DEFINITION
Trigger finger is an entrapment of the digital flexor tendon(s) by the flexor tendon sheath.Trigger finger progressively causes inflammation, pain, catching, locking, and reduced range of motion (ROM).
ANATOMY
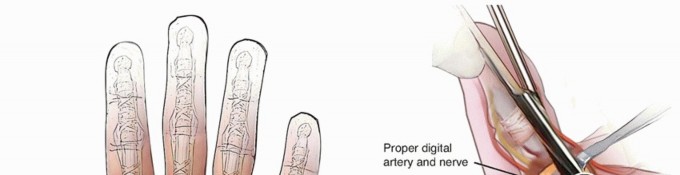
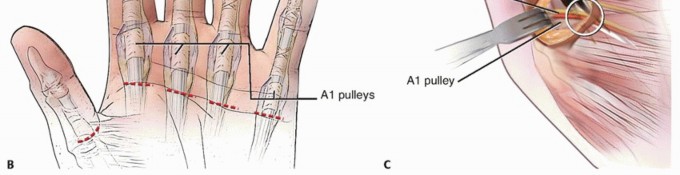
The flexor digitorum profundus and superficialis (flexor pollicis longus in the thumb) pass under (dorsal to) the flexor sheath, which consists of annular and cruciate pulleys.The A1 pulley, which is volar to the metacarpophalangeal (MCP) joint, is the most proximal pulley (except for athickening known as thepalmar aponeurotic pulley7) and is almost always the primary site of entrapment (FIG 1).
PATHOGENESIS
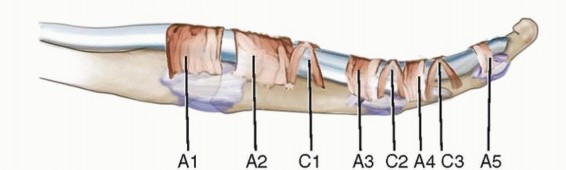
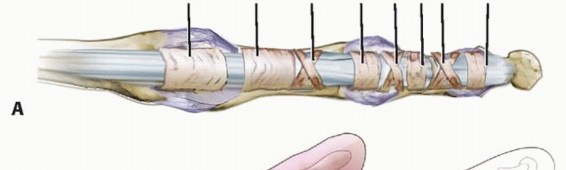
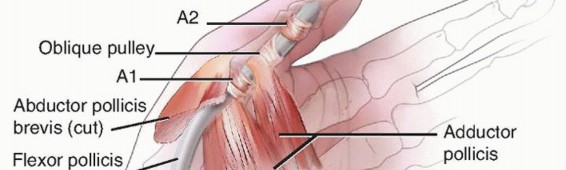

FIG 1 • To understand trigger finger and its release, an appreciation of the flexor tendon pulley system of the finger (A) and thumb (B) is required. This size mismatch causes hypertrophy (thickening) of the A1 pulley and tendinous swelling.These changes exacerbate the size discrepancy, setting up a cycle in which entrapment causes hypertrophy and hypertrophy causes entrapment.
NATURAL HISTORY
Trigger digits may develop spontaneously or may occur after swelling, from either trauma or a period of heavy use.Trigger digits may:Resolve spontaneously (especially in mild cases) Persist with the same level of symptomsAdvance to passively correctable lockingBecome indefinitely locked in either flexion or extension
PATIENT HISTORY AND PHYSICAL FINDINGS

FIG 2 • Reduced flexion caused by ring finger triggering. P.801Previous treatments for trigger finger and the extent and duration of the resultWhether the condition began after a particular incident or period of increased hand useThe patient's medical history should be evaluated for conditions that may cause trigger fingers and alter treatment as well as commonly associated conditions, including the following:DiabetesRheumatoid arthritis and other inflammatory arthropathiesAmyloidosis, most commonly secondary to renal disease requiring dialysis Lysosomal storage diseasesCarpal tunnel syndrome (often seen in patients with trigger finger but not causally related)The history and physical examination should exclude other conditions that cause overlapping symptoms, including the following:Nerve compression Muscle weaknessTendon interruption from laceration (partial or complete) or rupture Pulley rupture and bowstringingJoint or soft tissue contracture or swelling or bothExtensor tendon laceration or subluxation, especially at the MCP joint Joint dislocationMCP joint collateral ligament injuryThe physical examination should include the following:ROM test, which is the most objective measure of severity. If the patient has absolutely no active motion at the PIP (or thumb interphalangeal [IP]), consider tendon interruption.Palpation of the palm. If the A1 pulley is not tender, strongly consider other diagnoses. Examine for other causes of the patient's symptoms, including Dupuytren contracture, tendon sheath ganglion, PIP joint injury, and A3 pulley triggering.Examination of the extensor apparatus. Rule out extensor mechanism abnormalities and stress test the collateral ligaments of the MCP joint (radially and ulnarly) to rule out conditions that may cause overlapping signs or symptoms, including a popping sensation with ROM.Examination of the collateral ligaments at the MCP joint. Stress the collateral ligaments radially and ulnarly.Perform a neurovascular examination. Carpal tunnel syndrome often is associated with trigger finger. Muscle weakness may cause similar findings. Any neurovascular deficit should be documented before treatment.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Radiographs can exclude some unusual causes of trigger finger symptoms and can assess for arthritis but are not required to make the diagnosis of trigger finger.Ultrasound/dynamic ultrasound has been increasingly useful in confirmation of diagnosis and in guiding corticosteroid therapy for trigger finger.9If other pathology is suspected, magnetic resonance imaging (MRI) can be useful.Nerve conduction studies can evaluate for anterior interosseous nerve (AIN) compression, which may mimic a trigger thumb or concomitant carpal tunnel syndrome.
DIFFERENTIAL DIAGNOSIS
Extensor tendon subluxation at the MCP jointJoint contracture or injury, including MCP locking due to collateral ligaments and a swollen PIP jointSoft tissue swelling or contracture, including Dupuytren contracture Partial tendon lacerationTriggering at the A3 pulley (rare)Muscle weakness, including flexor pollicis longus weakness secondary to AIN palsy Masses (especially tendon sheath ganglions), which may cause A1 pulley tenderness
NONOPERATIVE MANAGEMENT
Observation and splintingMild, early cases often resolve spontaneously or do not bother the patient significantly. Use of a night extension splint may help minimize morning locking.Unless the PIP joint remains locked, in either flexion or extension, for several weeks, delayed treatment usually does not significantly change either the options available or their results.InjectionLong-term relief in most affected digits with one to three injections2Results in diabetic patients are not as good,1,4 but it still is worth trying. The patient should be warned that there glucose level may temporarily go up.Injection technique (FIG 3)One milliliter of 2% plain (no epinephrine) lidocaine and 1 mL of a soluble corticosteroid solution (eg, betamethasone or dexamethasone) in a single syringe with a 25-gauge needle is given.The A1 pulley area is prepped with an antiseptic solution such as alcohol or Betadine. A topical spray may be used to reduce discomfort.One to 2 mL is injected in the sheath or subcutaneously around the A1 pulley.13 Avoid injecting into the tendon itself; if increased resistance is encountered, this may be the cause.Ultrasound guidance may provide increased accuracy and avoid possible complications especially in the thumb.9
SURGICAL MANAGEMENT
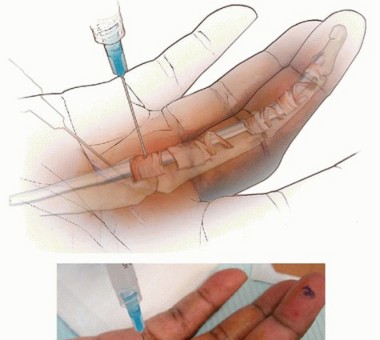
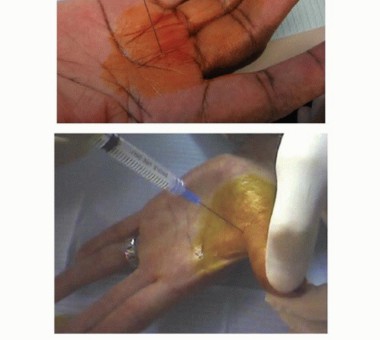
FIG 3 • Technique for trigger digit injection.
PREOPERATIVE PLANNING
Clinical notes and any studies obtained preoperatively should be reviewed.If procedures beyond an A1 pulley release are considered likely to be necessary (eg, possible resection of the ulnar slip of the flexor digitorum superficialis [FDS]), they should be discussed with the patient preoperatively.
POSITIONING
The patient is supine.The extremity is positioned so that the palm is facing up on a hand table.For index, middle, ring, and small digits, a hand holder (eg, a “lead hand”) may be helpful.For the thumb, it is more useful for the surgeon and assistant to position the hand and thumb throughout the procedure or to use a specialized thumb holder.Place a padded tourniquet and inflate it just before making the incision.
APPROACH
Anesthesia is obtained by injecting 2% plain (no epinephrine) lidocaine subcutaneously around the incision and in the tendon sheath.Sedation will mitigate the discomfort associated with the injection and the tourniquet. If sedation is used, the patient should be allowed to wake up in time to demonstrate complete active digital flexion and extension without locking, documenting successful pulley release.A standard volar approach to the A1 pulley is made with either an oblique Bruner-type, transverse, or longitudinal incision.For resection of the ulnar slip of the sublimis, a Bruner-type or midaxial longitudinal incision is used over the distal portion of the proximal phalanx.
TECHNIQUES
Open A1 Pulley Release
OPEN A1 PULLEY RELEASE
INCISION AND EXPOSURE


TECH FIG 1 • A. A longitudinal incision for ring finger A1 release. Index finger demonstrates a well-healed longitudinal incision without any contracture.(continued)



TECH FIG 2 • A. The digital neurovascular structures are retracted, and the A1 pulley has been cleared of all overlying soft tissue. B. The A1 pulley has been completely released. C. The palmar pulley remaining after A1 release. D. The flexor tendons are bluntly separated and pulled out of the wound, which then flexes the digit. (A-D: Top is proximal.)
PERFORMING THE RELEASE


TECH FIG 3 • A. Tenosynovium between the tendons can be gently removed. B. A tendon sheath mass. Pathologic analysis confirmed it was a tendon sheath ganglion. C,D. Full active extension and flexion after release.
COMPLETION

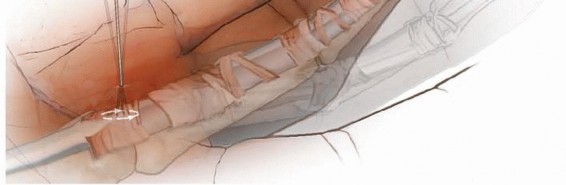
TECH FIG 4 • Percutaneous A1 release.

TECH FIG 5 • A Bruner-type incision. (Courtesy of Dominique Le Viet.) Distal to Proximal Ulnar Slip Excision Just distal to the A2 pulley, incise the tendon sheath, creating a radially based flap. This flap may be repaired later with 6-0 Prolene if desired.With the PIP joint maximally flexed, isolate and cut the ulnar slip of the FDS distally, taking care to preserve the vinculum brevis.Pull the tendon into the proximal wound and cut it as far proximal as can be reached safely. Confirm that the tendons now pass smoothly under the pulley system through a complete ROM. Release the tourniquet. Irrigate the wounds.Obtain hemostasis, usually with manual compression. Reinspect the wound, check for any arterial bleeding, and confirm the finger has brisk capillary refill.Close the skin with interrupted sutures and place a mildly compressive dressing. Proximal to Distal Ulnar Slip Excision
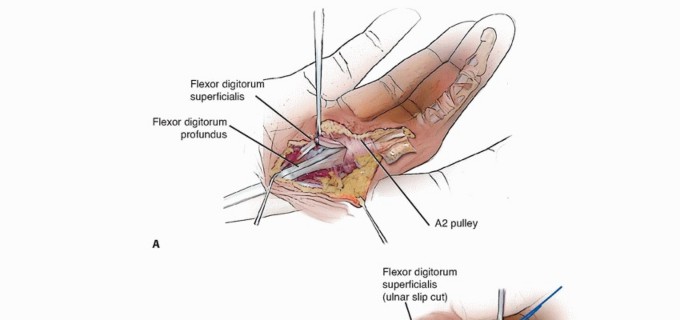
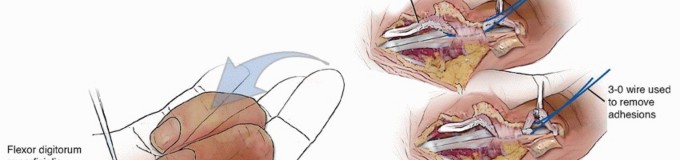
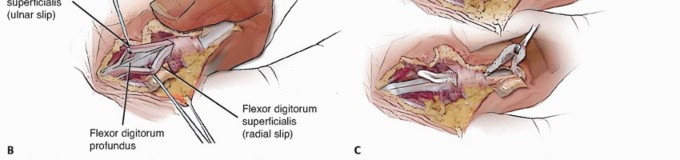
TECH FIG 6 • Open A1 pulley release with FDS ulnar slip excision. A. Enlargement of tendon proximal to A2 pulley (after A1 release). B. Separating the FDS tendon slips. C. Use of a wire loop to separate tendon adhesions after cutting the FDS tendon proximally. (A,B: Modified from Le Viet D, Tsionos I, Boulouednine M, et al. Trigger finger treatment by ulnar superficialis slip resection [U.S.S.R.]. J Hand Surg Br 2004:29[4]:368-373.)
PEARLS AND PITFALLS

FIG 4 • A soft dressing is applied with all the digits free.
POSTOPERATIVE CARE
A soft dressing is applied with all of the digits free (FIG 4). Active ROM as tolerated is encouraged. Minimize dressing bulk to avoid inhibiting motion.Formal therapy is required only if the patient has difficulty regaining ROM.Patients whose digits were locked preoperatively are more likely to need therapy. This may be started within the first week.Scar massage is encouraged after the wound is sealed.
OUTCOMES
Surgical release of trigger digits has a high success rate with a low complication and recurrence rate.3,14
COMPLICATIONS
Injury to digital nerve or artery BowstringingWound infection or dehiscence resulting in a flexor sheath infection Postoperative stiffnessIncomplete release Recurrence Incisional tenderness
REFERENCES
- Baumgarten KM, Gerlach D, Boyer MI. Corticosteroid injection in diabetic patients with trigger finger. A prospective, randomized, controlled double-blinded study. J Bone Joint Surg Am 2007;89(12):2604-2611.
- Benson LS, Ptaszek AJ. Injection versus surgery in the treatment of trigger finger. J Hand Surg Am 1997;22:138-144.
- Gilberts EC, Wereldsma JC. Long-term results of percutaneous and open surgery for trigger fingers and thumbs. Int Surg 2002;87:48-52.
- Griggs SM, Weiss AC, Lane LB, et al. Treatment of trigger finger in patients with diabetes mellitus. J Hand Surg Am 1995;20:787-789.
- Husain SN, Clarke SE, Buterbaugh GA, et al. Recalcitrant trigger finger managed with flexor digitorum superficialis resection. Am J Orthop 2011;40(12):620-624.
- Le Viet D, Tsionos I, Boulouednine M, et al. Trigger finger treatment by ulnar superficialis slip resection (U.S.S.R.). J Hand Surg Br 2004; 29:368-373.
- Manske PR, Lesker PA. Palmar aponeurosis pulley. J Hand Surg Am 1983;8:259-263.
- Marcus AM, Culver JE Jr, Hunt TR III. Treating trigger finger in diabetics using excision of the ulnar slip of the flexor digitorum superficialis with or without A1 pulley release. Hand 2007;2: 227-231.
- Mardani Kivi M, Lahiji FA, Jandaghi AB, et al. Efficacy of sonographically guided intra-flexoral sheath corticosteroid injection in the treatment of trigger thumb. Acta Orthop Traumatol Turc 2012;46(5):346-352.
- Rayan GM. Distal stenosing tenosynovitis. J Hand Surg Am 1990; 15:973-975.
- Ryzewicz M, Wolf JM. Trigger digits: principles, management, and complications. J Hand Surg Am 2006;31:135-146.
- Seradge H, Kleinert HE. Reduction flexor tenoplasty. J Hand Surg Am 1981;6:543-544.
- Taras JS, Raphael JS, Pan WT, et al. Corticosteroid injections for trigger digits: is intrasheath injection necessary? J Hand Surg Am 1998;23:717-722.
- Turowski GA, Zdankiewicz PD, Thomson JG. The results of surgical treatment of trigger finger. J Hand Surg Am 1997;22:145-149.
- Wilhelmi BJ, Mowlavi A, Neumeister MW, et al. Safe treatment of trigger finger with longitudinal and transverse landmarks: an anatomic study of the border finger for percutaneous release. Plast Reconstr Surg 2003;112:993-999.
- Wolfe SW. Tenosynovitis. In: Green DP, Hotchkiss RN, Pederson WC, et al, eds. Green's Operative Hand Surgery, ed 5. Philadelphia: Elsevier, 2005:2137-2158.
