who demonstrated a predisposition to dislocation as determined by evaluation of the unaffected knee. Predisposing signs included passive lateral hypermobility of the patella, a dysplastic distal third of the vastus medialis obliquis muscle, and a high and/or lateral position of the patella. A second study found that the risk of redislocation was considerably higher in patients who were in their teens at the first episode of dislocation compared to older patients. There are no studies linking either a patella baja or a bipartite patella to an increased risk of redislocation.
REFERENCES: Cash JD, Hughston JC: Treatment of acute patellar dislocation. Am J Sports Med 1988;16:244-249.
Larsen E, Lauridsen F: Conservative treatment of patellar dislocations: Influence of evident factors on the tendency to redislocation and the theraputic result. Clin Orthop
1982;171:131-136.
Question 37:
A 45-year-old man who smokes reports the rapid onset of color changes and coolness in the fingers. Examination shows an abnormal Allen test. Plain radiographs of the hand and wrist are normal. Which of the following studies will best aid in diagnosis?
Options:
- Contrast CT of the hand and wrist
- MRI of the hand and wrist
- Contrast angiography of the involved upper extremity
- Digital subtraction angiography
- Single-shot fluoroscopic angiography
Correct Answer: Contrast angiography of the involved upper extremity
Explanation:
DISCUSSION: The patient has symptoms typical of Raynaud’s phenomenon secondary to underlying vascular disease. The next most appropriate step in the management of this patient should be to perform contrast angiography on the involved upper extremity to look for proximal or distal arterial lesions or insufficiencies. MRI and contrast CT are not as specific as angiography for the identification of vascular lesions of the upper extremity. Although patients with primary Raynaud’s vasospastic disease can have normal angiographic findings, they typically are younger than age 40 years, are female, and have normal results on an Allen test.
REFERENCES: Green DP, Hotchkiss RN, Pederson WC (eds): Operative Hand Surgery, ed 4. New York, NY, Churchill Livingstone, 1999, pp 2288-2290.
Manske PR (ed): Hand Surgery Update. Rosemont, IL, American Society for Surgery of the Hand, 1994, pp 197-205.
Question 38:
Which of the following statements best characterizes polymethylmethacrylate (PMMA) when it is used to secure joint components in bone and to distribute the forces evenly across the bone-implant interface?
Options:
- PMMA is stronger in tension than compression.
- Porosity reduction increases the fatigue strength of PMMA.
- Hypotension that occasionally results after PMMA is placed in the femoral canal is independent of a patient’s intraoperative blood volume.
- Inclusion of antibiotics does not alter the strength of PMMA.
- PMMA bonds chemically to bone and the implant surface.
Correct Answer: Porosity reduction increases the fatigue strength of PMMA.
Explanation:
DISCUSSION: PMMA has no adhesive properties and can be more accurately described as grout than glue. It does not chemically bond to bone or implants; however, mechanical bonding is accomplished with porous or coated components and with cancellous bone. PMMA is approximately three times stronger in compression than in tension. Peak blood levels of monomer are usually seen approximately 3 minutes after the cement is placed. The monomer is cleared by the lungs. Associated hypotension is more closely related to diminished blood volume than to circulating monomer levels. High porosity decreases the tensile and fatigue properties of cement. Manually mixed cement may have porosity as high as 27%. Porosity may be reduced to less than 1% through vacuum mixing or centrifugation of the cement. When adding antibiotics to cement, the compressive and tensile forces are not appreciably decreased, but the overall fatigue strength may be reduced.
REFERENCES: Canale ST (ed): Campbell’s Operative Orthopaedics, ed 9. St Louis, MO, Mosby, 1998, pp 221-224.
Callaghan JJ, Dennis DA, Paprosky WG, Rosenberg AG (eds): Orthopaedic Knowledge Update: Hip and Knee Reconstruction. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1995, pp 27-33.
Question 39:
Of the following, what is the most reliable method of assessing spinal fusion? Review Topic
Options:
- Radiographs
- MRI
- Flexion/extension radiographs
- CT
- CT myelography
Correct Answer: CT
Explanation:
Despite the ease of attainment, radiographs only accurately diagnose failed arthrodesis in 60% to 80% of uninstrumented cases and these numbers are even lower in cases with posterior instrumentation. The role of dynamic radiographs remains unclear because of the paucity of normative data values after lumbar spine fusion. CT scans provide excellent bony detail and their images are not affected by metal components as in MRI. Post-myelogram CT is useful for identifying neurologic compression.
Question 40:
A 16-year-old girl has had pain in the left groin for the past 4 months. She notes that the pain is worse at night; however, she denies any history of trauma and has no constitutional symptoms. There is no history of steroid or alcohol use. Examination reveals pain in the left groin with rotation of the hip. There is no associated soft-tissue mass. A radiograph and MRI scan are shown in Figures 32a and 32b, and biopsy specimens are shown in Figures 32c and 32d. What is the most likely diagnosis?
Options:
- Clear cell chondrosarcoma
- Chondroblastoma
- Giant cell tumor
- Aneurysmal bone cyst
- Osteonecrosis of the femoral head
Correct Answer: Chondroblastoma
Explanation:
DISCUSSION: Based on the epiphyseal location and sharp, well-defined borders, the radiograph suggests chondroblastoma. Histologically, multinucleated giant cells are scattered among mononuclear cells. The nuclei are homogenous and contain a characteristic longitudinal groove. Although not seen here, “chicken-wire calcification” with a bland giant cell-rich matrix is also typical for chondroblastoma. Clear cell chondrosarcoma occurs in epiphyseal locations but has a more aggressive histologic pattern and occurs in an older age group. Giant cell tumors occur in the epiphysis but have a more uniform giant cell population histologically. Aneurysmal bone cyst often results in bone remodeling and has a different pathologic appearance. Osteonecrosis has a typical histologic pattern of empty lacunae and necrotic bone.
REFERENCES: Springfield DS, Capanna R, Gherlinzoni F, et al: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Simon M, Springfield D, et al: Chrondroblastoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 190.
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990,
pp 62-67.
Question 41:
After excising a mass from the thigh that was thought to be a lipoma, the pathology reveals that the mass is a high-grade sarcoma. Subsequent treatment should include
Options:
- repeat excision of the tumor bed.
- chemotherapy only.
- radiation therapy only.
- chemotherapy and radiation therapy only.
- administration of bisphosphonates.
Correct Answer: repeat excision of the tumor bed.
Explanation:
DISCUSSION: Following excision of a suspected benign soft-tissue tumor that proves to be malignant, repeat excision of the tumor bed is recommended. The initial surgical margins are inadequate after an intralesional or marginal excision, necessitating additional surgery for more definitive local control. While radiation therapy and/or chemotherapy may help to reduce the risk of local recurrence in patients with microscopic residual disease, local control is improved following repeat excision. Radiation therapy alone is inadequate to address poor surgical margins, and would likely be given postoperatively. Bisphosphonates have no current role in the treatment of soft-tissue sarcoma.
REFERENCES: Noria S, Davis A, Kandel R, et al: Residual disease following unplanned excision of soft-tissue sarcoma of an extremity. J Bone Joint Surg Am 1996;78:650-655.
Bell RS, O’Sullivan B, Liu FF, et al: The surgical margin in soft-tissue sarcoma. J Bone Joint Surg Am 1989;71:370-375.
Question 42:
Which of the following complications is more likely with an inside-out repair technique compared to an all-inside techniques for a medial meniscus tear? Review Topic
Options:
- Failure
- Intra-articular synovitis
- Peroneal nerve injury
- Saphenous nerve injury
- Arthrofibrosis
Correct Answer: Saphenous nerve injury
Explanation:
All of the answers are possible complications of meniscal repair. There are large volumes of literature evaluating the results of meniscal repair, both for the all-inside technique, as well as the inside-out technique. Failure rates are similar. Intra-articular synovitis occurs with absorbable sutures and absorbable implants. Peroneal nerve injuries are more common with the lateral-sided repairs. Saphenous nerve injuries are more common with medial-sided tears. Because of the incision required and the technique of tying over soft tissue, the risk of a saphenous nerve injury is greater with an inside-out technique than with an all-inside technique.
Question 43:
An 18-year-old high school football player sustains a left posterior hip dislocation that is reduced in the emergency department under IV sedation. Postreduction radiographs reveal a concentric reduction with no evidence of fracture or loose bodies within the joint. What is the most common complication of hip dislocations?
Options:
- Femoral nerve palsy
- Sciatic nerve palsy
- Recurrent hip dislocation
- Osteonecrosis of the femoral head
- Immediate chondrolysis of the hip joint
Correct Answer: Osteonecrosis of the femoral head
Explanation:
DISCUSSION: Traumatic dislocation of the hip in sports injuries is uncommon, and 85% to 92% occur in a posterior direction. In dislocations without fractures, osteonecrosis is the most common complication occurring in 10% to 20% of patients. MRI should be performed at 3 months postreduction to rule out osteonecrosis. Nerve injuries are rare in this setting, and recurrent dislocations are unusual without acetabular fractures. Chondrolysis has been reported as a rare occurrence.
REFERENCES: Anderson K, Strickland S, Warren R: Hip and groin injures in athletes. Am J Sports Med 2001;29:521-533.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 407-416.
Question 44:
A 30-year-old man has pain in the left arm after a motor vehicle accident. His neurovascular examination is intact, and radiographs are shown in Figures 25a and 25b. What is the best course of management?
Options:
- Closed reduction and cast immobilization for 4 weeks, followed by therapy directed at regaining motion
- Open reduction and internal fixation of the olecranon fracture, functional bracing of the humeral fracture, and therapy directed at regaining motion initiated at 2 weeks after surgery
- Open reduction and internal fixation of the olecranon and humeral fractures, followed by therapy directed at regaining motion
- Open reduction and internal fixation of the olecranon and humeral fractures, and splint immobilization for 4 weeks followed by therapy directed at regaining motion
- Open reduction and internal fixation of the olecranon fracture, functional bracing of the humeral fracture, and therapy directed at regaining motion initiated at 4 weeks after surgery
Correct Answer: Open reduction and internal fixation of the olecranon and humeral fractures, followed by therapy directed at regaining motion
Explanation:
DISCUSSION: The floating elbow is best managed with early open reduction and internal fixation of the humeral and forearm fractures, followed by early range of motion. These fractures predispose the elbow to stiffness, and early range of motion is recommended.
REFERENCES: Solomon HB, Zadnik M, Eglseder WA: A review of outcomes in 18 patients with floating elbow. J Orthop Trauma 2003;17:563-570.
Yokoyama K, Itoman M, Kobayashi A, et al: Functional outcomes of “floating elbow” injuries in adult patients. J Orthop Trauma 1998;12:284-290.
Question 45:
Figure 40 shows the AP radiograph of a 55-year-old man who reports left knee pain. Which of the following conditions is least likely to produce this radiographic presentation?
Options:
- Hemochromatosis
- Alkaptonuria
- Wilson’s disease
- Septic arthritis
- Calcium pyrophosphate dihydrate crystal deposition
Correct Answer: Septic arthritis
Explanation:
DISCUSSION: The radiograph reveals densities within the articular cartilage of the knee commonly referred to as chondrocalcinosis. The term chondrocalcinosis refers to the presence of calcium-containing crystals detected as radiodensities in cartilage. Calcium-containing crystals other than calcium pyrophosphate dihydrate may also deposit in articular cartilage and menisci, producing both radiographically detectable densities in cartilage and joint inflammation or degeneration. Hemochromatosis, alkaptonuria (ochronosis), and Wilson’s disease are characterized by cellular deposition of iron, calcium, and copper ions, respectively, into various tissues including articular cartilage and can give this appearance. Septic arthritis does not usually cause chondrocalcinosis.
REFERENCES: Klippel JH (ed): Primer on the Rheumatic Diseases, ed 11. Atlanta, GA, Arthritis Foundation, 1997, pp 226-229 and 328-331.
Resnick D, Wayama G: Diagnosis of Bone and Joint Disorders, ed 2. Philadelphia, PA, WB Saunders, 1988, pp 1675, 1779.
Question 46:
Massive cortical structural allografts are commonly used in oncologic and arthroplasty surgery. What percent of cortical structural allografts fracture due to insufficiency?
Options:
- 1 0% to 5%
- 2 15% to 30%
- 3 50% to 60%
- 4 70% to 80%
- 80% to 100%
Correct Answer: 2 15% to 30%
Explanation:
Allograft is available in particulate and structural forms. Particulate allograft has a higher rate of incorporation than structural but adds little structural support. Cortical allograft incorporation occurs slowly and the bulk of the graft fails to remodel and remains devascularized. Stress fractures eventually occur in approximately 25% of structural grafts used in tumor surgery.
Question 47:
A 12-year-old girl has back pain after falling 20 feet and landing in the sitting position. She has no fractures or other injuries, and her neurologic examination is normal. A lateral radiograph, transverse CT scan, and reformatted sagittal CT scan are shown in Figures 25a through 25c. Which of the following methods is associated with the best long-term outcome? Review Topic
Options:
- Hyperextension casting of the thoracolumbar spine for 6 weeks
- In situ posterior fusion with instrumentation
- Posterior fusion with instrumentation, with sagittal plane correction
- Posterior decompression, followed by posterior fusion with instrumentation, with sagittal plane correction
- Anterior decompression and partial corpectomy, with anterior instrumentation
Correct Answer: Posterior fusion with instrumentation, with sagittal plane correction
Explanation:
The patient has a displaced burst fracture. Fusion with instrumentation has shown better results than casting alone. Posterior fusion with instrumentation, with sagittal plane correction, yields the best results. Decompression occurs indirectly with correction of the kyphosis. Anterior decompression is unnecessary.
Question 48:
What is the most common mode of failure following unconstrained total elbow arthroplasty? Review Topic
Options:
- Polyethylene wear
- Bushing wear
- Instability
- Component fracture
- Loosening of the humeral component
Correct Answer: Instability
Explanation:
Elbow instability after placement of an unconstrained implant is most often the result of ligamentous insufficiency that can occur late after the index procedure. Instability can also occur from component malpositioning that creates undue stress to the collateral ligaments during the life of the prosthesis. Instability leads to revision surgery in many patients. Polyethylene wear and bushing wear are more common in linked and semiconstrained elbow arthroplasties. Loosening of humeral components may occur with aseptic or septic disease. Component fracture is uncommon.
Question 49:
What do the T2-weighted, fat-saturated MRI scans shown in Figures 76a through 76d reveal? Review Topic
Options:
- Posterior cruciate ligament (PCL) tear, isolated
- PCL tear and medial meniscus tear
- Anterior cruciate ligament (ACL) tear, isolated
- ACL tear and medial meniscus tear
Correct Answer: ACL tear and medial meniscus tear
Explanation:
The MRI scans show that edema is noted on the femoral insertion of the ACL consistent with a high-grade or complete ACL tear. The ACL is not visualized on the sagittal view, although the torn meniscus can be seen in the notch. On the coronal image, there is an empty lateral wall sign indicating proximal disruption of the ACL. The medial meniscus images show a disruption of normal meniscus morphology consistent with a bucket handle medial meniscus tear. Note the appearance on the sagittal MRI scan of what appears to be a second soft-tissue density in line with the PCL. This "double PCL" sign is highly indicative of a displaced medial meniscus tear rather than a displaced lateral meniscus tear.
Question 50:
Figures 51a and 51b show the AP and lateral radiographs of the elbow of a 26-year-old man who fell. Closed reduction was performed in the emergency department, and management consisted of immobilization for 3 weeks prior to the initiation of motion. At 12 weeks after injury, he reports continued feelings of instability and catching in his elbow when using his arms to rise from a chair. Which of the following procedures needs to be performed, at a minimum, to reestablish stability of the elbow? Review Topic
Options:
- Medial collateral ligament repair
- Medial collateral ligament reconstruction
- Hinged external fixation
- Lateral collateral ligament repair
- Lateral collateral ligament reconstruction
Correct Answer: Lateral collateral ligament reconstruction
Explanation:
The patient has chronic posterolateral instability of the elbow following dislocation. The lateral collateral ligament complex is responsible for maintaining stability of the elbow. Because of the chronicity of the injury, the ligamentous tissues are frequently attenuated and not amenable to simple repair; while the native ligament can be imbricated, reconstruction with allograft or autograft is recommended. Medial collateral ligament reconstruction or hinged external fixation is needed only if restoration of the lateral ligamentous complex does not restore elbow stability; however, these procedures are rarely required. Lateral elbow pain when rising from a chair is equivalent to a positive pivot shift test.
Question 51:
The tibiofibular overlap used to diagnose syndesmotic diastasis on an AP view is most commonly measured between the
Options:
- lateral border of the fibula and the medial border of the posterior tibial tubercle.
- medial border of the fibula and the lateral border of the posterior tibial tubercle.
- medial border of the fibula and the medial border of the deepest point of the incisura fibularis.
- medial border of the fibula and the lateral border of the anterior tibial tubercle.
- medial border of the fibula and the lateral border of the deepest point of the incisura fibularis.
Correct Answer: medial border of the fibula and the lateral border of the anterior tibial tubercle.
Explanation:
DISCUSSION: The tibiofibular overlap is measured between the medial border of the fibula and the lateral border of the anterior tibial tubercle. Plain radiographic assessment of the distal tibiofibular syndesmosis requires AP and mortise views. The following criteria have been used as the normal limits in adults: a talocrural angle of + or - 83 degrees with up to 5 degrees of normal difference between both sides, a medial clear space of less than 4 mm, a talar tilt of less than 2 mm, a tibiofibular clear space of less than 5 mm, a tibiofibular overlap of greater than or equal to 0 mm, and a talar subluxation that is a subjective assessment of congruity of the tibial articular surface and the talar dome; any incongruity is abnormal. It has been recommended to obtain the first three measurements on the mortise view and the other three on the AP view.
REFERENCES: Wuest TK: Injuries to the distal lower extremity syndesmosis. J Am Acad Orthop Surg 1997;5:172-181.
Stiehl JB: Ankle fractures with diastasis. Instr Course Lect 1990;39:95-103.
Question 52:
- Which of the following radiographic views best shows the size and displacement of a posterior wall fracture of the acetabulum?
Options:
- Inlet view of the pelvis
- Outlet view of the pelvis
- AP view of the hip
- Ilial oblique view (external oblique) of the hip
- Obturator oblique
Correct Answer: Obturator oblique
Explanation:
This view best reveals the posterior acetabular wall and the anterior column of the pelvis. This view is best taken by elevating the affected hip 45 degrees to the horizontal by means of a wedge and directing the beam through the hip joint with a 15 degree upward tilt. The inlet view best delineates posterior displacement of the hemipelvis. The outlet view best views the sacrum, the sacroiliac joints, and the sacral foramina, caudad and cephalad displacement as well. The standard AP radiograph is used in the initial trauma series as a screening tool. Ilial oblique views best view the anterior wall of the acetabulum and the posterior column of the pelvis.
Question 53:
Intramembranous ossification during fracture repair is characterized by absence of which of the following elements?
Options:
- Alkaline phosphatase
- Osteonectin
- Osteopontin
- Collagen type I expression
- Collagen type II expression
Correct Answer: Collagen type II expression
Explanation:
DISCUSSION: Intramembranous ossification occurs through the direct formation of bone without the formation of a cartilaginous intermediate. Clinically, both intramembranous and endochondral ossification occur simultaneously during fracture healing; however, the latter is characterized by the differentiation and maturation of chondrocytes, vascular invasion of a hypertrophic cartilage matrix, and bone formation. Collagens type II and X are cartilage specific and would be characteristic of endochondral ossification, not intramembranous ossification.
REFERENCES: Li J, Sandell LJ: Transcriptional regulation of cartilage-specific genes, in Rosier RN, Evans C (eds): Molecular Biology in Orthoapedics, Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, pp 21-24.
Buckwalter JA, Einhorn TA, Bolander ME: Healing of the musculoskeletal tissues, in Rockwood CA Jr, Green DP, Bucholz RW, et al (eds): Rockwood and Green’s Fractures in Adults, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, pp 261-276.
Question 54:
What spinal nerves in the cauda equina are primarily responsible for innervation of the bladder?
Options:
- L1, L2, and L3
- L4 and L5
- L5 and S1
- S2, S3, and S4
- Filum terminale
Correct Answer: S2, S3, and S4
Explanation:
DISCUSSION: The spinal nerves primarily responsible for bladder function are the S2, S3, and S4 nerve roots. With significant compression of the cauda equina by either disk herniation, tumor, or degenerative stenosis, bladder dysfunction may result.
REFERENCES: Hoppenfeld S: Physical Examination of the Spine and Extremities. Norwalk, CT, Appleton-Century-Crofts, 1976, p 254.
Pick TP, Howden R (edS): Gray’s Anatomy. New York, NY, Bounty Books, 1977, p 1004.
Question 55:
A 16-year-old snowboarder has significant pain and is still unable to bear weight after sustaining a lateral ankle injury in a fall 1 week ago. Examination reveals swelling and tenderness in the sinus tarsi. AP, lateral, and mortise radiographs of the ankle are unremarkable. Management should consist of
Options:
- an elastic bandage, cold packs, and weight bearing as tolerated.
- non-weight-bearing and a CT scan of the talus.
- cast immobilization for 10 days, followed by progressive rehabilitation.
- cast immobilization for 6 weeks, followed by progressive rehabilitation.
- stirrup splinting, cold packs, and aggressive rehabilitation.
Correct Answer: non-weight-bearing and a CT scan of the talus.
Explanation:
DISCUSSION: Because there is a significant possibility that the patient may have a fracture of the lateral process of the talus, there is some disagreement as to the best radiographic study to identify this injury. A CT scan is an appropriate diagnostic tool to visualize the fracture and identify any displacement. Displaced lateral process fractures are best treated surgically.
REFERENCES: Kirkpatrick DP, Hunter RE, Janes PC, Mastrangelo J, Nicholas RA: The snowboarder’s foot and ankle. Am J Sports Med 1998;26:271-277.
Ebraheim NA, Skie MC, Podeszwa DA, Jackson WT: Evaluation of process fractures of the talus using computed tomography. J Orthop Trauma 1994;8:332-337.
Question 56:
Figure 39 shows the AP radiograph of a 62-year-old man with degenerative osteoarthritis secondary to trauma. History reveals that he underwent total elbow arthroplasty 3 years ago. He continues to report instability and constant pain. A complete work-up, including aspiration and cultures, is negative. Treatment should consist of removal of the components and
Options:
- distraction interpositional arthroplasty.
- elbow arthrodesis.
- conversion to a resection arthroplasty.
- conversion to semiconstrained elbow arthroplasty.
- revision to unconstrained total elbow arthroplasty.
Correct Answer: conversion to semiconstrained elbow arthroplasty.
Explanation:
DISCUSSION: An unconstrained prosthesis dislocation is a disconcerting problem that is not easily resolved; however, revision to a semiconstrained prosthesis would best achieve both pain relief and stability. Removal of the components and distraction arthroplasty or conversion to a resection arthroplasty are options, but the results would be unpredictable with regards to pain relief, postoperative motion, or elbow stability. Arthrodesis is poorly tolerated. With revision to another unconstrained prosthesis, there is the risk of continued redislocation because of chronic ligamentous insufficiency.
REFERENCES: Linscheid RL: Resurfacing elbow replacement arthroplasty: Rationale, technique and results, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 602-610.
Morrey BF, King GJ: Revision of failed total elbow arthroplasty, in Morrey BF (ed): The Elbow and Its Disorders, ed 3. Philadelphia, PA, WB Saunders, 2000, pp 685-700.
Question 57:
While performing long fusion with osteotomies for a patient with adult scoliosis and sagittal plane deformity, the neurophysiologist reports a change in motor-evoked potentials in the lower extremities. What is the most appropriate next step?
Options:
- Perform an immediate wake-up test
- Continue with the surgery and reassess in 5 minutes
- Administer intravenous methylprednisolone
- Ensure that mean arterial blood pressure is 80 or higher
Correct Answer: Ensure that mean arterial blood pressure is 80 or higher
Explanation:
DISCUSSION
The use of intraoperative neuromonitoring is expanding, especially in the setting of deformity surgery. Changes in monitoring are concerning for the possibility of a neurologic injury; however, several other factors can alter signals. These include hypotension, changes in anesthesia depth and medications, the use of paralytic agents, and technical issues such as leads falling out or becoming disconnected. If a change in neuromonitoring signals is noted, these factors should be checked first to rule out false-positive findings. If this does not correct the problem, the wound should be explored to ensure there is no compression on the neural elements. Finally, if the deformity has been corrected, some of the correction can be released in an attempt to improve the signals. A wake-up test is difficult to perform and does not provide specific information regarding the location of the problem or how to correct it. Steroids may be used depending on surgeon preference, but should not be used until neurologic injury is ruled out. Any neuromonitoring changes always necessitate immediate investigation.
RECOMMENDED READINGS
Ziewacz JE, Berven SH, Mummaneni VP, Tu TH, Akinbo OC, Lyon R, Mummaneni PV. The design, development, and implementation of a checklist for intraoperative neuromonitoring changes. Neurosurg Focus. 2012 Nov;33(5):E11. doi: 10.3171/2012.9.FOCUS12263. PubMed PMID: 23116091.
View
Abstract at PubMed
Malhotra NR, Shaffrey CI. Intraoperative electrophysiological monitoring in spine surgery. Spine (Phila Pa 1976). 2010 Dec 1;35(25):2167-79. doi: 10.1097/BRS.0b013e3181f6f0d0.
Review. PubMed PMID: 21102290.
View Abstract at PubMed
Question 58:
Figure 61 is the radiograph of a 34-year-old woman who was involved in a rollover motor vehicle accident. On arrival at the trauma center she is hypotensive and tachycardic. An abdominal CT scan reveals a spleen laceration. The patient remains hypotensive despite resuscitation and is taken to surgery for an emergent laparotomy and splenectomy. After surgery her delta base is -9 mmol/L. What is the most appropriate management of her pelvic ring injury? Review Topic
Options:
- Application of a pelvic binder
- Application of skeletal traction
- Open reduction and internal fixation
- Placement of percutaneous iliosacral screws
- Placement of an anterior pelvic external fixator
Correct Answer: Open reduction and internal fixation
Explanation:
The patient has a displaced iliac wing and bilateral rami fractures with superior migration of the right hip. To prevent further deformity, the patient's right hip should be placed into skeletal traction. A pelvic binder may worsen the deformity because of the iliac wing fracture. Anterior external fixation is problematic with an iliac wing fracture. Although the patient will eventually require open reduction and internal fixation and/or placement of iliosacral screws, she must be stabilized and resuscitated prior to this treatment.
(SBQ12TR.80) A 37-year-old male arrives to the trauma slot following a high-speed motorcycle crash. His Glasgow Coma score is 14 and his only orthopaedic injury is exhibited in Figure A. His current vital signs are a BP of 90/60, HR 120, and a lactate of 2.5 mMol/L. Other findings include a grade 1 splenic laceration and bilateral pulmonary contusions seen on chest radiograph. Which of the following has been suggested as an indication to perform damage control orthopedic care?
1 HR >110
Bilateral pulmonary contusions seen on chest radiograph
SBP = 90mmHg
Unilateral femur fracture
Lactate = 2.5 mMol/L
Pulmonary contusion severe enough to be diagnosed on chest radiograph alone is an indicator that the patient may benefit from damage control orthopaedics (DCO).
Despite the patient's overall stable nature, suffering pulmonary injury severe enough to be seen on x-ray alone suggests that temporary stabilization with staged definitive fixation may avoid potential morbidity.
Pape et al. review the evolution and balance of early total care (ETC) and DCO. Summarizing the literature, the authors report several standalone indicators that would justify DCO regardless of stable status. This includes: Injury Severity Score of greater than 40, Injury Severity Score of greater than 20 with chest trauma, multiple injuries with severe pelvic/abdominal trauma/ hemorrhagic shock, bilateral femoral fractures, pulmonary contusion noted on radiographs alone, hypothermia of less than 35 degrees C), and a head injury with an Abbreviated Injury Score of 3 or greater.
Figure A exhibits a right femoral shaft fracture. Illustration A exhibits a summarized table stating the criterion used to determine the condition of a polytrauma patient. (Table from Pape et al, PMID: 19726738)
Incorrect answers:
Question 59:
A 71-year-old woman with coronary artery disease underwent an uncomplicated right total hip arthroplasty for osteoarthritis 12 years ago. Her hip has functioned well until approximately 18 months ago when she noted the spontaneous onset of groin, buttock, and proximal thigh pain that is present at rest and made worse with activity. A radiograph is shown in Figure 15. What is the recommended management at this point?
Options:
- Immediate admission to the hospital and emergent revision hip arthroplasty
- Reassurance and follow-up if symptoms worsen
- Repeat radiographs in 1 month
- Protected weight bearing with urgent revision hip arthroplasty when the patient is medically cleared
- A prescription for alendronate and reevaluation in 1 year
Correct Answer: Protected weight bearing with urgent revision hip arthroplasty when the patient is medically cleared
Explanation:
DISCUSSION: The radiograph shows significant osteolysis with loosening of the femoral component. The patient is symptomatic and surgery is indicated because of the extent of osteolysis and the loose femoral component.
Reassurance and follow-up if symptoms worsen places the patient at risk for further bone loss and periprosthetic fracture. Emergent surgery is not required because the symptoms have been present for more than a year; however, urgent revision hip arthroplasty is recommended when the patient is medically cleared. While there is data to suggest that bisphosphonates may slow the progression of osteolysis in animal modes, there is no clear evidence that bisphosphonate treatment prevents the progression of osteolysis in humans. Additionally, this patient has a loose symptomatic femoral component.
REFERENCES: Chiang PP, Burke DW, Freiberg AA, et al: Osteolysis of the pelvis: Evaluation and treatment. Clin Orthop Relat Res 2003;417:164-174.
Dunbar MJ, Blackley HR, Bourne RB: Osteolysis of the femur: Principles of management. Instr Course Lect 2001;50:197-209.
Rubash HE, Dorr LD, Jacobs JJ, et al: Does alendronate inhibit the progression of periprosthetic osteolysis? Trans
Orthop Res Soc 2004;29:1888.
)
Figure 16a Figure 16b
Question 60:
Figures 4a through 4c show the clinical photographs and radiographs of a 12-month-old boy who has progressive difficulty wearing shoes because of the length of the second toe, as well as width of the forefoot. Management should consist of
Options:
- form-fitted shoes.
- amputation of the second toe at the metatarsophalangeal joint.
- amputation of the first ray and amputation of the second toe.
- amputation of the second ray.
- an MRI scan of the foot, a CT scan of the chest, and a biopsy of the foot with the possibility of ankle disarticulation amputation.
Correct Answer: amputation of the second ray.
Explanation:
DISCUSSION: The patient has macrodactyly involving the second ray, with significant enlargement of the width and height of the foot. The radiographs show widening of the interval between the first and second metatarsal and between the second and third metatarsal. With this degree of involvement, amputation of the second ray with excision of the overgrowth of affected soft tissue provides the most consistent desired reduction in foot size. A threaded Steinmann pin should be inserted across the remaining metatarsals until healing has occurred. Patients with macrodactyly should be examined to exclude neurofibromatosis type 1 and Klippel-Trenaunay-Weber syndrome.
REFERENCE: Sullivan JA: The child’s foot, in Morrissy RT, Weinstein SL (eds): Lovell & Winter’s Pediatric Orthopaedics, ed 4. Philadelphia, Pa, Lippincott-Raven, 1996, pp 1077-1135.
Question 61:
A 16-year-old boy has abdominal and back pain after being involved in a high-velocity head-on motor vehicle accident. He was restrained in the rear of the automobile by a lap belt only. A radiograph and CT scan are shown in Figure 47. The patient has no other injuries. Optimal management should include
Options:
- bed rest for 6 weeks.
- open reduction and internal fixation with spinous process wiring.
- cast immobilization in hyperextension for 6 weeks, followed by a thoracolumbosacral orthosis.
- anterior corpectomy, tricortical autograft, and fixation with a plate and screws.
- posterior fixation with a pedicle screw construct.
Correct Answer: cast immobilization in hyperextension for 6 weeks, followed by a thoracolumbosacral orthosis.
Explanation:
DISCUSSION: Pediatric bony Chance fractures occur following severe flexion injuries as seen after motor vehicle accidents with lap belt restraints. There is a high rate of associated intra-abdominal injuries. In the absence of associated injuries, these fractures are best treated with immobilization. Bed rest is not necessary. Surgical fixation usually is not needed. Surgical stabilization and two-level fusion may be indicated in select individuals with progressive kyphosis of more than 25° or other conditions that preclude cast or brace immobilization.
REFERENCES: Greenwald TA, Mann DC: Pediatric seatbelt injuries: Diagnosis and treatment of lumbar flexion-distraction injuries. Paraplegia 1994;32:743-751.
Glassman
SD
, Johnson JR, Holt RT: Seatbelt injuries in children. J Trauma 1992;33:882-886.
Raney EM, Bennett JT: Pediatric Chance fracture. Spine 1992;17:1522-1524.
Question 62:
Thermal capsulorrhaphy of the inferior glenohumeral ligament can cause iatrogenic injury to which of the following nerves?
Options:
- Musculocutaneous
- Suprascapular
- Radial
- Axillary
- Median
Correct Answer: Axillary
Explanation:
DISCUSSION: The axillary nerve courses from anterior to posterior just below the inferior shoulder capsule. Thermal energy applied to the inferior aspect of the shoulder capsule can result in injury to this nerve.
REFERENCES: Wong KL, Williams GR: Complications of thermal capsulorrhaphy of the shoulder. J Bone Joint Surg Am 2001;83:151-155.
Bryan WJ, Schauder K, Tullos HS: The axillary nerve and its relationship to common sports medicine shoulder procedures. Am J Sports Med 1986;15:113-116.
Question 63:
A well-healed bulk proximal tibia osteoarticular allograft is removed 10 years after implantation due to arthropathy. Histologic examination of the host allograft junction site will most likely reveal
Options:
- bridging external callus along the allograft and perpendicular callus at the junction site.
- direct osteonal penetration of the allograft with haversian remodeling.
- complete incorporation of the allograft with obliteration of the host allograft junction site.
- fibrovascular invasion with absence of callus formation.
- gap formation with resorption of the allograft surface.
Correct Answer: bridging external callus along the allograft and perpendicular callus at the junction site.
Explanation:
Retrieval studies of well-fixed bulk allografts reveal that the junction site heals with bridging external callus and there is persistence of callus perpendicular to the junction site. External callus is annealed to the surface of the allograft. There is very little penetration of the allograft and the bone graft is not remodeled. Direct osteonal penetration of the allograft with haversian remodeling defines primary bone healing seen in fractures, which does not occur with allografts. Fibrovascular tissue is seen early in the healing phase of the cancellous portion of the allografts.
Question 64:
below show the radiographs obtained from a year-old woman with a year history of progressive hip pain in the left groin with activity, which is unresponsive to activity modification and physical therapy. Examination reveals normal range of motion, with pain on anterior impingement testing. What treatment is associated with the best long-term results?
Options:
- Hip arthroscopy with labral repair B. Reverse periacetabular osteotomy C. Varus rotational osteotomy
- Open surgical dislocation with rim trimming
Correct Answer: Open surgical dislocation with rim trimming
Explanation:
DISCUSSION:
This patient has symptomatic femoroacetabular impingement as well as clinical and radiographic signs of acetabular retroversion, including a cross-over sign, ischial spine sign, and posterior wall sign bilaterally. Good midterm to long-term outcomes have been reported with reverse (anteverting) Bernese periacetabular osteotomy (PAO). In patients with less retroversion, open or arthroscopic rim trimming with labral refixation have shown good short-term results, but longer-term results have yet to be fully delineated. Isolated hip arthroscopy and labral repair would not be indicated without addressing the retroversion deformity. Femoral varus rotational osteotomy plays no role in the treatment of this pathology. Open surgical dislocation with rim trimming could be considered in patients with less deformity, but some studies have shown inferior long-term results compared with reverse PAO.
Question 65:
What is the plasma half-life of warfarin?
Options:
- 1 to 2 hours
- 4 to 6 hours
- 12 to 18 hours
- 36 to 42 hours
Correct Answer: 36 to 42 hours
Explanation:
Warfarin, which is dosed daily, can take 72 to 96 hours to reach therapeutic levels. It has a plasma half-life of 36 to 42 hours. Low-molecular heparins have a plasma half-life of 4 to 5 hours, and fondaparinux has a half-life of 17 to 21 hours. Warfarin will not affect the International Normalized Ratio (INR) until 2 to 3 days after it is given. Patients on chronic warfarin therapy should have treatment stopped 3 to 5 days before elective surgery to allow the INR to normalize.
Question 66:
…Giant-cell tumor of bone usually involves the epiphysis of long bones. What is the next most common type of tumor involving this anatomical location?
Options:
- Conventional chondrosarcoma
- Aneurysmal bone cyst
- Chondroblastoma
- Osteoblastoma DISCUSSION.. Giant-cell tumor is the most common lesion involving the epiphysis, although its epicenter is usually in the metaphysis, and in the rare case of giant-cell tumor occurring in a skeletally immature patient, giant-cell tumor is located in the metaphysis. It also can involve the flat bone of the pelvis and sacrum. Chondroblastoma exclusively occurs in the epiphysis of skeletally immature patients. It is more common than the other responses. Although conventional chondrosarcoma does not involve the epiphysis, clear-cell chondrosarcoma involves the epiphysis as well; however, it is rare and less common than chondroblastoma. Aneurysmal bone may occur in the epiphysis; however, it is often seen with other benign tumors such as chondroblastoma or giant-cell tumor. It is less common in this location than chondroblastoma. Osteoblastoma does not classically appear at the epiphysis. It is more commonly seen in the spine or the diaphysis of long bones.
Correct Answer: Chondroblastoma
Explanation:
CLINICAL SITUATION FOR QUESTIONS 71 THROUGH 73
Figures 71a through 71e are the radiographs, MRI scan, and CT scans of a 14-year-old-boy who has cyclical pain in his thigh. His symptoms began approximately 6 months ago. He complains of increased pain when he runs and also of pain that wakes him at night. This pain is relieved by nonsteroidal anti-inflammatory drugs (NSAIDs).
Question 67:
Venous thrombolembolism is a common complication following total hip and total knee arthroplasty; therefore, prophylaxis is deemed efficacious. Several studies on low-molecular-weight heparin (LMWH) have shown which of the following findings?
Options:
- LMWH is associated with bleeding complications of less than 1% and may be administered immediately after surgery.
- LMWH is superior to adjusted-dose warfarin.
- LMWH acts on several sites of the coagulation cascade, with its principal action inhibition of factor 10a.
- LMWH and unfractionated heparin are equally likely to cause thrombocytopenia.
- LMWH may be used in conjunction with regional anesthesia and is not contraindicated in patients with indwelling epidural catheters.
Correct Answer: LMWH acts on several sites of the coagulation cascade, with its principal action inhibition of factor 10a.
Explanation:
DISCUSSION: Prophylactic LMWH is associated with a risk of bleeding complications, especially if administered too soon after surgery. The risk of major bleeding is 0.3% for control, 0.4% for aspirin, 1.3% for warfarin, 1.8% for LMWH, and 2.6% for unfractionated heparin. Colwell and associates conducted a prospective, randomized trial on over 1,500 total hip arthroplasty patients. Overall, the risk of clinically apparent venous thrombolembolism was 3.6% for LMWH and 3.7% for warfarin. LMWH acts in several sites of the coagulation cascade, with its principal action being inhibition of factor 10a. Thrombocytopenia is less common with LMWH than with unfractionated heparin. The use of LMWH is a relative contraindication with indwelling epidural anesthesia.
REFERENCES: Colwell CW Jr, Collis DK, Paulson R, et al: Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty:. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999;81:932-940.
Salvati EA, Pelligrini VD Jr, Sharrock NE, et al: Recent advances in venous thromboembolic prophylaxis during and after total hip replacement. J Bone Joint Surg Am 2000;82:252-270.
Question 68:
Dislocation following primary total hip arthroplasty is more likely to occur in which of the following situations?
Options:
- Women rather than men
- Younger patients rather than older patients
- Ceramic-on-polyethylene bearings rather than cobalt-chromium on polyethylene bearings
- Cemented rather than cementless femoral components
- Metal-on-polyethylene rather than metal-on-metal bearings of the same diameter
Correct Answer: Women rather than men
Explanation:
DISCUSSION: Dislocation following total hip arthroplasty is twice as common in women than in men. It is more likely to occur in older patients. There is no clear association between dislocation and the method of fixation or the type of bearing, so long as the bearing diameter is the same.
REFERENCE: Berry DJ: Dislocation, in Steinberg ME (ed): Revision Total Hip Arthroplasty. Philadelphia, PA, 1999, pp 463-482.
Question 69:
A 75-year-old man presents with a displaced femoral neck fracture. During your surgical exposure for a hemiarthroplasty, the femoral neck has fractured through a pathologic lesion which is diagnosed as a lymphoma on frozen section. The lesion is located in the center of the femoral neck and the calcar femorale is not involved. Your treatment should include:
Options:
- Closure of the wound and chemotherapy
- Radical resection of the proximal femur and megaprothesis hemiarthroplasty
- Hemiarthroplasty with postoperative staging and chemo-radiotherapy as indicated
- Bone marrow transplantation
- Hip disarticulation
Correct Answer: Hemiarthroplasty with postoperative staging and chemo-radiotherapy as indicated
Explanation:
This case presents a treatment dilemma for most orthopaedic surgeons. However, because lymphomas are very chemo-radiotherapy sensitive, treatment is straightforward. Lymphoma isolated to bone is treated by resection and reconstruction as indicated. In this case, the resection is accomplished with neck osteotomy and the reconstruction with a hemiarthroplasty. Postoperative adjuvant radiotherapy and chemotherapy can be used to treat the local and distant disease as necessary. You wouldn't close the wound without surgical fixation unless the chemotherapy would be used to improve your surgical margin (such as for a osteosarcoma). Radical resection or hip disarticulation are very aggressive and morbid procedures for a tumor that is very sensitive to chemo-radiotherapy. Bone marrow transplantation is not used in the initial treatment of lymphoma, but can be considered for relapsed disease.
The clinical and radiographic features specific to lymphoma of bone are outlined by Dürr but on the whole are not diagnostic.
Vose describes the current treatment protocols for patients with non-Hodgkin's lymphoma including patients with impending/sustained pathologic fractures.
Question 70:
A 12-year-old girl has had progressive left knee pain for the past 4 months. She reports that the pain is unrelated to activity, and she has no history of fever or recent infections. Examination reveals full range of motion of the knee but tenderness along the medial joint line. Plain radiographs and MRI scans are shown in Figures 39a through 39d. A biopsy specimen of the lesion is shown in Figure 39e. Treatment should include
Options:
- curettage.
- systemic antibiotics.
- observation and protected weight bearing.
- chemotherapy.
- radiation therapy.
Correct Answer: curettage.
Explanation:
DISCUSSION: The lesion is a chondroblastoma. The plain radiographs show a well-defined radiolucent lesion in the distal femoral epiphysis of a skeletally immature patient. The margins are well defined, suggesting a benign growth. The epiphysis is an unusual location for bone tumors, except for chondroblastomas. Of all chondroblastomas, 95% are located within the epiphysis. The MRI scans show a punctate appearance that is commonly seen in cartilage lesions. The biopsy specimen shows a chondroid lesion with polygonal chondrocytes. These findings are consistent with a chondroblastoma. The natural history of chondroblastomas is for continued growth and bone destruction if left untreated. Treatment should consist of curettage, with or without the use of physical or chemical adjuvants, and bone grafting.
REFERENCE: Springfield DS, Capanna R, Gherlinzoni F, Picci P, Campanacci M: Chondroblastoma: A review of seventy cases. J Bone Joint Surg Am 1985;67:748-755.
Question 71:
Which of the following is a true statement regarding thoracic disk herniations? Review Topic
Options:
- Are most commonly discovered during the fifth to seventh decades of life
- Occur with similar frequency as cervical disk herniations
- Occur most commonly in the midthoracic or apical region of the spine
- Can be found in 40% of asymptomatic individuals
- Are best treated surgically with posterior laminectomy and excision
Correct Answer: Can be found in 40% of asymptomatic individuals
Explanation:
Symptomatic herniations of the thoracic spine are much less common than those of the cervical or lumbar region. They tend to occur most commonly during the third to fifth decades of life and although they can be found at all levels, they are most
common in the lower third near the thoracolumbar region. Posterior laminectomy and disk excision has the highest rate of neurologic deterioration and is not recommended. Multiple studies have shown that herniated thoracic disks can be found at one or more levels in 40% of asymptomatic individuals.
Question 72:
Which of the following clinical tests is used to diagnose medial instability of the elbow? Review Topic
Options:
- Posterolateral rotatory drawer test
- Lateral pivot-shift test
- Moving valgus stress test
- Chair test (apprehension or dislocation on terminal extension of the supinated forearm when rising from a seated position)
- Pushup sign
Correct Answer: Moving valgus stress test
Explanation:
The moving valgus stress test is used in the diagnosis of medial collateral ligament instability of the elbow. The other tests apply a varus force to the elbow and are used to diagnose lateral ulnar collateral insufficiency.
Question 73:
Figure 10 shows the AP radiograph of an ambulatory 76-year-old patient. What is the most appropriate surgical treatment option for this patient?
Options:
- Revision arthroplasty using a cemented femoral component
- Impaction allografting of the femoral component
- Proximal femoral replacement arthroplasty
- Resection arthroplasty
- Hip arthrodesis
Correct Answer: Proximal femoral replacement arthroplasty
Explanation:
DISCUSSION: The patient has a periprosthetic fracture around a loose cemented femoral component. The proximal bone stock is poor; therefore, this fracture may be categorized as Vancouver 3-B. Hip arthrodesis and resection arthroplasty provide suboptimal results, particularly for ambulatory patients. Although impaction allografting may be an option to restore the bone stock in a younger patient, the latter procedure will be very difficult to perform when the proximal bone is poor in quality and fractured. Cementing another component into this wide femur is not an option. The best option for revision of the femoral component in this elderly patient is proximal femoral replacement arthroplasty.
REFERENCES: Malkani AL, Settecerri JJ, Sim FH, et al: Long-term results of proximal femoral replacement for non-neoplastic disorders. J Bone Joint Surg Br 1995;77:351-356.
Parvizi J, Sim FH: Proximal femoral replacements with megaprostheses. Clin Orthop 2004;420:169-175.
Question 74:
Figures 20a through 20c show the radiographs of a 69-year-old woman who has severe pain in her dominant right arm after falling on the ice. History includes arthritis, hypertension, and heart disease. She is neurovascularly intact. Management should consist of
Options:
- a long arm cast.
- immediate functional bracing.
- closed reduction and percutaneous pin fixation.
- percutaneous olecranon pin traction.
- total elbow arthroplasty.
Correct Answer: total elbow arthroplasty.
Explanation:
DISCUSSION: The radiographs reveal a severely comminuted distal humerus fracture. A long arm cast, functional bracing, and closed reduction and percutaneous pin fixation all have a poor outcome and could result in a nonunion that will be very difficult to treat. Open reduction and internal fixation is indicated in most supracondylar humerus fractures, but total elbow arthroplasty is a good alternative in elderly patients who have multiple medical problems and when the fracture pattern may preclude stable enough internal fixation to allow postoperative motion.
REFERENCES: Cobb TK, Morrey BF: Total elbow arthroplasty as primary treatment for distal humeral fractures in elderly patients. J Bone Joint Surg Am 1997;79:826-832.
Morrey BF: Fractures of the distal humerus: Role of elbow replacement. Orthop Clin North Am 2001;31:145-155.
Question 75:
A 27-year-old professional baseball pitcher who underwent arthroscopic olecranon debridement continues to have medial-sided elbow pain during late cocking. Physical examination reveals laxity and pain with valgus stress testing. What is the most likely cause of his pain? Review Topic
Options:
- Ulnar neuritis
- Excessive olecranon resection
- Osteochondritis dissecans of the capitellum
- Olecranon stress fracture
- Valgus extension overload
Correct Answer: Excessive olecranon resection
Explanation:
Both the medial collateral ligament and the olecranon contribute to valgus stability of the elbow. Excessive olecranon resection increases the demand placed on the medial collateral ligament in resisting valgus forces during throwing. Bone removal from the olecranon should be limited to osteophytes.
Question 76:
An 83-year-old woman with a long history of her foot slowly and progressively “turning out” now reports significant ankle pain. History reveals that she has significant cardiac disease and exercise-induced angina. Examination reveals a deficiency in the posterior tibial tendon; however, the hindfoot remains moderately supple. Radiographs reveal a valgus tilt of the tibiotalar joint and early arthrosis. What is the most appropriate orthotic management?
Options:
- Total contact orthotic
- UCBL orthotic
- Molded articulated ankle-foot orthosis
- Molded ankle gauntlet (Arizona brace)
- Lateral heel flare
Correct Answer: Molded ankle gauntlet (Arizona brace)
Explanation:
DISCUSSION: The patient will continue to have pain secondary to the ankle arthrosis with both the UCBL and the molded articulated ankle-foot orthosis. The total contact orthotic does not provide enough hindfoot control to support the progressive collapse of the ankle into valgus positioning. A molded leather gauntlet will not only control tibiotalar motion but also control hindfoot motion and allow support of the longitudinal arch.
REFERENCE: Augustin JF, Lin SS, Berberian WS, et al: Nonoperative treatment of adult acquired flat foot with the Arizona brace. Foot Ankle Clin 2003;8:491-502.
Question 77:
The best definitive treatment for this patient’s left knee is
Options:
- total knee replacement.
- knee arthrodesis using an anterior plate and screws.
- knee arthrodesis using an external fixator.
- observation.
Correct Answer: observation.
Explanation:
DISCUSSION
This patient now has a major fixed flexion contracture and severe varus alignment and instability. Infection of the knee joint has to be ruled out. The radiograph shows all the hallmarks of Charcot arthropathy, including disintegration and fragmentation of the joint with major deformity. Infection of the knee joint and contiguous osteomyelitis still have to be ruled out. The clinical and radiographic findings are highly suggestive of a Charcot neurogenic arthropathy associated with uncontrolled diabetes. This patient is an unsuitable candidate for total knee arthroplasty (TKA) because he is noncompliant regarding his diabetes and has had a previously infected native joint that now is associated with Charcot arthropathy. He is nonambulatory. The failure rate of TKA or knee arthrodesis is extremely high in this setting. He will best be served with observation or amputation depending upon his symptom severity.
Question 78:
Which of the following methods of treating a vertically oriented (eg, Pauwels III) femoral neck fracture is mechanically optimal?
Options:
- Two parallel fully threaded screws
- Three parallel partially threaded screws
- Three parallel fully threaded screws
- Four parallel partially threaded screws
- Sliding hip screw and side plate
Correct Answer: Two parallel fully threaded screws
Explanation:
Vertical fractures have a higher rate of displacement and nonunion because of shearing forces across the fracture. Biomechanical and clinical studies indicate that for the vertically oriented fracture of the femoral neck, the most stable fixation construct is a sliding hip screw and side plate. Antirotation screws may be used as well. Nonsurgical management carries a high risk of early displacement because of shear forces. Three screws are loaded as a cantilever and have less resistance to displacement compared with a fixed-angle device with a side plate. Fully threaded screws will not allow any compression and have the same drawbacks as partially threaded screws. The addition of a fourth screw has not been shown to be of benefit.
(SBQ12TR.68) Figure A is a radiograph of a 75-year-old woman that fell onto her non-dominant shoulder from a standing height. She was treated non-operatively for 9 months but continues to complain of pain when she elevates her arm. In patients with this type of fracture pattern, what factor has the greatest impact on fracture healing?
Hand dominance
Angulation of fracture
Smoking
Early physical therapy
Diet
This patient has an impacted varus proximal humerus fracture. Smoking has been shown to increase the nonunion risk up to 5.5 times with these fractures.
Impacted varus proximal humerus fractures can be managed effectively with nonoperative care. The major factors that influence non-union are age and smoking. Solid bony union can be seen in 93-98% of patients at 1 year, with more than 97% of people returning to pre-injury level of function. The angulation of fracture, hand dominance and physical therapy does not seem to influence bone union or functional outcomes with this fracture pattern.
Court-Brown et al. looked at the outcomes of impacted varus fractures. They determined that the age of the patient was the major factor in overall outcome. They showed that the best results occurred in younger patients, but results deteriorate with advancing age. Physical therapy was not found to impact outcome.
Hanson et al. showed that impacted varus fractures can be successfully managed with non-operative care. They found that overall fracture displacement had a minor impact of fracture healing and functional outcome. The predicted risk of delayed union and nonunion was 7% with patients that smoke. This was 5.5 times greater than nonsmokers.
Figure A shows an AP radiograph of a varus angulated proximal humerus fracture. This radiograph shows delayed atrophic union.
Incorrect Answers:
Question 79:
Figure 44 shows the radiograph of an 11-year-old girl who has hip pain. Further diagnostic workup should include
Options:
- a renal ultrasound.
- an echocardiogram.
- an electromyogram.
- an MRI scan of the spine.
- an iliac crest biopsy.
Correct Answer: an echocardiogram.
Explanation:
DISCUSSION: The patient has severe acetabular protrusio, a condition that is frequently associated with Marfan syndrome. An echocardiogram is necessary to rule out the most serious consequence of this syndrome, aortic root widening, which can lead to aortic valve dysfunction or fatal aortic rupture. An electromyogram may be indicated for Charcot-Marie-Tooth disease, which is associated with acetabular dysplasia, but not protrusio. The renal ultrasound, the MRI scan, and the biopsy would be of no value in this patient. Protrusio can also be seen in patients with osteogenesis imperfecta and juvenile rheumatoid arthritis.
REFERENCES: Steel HH: Protrusio acetabuli: Its occurrence in the completely expressed Marfan syndrome and its musculoskeletal component and a procedure to arrest the course of protrusion in the growing pelvis. J Pediatr Orthop 1996;16:704-718.
Wenger DR, Ditkoff TJ, Herring JA, Mauldin DM: Protrusio acetabuli in Marfan’s syndrome. Clin Orthop 1980;147:134-138.
Question 80:
Figure 1 is the T2 coronal MRI scan of a 52-year-old woman with a 6- month history of shoulder pain. She does not recall a history of trauma. Physical therapy is recommended. What is the most significant predictor of failure of nonoperative treatment?
Options:
- Tear size
- Pain scale score
- Strength deficit
- Patient expectations The MRI reveals a large full thickness supraspinatus tear. A large, prospective study showed that physical therapy can be effective in the treatment of atraumatic full-thickness rotator cuff tears. Patient expectations regarding the role of rehabilitation were the strongest predictor of surgery. Other factors associated with surgery were higher activity level and not smoking. Anatomic features of the rotator cuff tear and the severity of patient’s reported pain did not predict failure of nonoperative treatment. Patients who have low expectations regarding the effectiveness of physical therapy are more likely to fail nonoperative treatment.
Correct Answer: Patient expectations The MRI reveals a large full thickness supraspinatus tear. A large, prospective study showed that physical therapy can be effective in the treatment of atraumatic full-thickness rotator cuff tears. Patient expectations regarding the role of rehabilitation were the strongest predictor of surgery. Other factors associated with surgery were higher activity level and not smoking. Anatomic features of the rotator cuff tear and the severity of patient’s reported pain did not predict failure of nonoperative treatment. Patients who have low expectations regarding the effectiveness of physical therapy are more likely to fail nonoperative treatment.
Explanation:
Figures 1 through 3 are the MRI scans of a 51-year-old active man who injured his right shoulder after a fall while sailing 4 days ago. Optimal surgical management of the patient’s pathology is expected to involve
Question 81:
A 45-year-old man who underwent an ankle arthrodesis reports that for the first 6 years he had significant pain relief after the fusion healed. However, he now has increasing pain in the sinus tarsi. AP and lateral radiographs are shown in Figures 8a and 8b. What is the most likely cause of the patient’s symptoms?
Options:
- Nonunion
- Tarsal tunnel syndrome
- Degenerative arthritis of the hindfoot joints
- Sinus tarsi syndrome
- Chronic osteomyelitis of the distal tibia
Correct Answer: Degenerative arthritis of the hindfoot joints
Explanation:
DISCUSSION: The patient has a solid ankle fusion radiographically. With a tibiotalar arthrodesis, the adjacent joints (subtalar and transverse tarsal) take additional stress. Over time, progressive degenerative arthritis will occur in these adjacent joints, often necessitating further surgery.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 613-631.
Coester LM, Saltzman CL, Leupold J, Pontarelli W: Long-term results following ankle arthrodesis for post-traumatic arthritis. J Bone Joint Surg Am 2001;83:219-228.
Question 82:
Which of the following is an indication for surgical management of a Weber type B distal fibular fracture?
Options:
- Medial hindfoot ecchymosis
- Medial ankle tenderness
- Widened medial clear space
- Comminution
- Two millimeters of fibular displacement
Correct Answer: Widened medial clear space
Explanation:
DISCUSSION: A widened medial clear space indicates instability caused by an associated tear of the deltoid ligament; therefore, nonsurgical management is not warranted. Weber type B distal fibular fractures without a deltoid tear have a medial clear space of < 4 mm, even under stress, and may be successfully treated nonsurgically. The presence of medial hindfoot ecchymosis and medial ankle tenderness is not fully indicative of medial soft-tissue instability; however, these findings may indicate a deltoid injury and should raise suspicion of an unstable fracture injury pattern. Stress testing is necessary to demonstrate the presence or absence of instability. A small amount of comminution is also cause for increased suspicion of an unstable pattern; however, it is not a direct contraindication when considering nonsurgical management. Two millimeters of fibular displacement without lateral shift of the talus is an acceptable position when considering nonsurgical management of Weber type B distal fibular fractures.
REFERENCES: Michelson JD, Magid D, Ney DR, et al, Examination of the pathologic anatomy of ankle fractures. J Trauma 1992;32:65-70.
Marsh JL, Saltzman CL: Ankle fractures, in Rockwood & Green’s Fractures in Adults, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 2001-2090.
Question 83:
Figure 17 shows the radiograph of an 80-year-old woman who has left groin pain. She underwent a total hip arthroplasty 15 years ago and has no history of hip dislocation; however, she now reports that the pain results in functional impairment. Preoperative findings reveal that the component used has been discontinued, the locking mechanism is poor, and there is no replacement polyethylene available from the company. During surgery, the acetabular component is found to be well fixed, it is in satisfactory position, and adequate access can be obtained through the screw holes in the component to debride the osteolytic cavities. What is the best course of action for revision?
Options:
- Remove the component and replace it with a “jumbo” cup with bone graft or substitute.
- Remove the component and replace it with a bipolar component with bone graft or substitute.
- Remove the component and replace it with a support ring with graft or graft substitute and cement a cup into the support ring.
- Score the component for improved cement interdigitation and cement a cup into the retained socket with bone graft or substitute.
- Use a structural acetabular graft to reconstruct the acetabulum and cement a cup into the structural graft.
Correct Answer: Score the component for improved cement interdigitation and cement a cup into the retained socket with bone graft or substitute.
Explanation:
DISCUSSION: The clinical result in this patient has been good, with no dislocations, suggesting that the components are in reasonably good position. The radiograph and examination at the time of surgery suggest that the acetabular component is well fixed. The surrounding bone of the acetabulum is osteopenic and there would most likely be considerable bone loss if the acetabular component is removed. Access to the osteolytic lesions is possible. Cementing an acetabular component into the retained socket will cause the least amount of bone loss, shorten the procedure, and most likely result in a functional hip.
REFERENCES: Maloney WJ: Socket retention: Staying in place. Orthopedics 2000;23:965-966.
Blaha JD: Well-fixed acetabular component retention or replacement: The whys and the wherefores. J Arthroplasty 2002;17:157-161.
Question 84:
A 52-year-old woman has bicompartmental osteoarthritis following patellectomy. Treatment should consist of
Options:
- high tibial osteotomy.
- arthroscopic debridement.
- patella arthroplasty.
- total knee arthroplasty.
- knee arthrodesis.
Correct Answer: total knee arthroplasty.
Explanation:
DISCUSSION: The patient has extensive degenerative changes in both the medial and lateral compartments within the knee; therefore, arthroscopic debridement or an osteotomy will not be helpful. A patellar arthroplasty will not address the medial and lateral compartments. Because the extensor mechanism provides a significant amount of anteroposterior stability, a posterior cruciate-substituting total knee arthroplasty is the treatment of choice for this patient.
REFERENCES: Martin SD, Haas SB, Insall JN: Primary total knee arthroplasty after patellectomy. J Bone Joint Surg Am 1995;77:1323-1330.
Pagnano MW, Cushner FD, Scott WN: Role of the posterior cruciate ligament in total knee arthroplasty. J Am Acad Orthop Surg 1998;6:176-187.
Question 85:
A 23-year-old man cut the dorsal and ulnar aspects of his long finger on a table saw. The dorsal and ulnar skin over the middle phalanx is missing, with a 2-cm x 2-cm area of loss. There is a 50% loss of the extensor tendon (ulnar), and the remaining tendon has no tenosynovium. The physician should recommend irrigation and debridement and
Options:
- tendon repair, and thenar flap coverage.
- full-thickness skin graft.
- reversed cross-finger flap from the ring finger.
- cross-finger flap coverage from the ring finger.
Correct Answer: reversed cross-finger flap from the ring finger.
Explanation:
EXPLANATION:
The patient has exposed bone and tendon and a partial tendon injury. The remaining radial tendon is satisfactory and no tendon repair is required. The exposed bone and tendon necessitate vascularized tissue coverage. A reversed cross-finger flap from the ring finger is suitable for coverage of the dorsal surface of an adjacent digit.
Question 86:
The usual presentation of traumatic subscapularis tears is most often seen after forced Review Topic
Options:
- internal rotation.
- external rotation.
- extension.
- abduction.
- forward flexion.
Correct Answer: external rotation.
Explanation:
The typical mechanism of injury is a fall and the patient grasps something to prevent the fall. This maneuver forces the arm into external rotation against resistance.
Question 87:
A 58-year-old man has a painful, warm, erythematous and fluctuant area over his left olecranon. An aspiration would be most likely to reveal
Options:
- Staphylococcus aureus.
- Streptococcus pyogenes.
- Enterococcus faecalis.
- Psuedomonas aurigonosa.
Correct Answer: Staphylococcus aureus.
Explanation:
Discussion: Staphylococcus aureus is the most common causative organism in septic bursitis, making up 80% or more of cases of culture-proven septic bursitis (
https://www.uptodate.com/contents/septic-bursitis
). Staphylococcus aureus was the most frequent pathogen (217 out of 256 or 85%), followed by Streptococcus pyogenes (16), other streptococci (15), Enterococcus faecalis (4) and coagulase-negative staphylococci (2). Staphylococcus aureus is the most common causative organism in septic bursitis, making up 80% or more of cases of culture-proven septic bursitis (
https://www.uptodate.com/contents/septic-bursitis
). Staphylococcus aureus was the most frequent pathogen (217 out of 256 or 85%), followed by Streptococcus pyogenes (16), other streptococci (15), Enterococcus faecalis (4) and coagulase-negative staphylococci (2).
Question 88:
A 23-year-old man reports pain on the superior aspect of his right shoulder with repetitive overhead activities and when lying on his right side. Figure 29 shows an axial MRI scan. What is the most likely diagnosis based on the MRI findings? Review Topic
Options:
- Osteoarthritis of the acromioclavicular joint
- Acromioclavicular joint separation
- Os acromiale
- Partial-thickness rotator cuff tear
- Superior labral tear
Correct Answer: Os acromiale
Explanation:
Os acromiale represents a failure of fusion of the anterior acromial apophysis and has been reported in approximately 8% of the population. Patients with a symptomatic os acromiale often report impingement-type symptoms with pain over the superior acromion, especially with overhead activities or sleeping. When nonsurgical management is unsuccessful, surgical options include excision, open reduction and internal fixation, and arthroscopic decompression.
Question 89:
A 24-year-old man has had pain in the left knee for the past several months. He reports that initially the pain was associated with weight-bearing activities, but it has now become more constant. He denies any swelling but reports a lateral fullness at the tibial plateau. Figures 23a through 23e show radiographs, a bone scan, and T1- and T2-weighted MRI scans. What is the most likely diagnosis?
Options:
- Stress fracture
- Simple bone cyst
- Fibrous dysplasia
- Infection
- Giant cell tumor
Correct Answer: Giant cell tumor
Explanation:
DISCUSSION: The radiographs reveal a lytic subchondral lesion that has a poorly defined margin and lacks mineralization. The bone scan confirms an active lesion that has central photopenia, producing the characteristic doughnut configuration. The MRI scans confirm the presence of a subchondral lesion that is modestly expansile at the lateral plateau and has low signal intensity on the T1-weighted image and a mixed high signal on the T2-weighted image. These features strongly suggest giant cell tumor of bone, more than 50% of which appear around the knee. Simple cyst is excluded by the MRI characteristics. Fibrous dysplasia is unlikely to be in a subchondral location and typically does not show this intensity of uptake on bone scan.
REFERENCES: Parsons TW: Benign bone tumors, in Fitzgerald RH, Kaufer H,
Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1027-1035.
Resnick D, Kyriakos M, Greenway GD: Tumors and tumor-like lesions of bone: Imaging and pathology of specific lesions, in Resnick D (ed): Diagnosis of Bone and Joint Disorders, ed 4. Philadelphia, PA, WB Saunders, 2002, vol 4, pp 3939-3962.
Question 90:
Figures A and B are radiographic images of an 85-year-old woman with isolated left hip pain. She describes a non-syncopal fall from standing 4 hours ago. Physical examination reveals pain with log-rolling the left thigh and the inability to bear weight on the affected leg. The radiologist reports no fracture in the left hip. What would be the next best step? Review Topic
Options:
- Stress view radiographs of the left hip
- Non-weight bearing and pelvic bone scan in 7 days
- Non-weight bearing and repeat the CT scan after 48 hours from injury
- MRI hip and pelvis
- Weight bearing activity as tolerated with close follow-up
Correct Answer: Stress view radiographs of the left hip
Explanation:
The next best step would be an MRI hip and pelvis to investigate for an occult fracture of the left hip.
Moderate evidence supports MRI as the advanced imaging of choice for diagnosis of presumed hip fracture not apparent on initial radiographs. MRI has been shown to be able to detect occult fractures earlier than bone scan, with better spatial resolution. Usually the MRI should be obtained in less than 24 hours from the time of injury. For situations in which MRI is not immediately available, bone scan can be considered after 72 hours form the time of injury. However, this may compromise patient care and put the patient at risk of fracture displacement.
Cannon et al. reviewed the imaging of choice in occult hip fracture. They showed that physical examination yields a poor sensitivity identifying occult hip fractures, with log-rolling and straight-leg raise as 50% and 70%, respectively. The most sensitive modality for occult fracture identification was MRI.
Iwata et al. retrospectively reviewed a cohort of 35 patients with clinically suspected fractures of the hip that underwent MRI. All radiographs were negative. In 26 of these patients, a T1-weighted coronal MRI showed a hip fracture with 100% sensitivity.
Roberts et al. reviewed the 2015 AAOS Clinical Practice Guideline: Management of Hip Fractures in the Elderly. They report moderate evidence that supports MRI as the advanced imaging of choice for diagnosis of presumed hip fractures not apparent on initial radiographs.
Figure A is a AP radiograph of the left hip and pelvis. Apart from a healed fracture of the ischiopubic rami and generalized osteopenia, there is no obvious hip fracture. Figure B is a coronal CT image that does not demonstrate evidence of an acute hip fracture. Illustration A is a T1 weighted MR image that shows a non displaced fracture (white arrow) through the intertrochanteric region of the left proximal femur.
Incorrect Answers:
(SBQ12TR.32) A 20-year-old male is taken to the emergency department following a motorcycle collision with the injury seen in Figures A and B. He undergoes serial debridements with placement of an antibiotic bead pouch, followed by intramedullary nailing and free tissue transfer. His preoperative examination is notable for absent plantar sensation. Which of the following is predictive of a worse long term outcome in this patient?
Absent plantar sensation at presentation
Depression at 3 months post-injury
Use of an intramedullary nail
Free tissue transfer instead of rotational flap
Need for multiple debridements
The presence of depression at the 3 months post-injury is a significant predictor of worse long term outcome as well as lower return to work rates in patients that present with limb threatening lower extremity trauma.
The findings of the Lower Extremity Assessment Project (LEAP study) has challenged many of the long-held beliefs of lower extremity trauma surgery, including the concept that patients with absent plantar sensation should undergo immediate amputation . The LEAP study has also brought to light the importance of socioeconomic and psychosocial factors in patient outcomes following these injuries.
Bosse et al analyzed a subgroup of 55 patients from the LEAP study with absent plantar sensation at presentation. Those patients that underwent limb salvage despite absent sensation (n=26) had no significant difference in functional outcome when compared with either insensate patients who underwent amputation or a matched control group of sensate patients with similar injuries. All but one patient in the salvage group had return of some sensation at 2-year follow up and the authors concluded that an insensate plantar foot at presentation should not be included in the algorithm for amputation.
Mackenzie and Bosse reviewed the results of the LEAP study with particular emphasis on the social and economic variables that influence outcomes in severe lower extremity. The authors note that 19% of patients screened positive for severe depression. The presence of anxiety, pain and depression at 3 months post-injury were significant predictors of poor outcome
Incorrect Answers:
tissue for type IIIB tibia fractures. Answer 5: The number of debridements has not been shown to influence outcome.
Question 91:
A displaced pediatric supracondylar humerus fracture is treated with closed manipulation and placement of 2 Kirschner wires placed from the lateral side. What would be the effect of adding a third pin from the lateral side? Review Topic
Options:
- Increase risk for iatrogenic ulnar nerve injury
- Provide more construct stiffness than adding a medial pin
- Improve construct stiffness in the presence of medial column comminution
- Will not affect construct stiffness in the presence of residual distal fragment internal rotation
Correct Answer: Improve construct stiffness in the presence of medial column comminution
Explanation:
Multiple biomechanical studies have shown that the addition of a third pin from the lateral side improves construct stiffness in the presence of medial column loss or slight internal rotation of the distal fragment. The same studies show that addition of a medial pin (cross pinning) has essentially the same benefit. Placement of a medial pin increases risk for iatrogenic nerve injury.
Question 92:
Figure 7 shows the radiograph of an otherwise healthy 65-year-old man who injured his right dominant shoulder while skiing 18 months ago. He did not seek treatment at the time of the injury. He now reports intermittent soreness when playing golf but has no other limitations. Examination reveals full range of motion and no tenderness, but he has slight pain with a crossed arm adduction stress test. He is neurologically intact. Initial management should consist of
Options:
- excision of the distal clavicle.
- open reduction and internal fixation with intramedullary partial threaded pins.
- open reduction and internal fixation with a reconstruction plate, screws, and bone grafting.
- bone grafting and use of heavy sutures to secure the clavicle to the coracoid.
- observation and nonsteroidal anti-inflammatory drugs.
Correct Answer: observation and nonsteroidal anti-inflammatory drugs.
Explanation:
DISCUSSION: The radiograph shows a displaced type II distal clavicle fracture with nonunion. Because the patient’s symptoms are minimal, the injury can be treated like a grade III acromioclavicular separation. Present management should consist of ice, anti-inflammatory drugs, activity modification, and perhaps physical therapy. If nonsurgical management fails to provide relief, the surgical options are varied with no uniformity in the literature regarding surgical treatment of this injury.
REFERENCES: Beaty JH (ed): Orthopaedic Knowledge Update 6. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999, pp 271-286.
Craig EV: Fractures of the clavicle, in Rockwood CA Jr, Matsen FA III (eds): The Shoulder. Philadelphia, PA, WB Saunders, 1998, vol 1, pp 428-482.
Question 93:
It has been shown that bisphosphonate-based supportive therapy (pamidronate or zoledronate) reduces skeletal events (onset or progression of osteolytic lesions) both in patients with multiple myeloma and in cancer patients with bone metastasis. The use of biphosphonate therapy has been associated with
Options:
- increased medical complications of treatment.
- osteonecrosis of the jaw.
- improved long-term survival rates.
- anorexia.
- decreased quality of life measures.
Correct Answer: osteonecrosis of the jaw.
Explanation:
DISCUSSION: The use of bisphosphonates has been recently associated with the development of osteonecrosis of the jaw. Length of exposure seems to be the most important risk factor for this complication. The type of bisphosphonate may play a role and previous dental procedures may be a precipitating factor. Bisphosphonates are a class of therapeutic agents originally designed to treat loss of bone density (ie, alendronate). The primary mechanism of action of these drugs is inhibition of osteoclastic activity, and it has been shown that these drugs are useful in diseases with propensities toward osseous metastases. In particular, they are effective in diseases in which there is clear upregulation of osteoclastic or osteolytic activity, such as breast cancer and multiple myeloma, and have developed into a mainstay of treatment for individuals with these diseases. Although shown to reduce skeletal events, there has been no improvement in patient survival.
REFERENCES: Bamias A, Kastritis E, Bamia C, et al: Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J Clin Oncol 2005;23:8580-8587.
Thakkar SG, Isada C, Smith J, et al: Jaw complications associated with bisphosphonate use in patients with plasma cell dyscrasias. Med Oncol 2006;23:51-56.
Van Poznak C: The phenomenon of osteonecrosis of the jaw in patients with metastatic breast cancer. Cancer Invest 2006;24:110-112.
Question 94:
- A 47-year-old woman who reports mild, aching pain in her knee has no history of trauma. Examination of the knee is normal. Figure 23a shows the AP radiograph. A bone scan shows increased uptake at this site only. Figure 23b shows the CT scan, and Figure 23c shows the histology from the CT scan-guided needle biopsy. Treatment should include
Options:
- extended curettage and polymethylmethacrylate cementation
- extra-articular resection of the knee and an allograft arthrodesis
- wide resection of the proximal tibia and custom prosthetic replacement
- prophylactic internal fixation and postoperative irradiation
- excision of the lateral condyle and reconstruction with a hemicondylar allograft
Correct Answer: extended curettage and polymethylmethacrylate cementation
Explanation:
Patients with giant cell tumors typically present with local pain, swelling and tenderness. Radiographs usually reveal a lesion destructive of both medullary and cortical bone. The lesion is characterized by an expanding zone of radiolucency that is located eccentrically in the end of a long bone in an adult.
The modern technique for the removal of a giant cell tumor involves wide decortication of all the bone overlying the area of the tumor. The cavity is filled with methylmethacrylate bone cement and covered with demineralized bone matrix to stimulate the restoration of strong cortical
boundaries. The other procedures are much more invasive and not necessary to treat a low-grade neo-plastic lesion such as a giant cell tumor. Fewer complications and better functional results have been found after intralesional excision and insertion of methylmethacrylate than other techniques.
Question 95:
The most common mechanism of injury to the triangular fibrocartilage complex (TFCC) involves
Options:
- wrist extension and forearm pronation.
- wrist extension and forearm supination.
- wrist flexion and forearm pronation.
- wrist flexion and forearm supination.
- axial load in ulnar deviation.
Correct Answer: wrist extension and forearm pronation.
Explanation:
DISCUSSION: TFCC tears are common in athletes. As the athlete braces for a fall, the wrist is most commonly in an extended position and the forearm is pronated.
REFERENCES: Cohen MS: Ligamentous injuries of the wrist in the athlete. Clin Sports Med 1998;17:533-552.
Rettig AC: Elbow, forearm and wrist injuries in the athlete. Sports Med 1998;25:115-130.
Question 96:
Which of the following amputations will lead to the greatest oxygen requirement per meter walked following prosthesis fitting?
Options:
- Above-knee-amputation (transfemoral)
- Below-knee-amputation (transtibial)
- Through Knee
- Syme
- Midfoot
Correct Answer: Above-knee-amputation (transfemoral)
Explanation:
DISCUSSION: The general trend is increasing energy requirement for more proximal amputations. Amputation should be performed at the lowest possible level in order to preserve the most function. Pinzur compared 5 patients with amputations at midfoot, Syme’s, BKA, through knee, and AKA with five controls. Walking speed and cadence decreased while oxygen consumption per meter walked increased with each more proximal amputation. The only exception is the Syme which was the most energy efficient even though it is more proximal to the midfoot amputation.
Question 97:
Figures 122a and 122b are the radiographs of a 79-year-old woman with a 2-year history of progressively worsening right hip pain. She had a right total hip arthroplasty 7 years prior. An infection workup is negative. She opts for revision surgery; the most appropriate surgical plan to address her femoral component is
Options:
- extended trochanteric osteotomy and revision to a cementless long-stem prosthesis.
- extended trochanteric osteotomy and revision to a cemented long-stem prosthesis.
- revision to a cementless long-stem prosthesis without use of an extended trochanteric osteotomy.
- revision to a cemented long-stem prosthesis without use of an extended trochanteric osteotomy.
Correct Answer: extended trochanteric osteotomy and revision to a cementless long-stem prosthesis.
Explanation:
DISCUSSION
The patient’s radiographs show loosening of the cemented femoral stem and varus remodeling of the femur. An extended trochanteric osteotomy is necessary because attempting to extract the existing prosthesis and implant another prosthesis without an osteotomy is likely to cause a proximal femoral fracture. Also, an osteotomy would facilitate atraumatic removal of the stem and cement. Cementless fixation is likely to produce a more predictable long-term outcome than cemented fixation for the revision implant.
Question 98:
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with Review Topic
Options:
- an avulsion of the lesser tuberosity.
- a midsubstance tear of the capsule.
- a tear of the anterior inferior labrum.
- a tear of the subscapularis.
- a tear of the humeral insertion of the inferior glenohumeral ligament.
Correct Answer: a tear of the humeral insertion of the inferior glenohumeral ligament.
Explanation:
An isolated avulsion of the lesser tuberosity occurs very rarely and usually is found in 12- and 13-year-old adolescents. The MRI scans reveal a tear of the humeral attachment of the inferior glenohumeral ligament, a so-called HAGL lesion. This injury to the inferior glenohumeral ligament occurs much less commonly than the classic Bankart lesion (anterior inferior labral tear). A tear of the subscapularis occurs with a similar mechanism of injury but generally occurs in older individuals.
Question 99:
A 25-year-old woman sustains a fall on an outstretched hand. She complains of elbow pain. Examination reveals tenderness over the lateral elbow and pain on elbow motion. Injury radiographs and CT scans are shown in Figures A and B, respectively. What is the next best step?
Options:
- Splint until swelling subsides, then long-arm cast
- Excision of fracture fragments
- Closed reduction and percutaneous pinning
- Open reduction and internal fixation (ORIF)
- Radial head replacement
Correct Answer: Closed reduction and percutaneous pinning
Explanation:
This patient has Mason II radial head fracture. ORIF will give the best results.
Non-/minimally displaced radial head fractures without a block to rotation can be managed nonoperatively. Complete articular fractures with >=3 fragments do better with radial head replacement. Indications for ORIF include large articular surface fragments, > 2 mm of displacement, mechanical block to forearm rotation, or associated fractures or ligament injuries requiring surgery.
Pike et al. retrospectively compared patients undergoing ORIF for isolated radial head fractures with radial fractures associated with other fractures/dislocations. They found no differences in pain/disability and complications or secondary capsular release between groups.
Yoon et al. retrospectively compared isolated partial articular displaced (2-5mm) radial head fractures treated nonoperatively vs ORIF. They found no clinical benefit with ORIF compared to non-operative management. The ORIF group had more complications. Younger patient age and larger fracture displacement favored operative intervention. Younger patients fared worse.
Figures A and B are radiographs and 3D reformatted CT images showing a displaced partial articular radial head fracture.
Incorrect Answers:
>= 3 fragments.
Question 100:
A 51-year-old woman with shoulder pain responds transiently to a subacromial injection and physical therapy exercise program. When her symptoms recur, an arthroscopic subacromial decompression is recommended. During the surgery, a partial-thickness articular-sided supraspinatus tear is noted. The supraspinatus footprint is exposed for 3 mm from the articular margin. The remaining intra-articular structures are normal. Inspection from the bursal surface reveals the tendon to be intact. What is the most appropriate course of management? Review Topic
Options:
- Completion of the tear from the bursal surface and rotator cuff repair
- Arthroscopic long head biceps tenotomy
- Arthroscopic glenohumeral synovectomy
- Arthroscopic tendon debridement and subacromial decompression
- Transtendinous rotator cuff repair
Correct Answer: Arthroscopic tendon debridement and subacromial decompression
Explanation:
The patient has a partial articular supraspinatus tendon avulsion (PASTA) lesion. Outcome studies suggest that articular-sided tears of this magnitude do well with arthroscopic decompression and debridement alone. Determination of lesion thickness is important in recommending treatment, and may be done with a variety of methods. Tears that involve exposure of less than 5 mm of the rotator cuff footprint likely measure less than half of the tendon thickness. In the absence of other associated pathology, bicipital tenotomy or synovectomy would be unnecessary. Completion of the tear or transtendinous repair would be considered for lesions of greater than 50% thickness.