Acute Knee Injury Case Study: Collegiate Athlete with ACL Rupture & Multiligamentous Damage
Key Takeaway
Diagnosing a complex ACL rupture, as seen in collegiate athletes, involves detailed clinical examination including Lachman and Pivot Shift tests, often revealing associated MCL sprains and meniscal tears. Imaging, particularly MRI, confirms complete ACL disruption, bone contusions, and specific findings like a Segond fracture or bucket-handle meniscal tears, guiding comprehensive treatment.
Patient Presentation and History
A 22-year-old collegiate male soccer player presented to the emergency department with acute right knee pain, swelling, and instability following a non-contact injury during a competitive match. The mechanism described was a sudden deceleration with a pivoting motion on a planted foot, followed by a valgus collapse of the knee. The patient reported hearing a distinct "pop" at the time of injury, experienced immediate severe pain, and was unable to bear weight or continue playing.
The mechanism of injury is highly characteristic of anterior cruciate ligament rupture. Non-contact pivoting injuries account for approximately seventy to eighty percent of all anterior cruciate ligament tears. The biomechanical cascade typically involves the athlete attempting to change direction rapidly. The foot becomes fixed to the playing surface, often exacerbated by the high coefficient of friction provided by modern cleats on artificial turf or firm natural grass. As the athlete decelerates and internally rotates the femur over a fixed, externally rotated tibia, a significant valgus moment is applied to the knee joint. This complex loading pattern overwhelms the tensile capacity of the anterior cruciate ligament, often resulting in mid-substance rupture or, less commonly, avulsion from the femoral or tibial footprint.
His past medical history was unremarkable, with no significant comorbidities. He was highly active, participating in competitive soccer at a Division I collegiate level, and had no prior history of knee injury or surgical intervention. He reported no allergies and was not taking any regular medications. Social history was negative for smoking, and he consumed alcohol occasionally. His primary goal was to return to elite-level competitive soccer, a factor that heavily influenced the subsequent surgical decision-making process.
The patient's demographic profile places him in a high-risk category for subsequent knee instability and secondary meniscal or chondral damage if left untreated. Young, highly active males participating in cutting and pivoting sports demonstrate the highest incidence of anterior cruciate ligament injuries. Furthermore, the presence of a concomitant medial collateral ligament injury and suspected meniscal pathology, often referred to as a variation of O'Donoghue's unhappy triad, complicates the clinical picture and necessitates a comprehensive, staged approach to both diagnosis and management.
Clinical Examination Findings
Upon initial examination in the emergency department, the patient was in moderate distress secondary to acute hemarthrosis and capsular distension.
Inspection and Palpation
The right knee demonstrated significant effusion, particularly prominent in the suprapatellar pouch. The rapidity of the effusion onset, occurring within hours of the injury, is highly indicative of a hemarthrosis, which in the context of acute knee trauma carries a seventy to ninety percent positive predictive value for an anterior cruciate ligament tear or an osteochondral fracture. Mild ecchymosis was noted laterally. The knee was held in approximately 15 degrees of flexion, representing the position of maximum capsular volume, with visible guarding against extension. No gross structural deformity was observed, reducing the likelihood of a high-energy knee dislocation, though spontaneous reduction of a subluxation event could not be excluded.
Diffuse tenderness was elicited over the medial and lateral joint lines, as well as along the anteromedial aspect of the knee overlying the superficial medial collateral ligament. A significant effusion was ballotable, and the joint felt warm to the touch. No focal tenderness over bony prominences suggested an acute fracture, though precise palpation of the lateral tibial plateau was necessary to assess for a potential Segond fracture, a pathognomonic radiographic sign of anterolateral capsular avulsion.
Range of Motion Assessment
Active range of motion was severely limited due to pain and intra-articular swelling, ranging from 15 degrees of flexion to approximately 90 degrees. Passive range of motion was similarly restricted. Attempts to achieve terminal extension resulted in a firm, painful endpoint. This limitation in extension can be attributed to several factors, including hamstring spasm, capsular distension from the hemarthrosis, or mechanical block secondary to an interposed meniscal fragment or the stump of the ruptured anterior cruciate ligament impinging within the intercondylar notch.
Ligamentous Stability Testing
Ligamentous evaluation was performed carefully to minimize patient discomfort while maximizing diagnostic yield.
- Lachman Test: Performed at 20 to 30 degrees of flexion to isolate the posterolateral bundle of the anterior cruciate ligament. This test was grossly positive (Grade III, greater than 10 millimeters of translation), demonstrating significant anterior tibial translation with a soft, indistinct end-point. The Lachman test remains the most sensitive clinical examination maneuver for acute anterior cruciate ligament rupture.
- Anterior Drawer Test: Positive, confirming anterior instability. However, this test is often less sensitive than the Lachman test in the acute setting due to the stabilizing effect of the posterior horn of the medial meniscus against the medial femoral condyle at 90 degrees of flexion, as well as secondary restraint provided by hamstring muscle guarding.
- Pivot Shift Test: Initially difficult to assess due to pain and muscle guarding. Following intra-articular local anesthetic instillation or examination under anesthesia, a definitive high-grade clunk was elicited during the reduction phase as the knee was brought from flexion to extension with valgus and internal rotation. This strongly suggested profound anterolateral rotatory instability and potential compromise of the anterolateral ligament complex.
- Posterior Drawer Test and Posterior Sag Sign: Negative, confirming an intact posterior cruciate ligament. The normal step-off of the medial tibial plateau relative to the medial femoral condyle was preserved.
- Varus Stress Test: Stable in full extension and at 30 degrees of flexion, indicating an intact lateral collateral ligament and posterolateral corner complex.
- Valgus Stress Test: Stable in full extension, indicating an intact posterior medial corner and posterior oblique ligament. However, mild gapping (3 to 5 millimeters) was observed at 30 degrees of flexion with a firm endpoint, suggesting a Grade I to II sprain of the superficial medial collateral ligament.
Meniscal and Patellofemoral Evaluation
- McMurray Test: Positive with a palpable and audible click during internal and external rotation, particularly with valgus stress and extension. This finding strongly suggested a medial meniscal tear, a common concomitant injury occurring in up to sixty percent of acute anterior cruciate ligament ruptures.
- Apley Grind Test: Produced pain and a click, further corroborating the suspicion of a meniscal lesion over isolated ligamentous sprain.
- Patellofemoral Joint: No evidence of patellar apprehension or instability. The patellar grind test was negative, and the extensor mechanism was intact, albeit inhibited by pain.
Neurological and Vascular Assessment
Distal sensation was intact in all major nerve distributions, including the saphenous, deep peroneal, superficial peroneal, sural, and tibial nerves. Motor function of the extensor hallucis longus, tibialis anterior, and gastrocnemius-soleus complex was normal (Grade 5/5).
Distal pulses, specifically the dorsalis pedis and posterior tibial arteries, were bounding and symmetric bilaterally. Capillary refill in the digits was less than two seconds. Given the high-energy nature of pivoting injuries, albeit non-contact, vigilance for vascular compromise is essential, particularly if there is suspicion of a transient knee dislocation. Ankle-brachial indices were not indicated given the normal symmetric pulses and absence of high-energy multiligamentous trauma involving the posterior cruciate ligament. Compartment compartments of the lower leg were soft and compressible, with no severe pain out of proportion or pain with passive stretch of the digits.
Imaging and Diagnostics
Accurate diagnosis and surgical planning rely heavily on a comprehensive imaging workup. The standard protocol for an acute knee injury of this magnitude involves initial plain radiography followed by advanced cross-sectional imaging.
Plain Radiography Findings
Standard weight-bearing (when tolerated) anteroposterior, lateral, notch (tunnel), and Merchant (skyline) views were obtained.
- Anteroposterior and Lateral Views: Demonstrated a significant joint effusion, evidenced by the displacement of the suprapatellar fat pad. No gross fractures of the distal femur, proximal tibia, or patella were identified. The joint space was preserved bilaterally, with no evidence of underlying osteoarthritic changes, consistent with the patient's age.
- Notch View: The intercondylar notch appeared normal in width. Narrow intercondylar notches have been implicated as an intrinsic anatomical risk factor for anterior cruciate ligament injury due to potential impingement of the ligament against the lateral femoral condyle during dynamic valgus loading.
- Lateral Capsular Sign: A careful review of the anteroposterior radiograph revealed a subtle, small elliptic avulsion fracture arising from the lateral aspect of the proximal tibia, just distal to the articular surface. This finding, known as a Segond fracture, represents an avulsion of the anterolateral capsule and anterolateral ligament. It is considered pathognomonic for an anterior cruciate ligament tear and indicates a higher degree of anterolateral rotatory instability.
Magnetic Resonance Imaging Evaluation
Magnetic resonance imaging without contrast is the gold standard for evaluating intra-articular knee pathology. Standard sequences included T1-weighted, T2-weighted, and proton density fat-suppressed images in the sagittal, coronal, and axial planes.
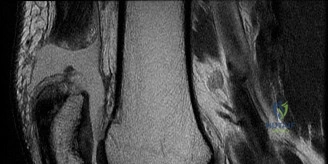
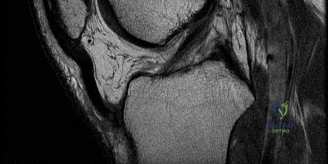
- Anterior Cruciate Ligament: Sagittal T2-weighted images demonstrated a complete discontinuity of the anterior cruciate ligament fibers. The ligament appeared edematous and amorphous, with the classic "empty notch sign" visible on coronal sequences. The proximal stump of the ligament was retracted and resting horizontally within the intercondylar notch.
- Bone Bruise Pattern: Characteristic osteochondral impaction injuries, or "bone bruises," were evident as areas of hyperintensity on T2 fat-suppressed images in the middle portion of the lateral femoral condyle and the posterior aspect of the lateral tibial plateau. This kiss-lesion pattern results from the anterior subluxation of the tibia and subsequent impaction of the lateral femoral condyle against the posterolateral tibial plateau during the pivot-shift mechanism. The presence of severe bone bruising correlates with higher initial pain levels and potential long-term chondral degradation.
- Meniscal Pathology: The coronal and sagittal sequences revealed a hyperintense linear signal extending to the articular surface in the posterior horn of the medial meniscus. The morphology was consistent with a longitudinal vertical tear located in the red-white zone (peripheral third), making it a highly suitable candidate for meniscal repair. The lateral meniscus appeared intact.
- Medial Collateral Ligament: Coronal T2 sequences showed periligamentous edema surrounding the superficial medial collateral ligament, primarily at its femoral origin, with some intra-substance signal but no complete discontinuity. This confirmed the clinical diagnosis of a Grade II medial collateral ligament sprain.
- Anterolateral Complex: Edema was noted in the anterolateral soft tissues, corresponding to the radiographic Segond fracture, confirming injury to the anterolateral capsular structures.
Differential Diagnosis
When evaluating acute hemarthrosis and instability following a non-contact knee injury, several distinct pathologies must be considered. The following table delineates the primary differential diagnoses, comparing their clinical presentations, imaging hallmarks, and management implications.
| Diagnostic Consideration | Key Clinical Findings | Imaging Hallmarks (MRI/X-ray) | Management Implications |
|---|---|---|---|
| Anterior Cruciate Ligament Rupture | Immediate swelling, audible "pop", positive Lachman, positive Pivot Shift, giving way. | Empty notch sign, fiber discontinuity, lateral compartment bone bruising, Segond fracture. | Operative reconstruction for young/active patients; pre-habilitation to restore ROM prior to surgery. |
| Acute Patellar Dislocation | Medial-sided pain (MPFL origin), positive patellar apprehension, large effusion, visible deformity if unreduced. | Lateral patellar tilt/subluxation, bone bruise on medial patellar facet and lateral femoral condyle, MPFL disruption. | Often non-operative initially with bracing and therapy; operative stabilization for recurrent instability or osteochondral loose bodies. |
| Isolated Meniscal Tear | Delayed swelling (over 24 hours), joint line tenderness, mechanical symptoms (catching, locking), positive McMurray. | Linear intrameniscal signal extending to articular surface. Morphology dictates repairability (e.g., bucket-handle). | Conservative for degenerative/stable tears; arthroscopic repair or partial meniscectomy for symptomatic/unstable tears. |
| Osteochondral Defect or Fracture | Acute sharp pain, hemarthrosis, focal tenderness, mechanical catching if loose body is present. | Focal chondral defect, subchondral bone marrow edema, potential intra-articular radiopaque/radiolucent loose body. | Dependent on lesion size and location; options include microfracture, OATS, or loose body removal/fixation. |
| Medial Collateral Ligament Rupture (Isolated) | Medial pain and swelling, localized tenderness over femoral/tibial attachments, valgus laxity. | Thickening, edema, or discontinuity of the MCL. Rarely associated with large intra-articular hemarthrosis unless capsular tear. | Primarily non-operative with hinged knee bracing; surgical repair/reconstruction reserved for chronic Grade III or multiligamentous injuries. |
Surgical Decision Making and Classification
The management of anterior cruciate ligament injuries must be highly individualized, taking into account the patient's age, baseline activity level, occupational demands, and the presence of concomitant intra-articular pathology.
Rationale for Operative Intervention
In this case, conservative management (physical therapy and bracing) was deemed inappropriate. The patient is a 22-year-old Division I collegiate soccer player. Elite soccer places extreme demands on the dynamic stability of the knee, requiring repetitive cutting, pivoting, and sudden deceleration. Literature clearly demonstrates that high-demand athletes with anterior cruciate ligament deficiency who attempt to return to sport without surgical stabilization experience a high rate of recurrent instability episodes. These recurrent subluxations lead to devastating secondary injuries, particularly non-recoverable meniscal tears and irreversible chondral damage, rapidly accelerating the onset of early post-traumatic osteoarthritis.
Furthermore, the presence of a repairable longitudinal tear in the posterior horn of the medial meniscus strongly pushes the indication toward early operative intervention. The anterior cruciate ligament and the medial meniscus act synergistically. The posterior horn of the medial meniscus is a critical secondary restraint to anterior tibial translation. Reconstructing the anterior cruciate ligament protects the meniscal repair from excessive shear forces, while repairing the meniscus protects the anterior cruciate ligament graft from excessive load-to-failure stress.
Timing of Surgery
The timing of the surgical intervention is a critical variable in optimizing outcomes and minimizing complications, specifically arthrofibrosis. Historically, acute reconstruction within the first few days of injury was associated with a high incidence of postoperative joint stiffness. Current evidence-based protocols advocate for a period of "pre-habilitation."
The patient was placed in a hinged knee brace and initiated on a strict physical therapy regimen aimed at resolving the acute effusion, restoring normal gait mechanics, and achieving full, symmetric range of motion, particularly terminal extension. Surgery was scheduled for four weeks post-injury, at which point his knee was quiet, the effusion had resolved, and he had regained full extension and 125 degrees of flexion. The concomitant Grade II medial collateral ligament sprain was managed non-operatively during this waiting period. Grade I and II medial collateral ligament injuries have excellent healing potential with bracing and rarely require surgical intervention, even in the setting of anterior cruciate ligament reconstruction.
Graft Selection
Graft selection remains one of the most debated topics in orthopedic sports medicine. The primary options include bone-patellar tendon-bone (BTB) autograft, hamstring tendon autograft (semitendinosus and gracilis), quadriceps tendon autograft, and various allografts.
For a young, elite collegiate soccer player, allograft tissue is generally contraindicated due to significantly higher failure rates (up to three to four times higher) compared to autografts in the under-25 demographic, likely due to delayed graft incorporation and sterilization-induced structural alterations.
The decision was made to proceed with a Bone-Patellar Tendon-Bone (BTB) autograft. The BTB autograft is often considered the gold standard for high-demand cutting athletes. Its primary biomechanical advantage lies in the rigid bone-to-bone healing within the femoral and tibial tunnels, which allows for faster incorporation (typically 6 to 8 weeks) compared to soft tissue healing (10 to 12 weeks). Furthermore, the structural properties of the central third of the patellar tendon closely match those of the native anterior cruciate ligament. While hamstring autografts offer a less morbid harvest site and less anterior knee pain, they have been associated with a slightly higher rate of graft elongation and residual laxity in elite athletes. The quadriceps tendon is an excellent alternative gaining popularity, but BTB was selected based on the surgeon's experience and the robust, predictable outcome profile in elite soccer demographics.
Consideration of Lateral Extra-articular Tenodesis
Given the presence of a high-grade pivot shift and a radiographic Segond fracture indicating anterolateral complex injury, the addition of a Lateral Extra-articular Tenodesis (LET) or Anterolateral Ligament (ALL) reconstruction was strongly considered. Recent biomechanical and clinical outcome studies, including the STABILITY trial, have demonstrated that adding a LET to a primary anterior cruciate ligament reconstruction in young, high-risk patients significantly reduces the risk of graft rupture and persistent rotatory laxity. The decision was made to perform a modified Lemaire lateral extra-articular tenodesis utilizing a strip of the iliotibial band to augment the intra-articular reconstruction.
Surgical Technique and Intervention
The patient was brought to the operating room and placed in the supine position on the operating table. General endotracheal anesthesia was administered. A thorough examination under anesthesia (EUA) was performed, confirming the Grade III Lachman, high-grade pivot shift, and stable medial and lateral collateral ligaments in extension.
Patient Positioning and Preparation
A high thigh tourniquet was applied to the operative limb. The non-operative limb was placed in a well-leg holder. The operative leg was positioned in a standard leg holder allowing for full range of motion from hyperextension to 120 degrees of flexion. The limb was prepped and draped in standard sterile orthopedic fashion. Esmarch bandage was used for exsanguination, and the tourniquet was inflated to 250 mmHg.
Diagnostic Arthroscopy and Meniscal Management
Standard anterolateral and anteromedial portals were established. A diagnostic arthroscopic sweep was performed.
The anterior cruciate ligament was confirmed to be completely avulsed from the femoral footprint, with the stump lying in the intercondylar notch. The articular cartilage of the patellofemoral joint and medial compartment was pristine. The lateral compartment demonstrated the expected Grade II chondral impaction injury on the lateral femoral condyle.
Attention was turned to the medial meniscus. Probing confirmed a 1.5-centimeter longitudinal vertical tear in the posterior horn, situated in the vascularized red-white zone. The tear was unstable, easily displacing anteriorly into the joint space. An all-inside meniscal repair technique was selected. The meniscal edges and the adjacent synovium were aggressively rasped using an arthroscopic rasp and shaver to stimulate a bleeding bed and promote a healing response. Two all-inside meniscal repair devices (suture anchors) were deployed sequentially, capturing the superior and inferior leaflets of the meniscus and reducing the tear anatomically. Excellent compression and stability were achieved.
Graft Harvest and Preparation
Attention was directed to the anterior knee. A 5-centimeter longitudinal incision was made midline over the patellar tendon, extending from the inferior pole of the patella to the tibial tubercle. Full-thickness flaps were developed. The paratenon was incised longitudinally and preserved for later closure.
Using a double-bladed scalpel, the central 10 millimeters of the patellar tendon was demarcated. An oscillating saw and osteotomes were used to harvest a 20-millimeter bone block from the patella and a 25-millimeter bone block from the tibial tubercle. The graft was taken to the back table. The bone blocks were trimmed to easily pass through a 10-millimeter sizing cylinder. Drill holes were placed in both bone blocks, and passing sutures (Number 5 non-absorbable) were placed. The graft was wrapped in a saline-soaked sponge.
Tunnel Preparation
The principles of anatomic anterior cruciate ligament reconstruction dictate that the tunnels must be placed within the native anatomical footprints to restore normal kinematics.
- Femoral Tunnel: The intercondylar notch was debrided to visualize the native femoral footprint, specifically the lateral bifurcate ridge and the lateral intercondylar ridge (resident's ridge). To achieve independent and anatomic femoral tunnel placement, an accessory anteromedial portal was utilized. The knee was hyperflexed to 120 degrees. A guide pin was placed in the center of the native footprint on the medial wall of the lateral femoral condyle. A 10-millimeter reamer was used to drill the femoral socket to a depth of 25 millimeters.
- Tibial Tunnel: A tibial drill guide was introduced through the anteromedial portal and set at 55 degrees. The tip was placed in the center of the native tibial footprint, slightly medial to the anterior horn of the lateral meniscus and anterior to the posterior cruciate ligament. A guide pin was drilled from the anteromedial tibia into the joint. A 10-millimeter reamer was used to create the tibial tunnel over the guide pin. The intra-articular apertures of both tunnels were carefully chamfered to prevent graft abrasion.
Graft Passage and Fixation
The BTB graft was passed through the tibial tunnel and into the femoral socket using the passing sutures. The femoral bone block was visualized arthroscopically to ensure flush seating within the socket.
- Femoral Fixation: With the knee in hyperflexion, a guidewire was passed through the accessory anteromedial portal alongside the femoral bone block. A 7-millimeter by 20-millimeter titanium interference screw was advanced over the wire, providing rigid aperture fixation.
- Tibial Fixation: The knee was taken through a full range of motion to cycle the graft and eliminate creep. With the knee positioned at 20 degrees of flexion and a posterior drawer force applied to restore the normal tibiofemoral step-off, maximum manual tension was applied to the tibial bone block. An 8-millimeter by 25-millimeter titanium interference screw was inserted into the tibial tunnel, securing the graft.
Arthroscopic evaluation confirmed excellent graft tension, no impingement in the notch during full extension, and complete restoration of anterior stability.
Lateral Extra-articular Tenodesis (LET)
Following intra-articular fixation, the lateral aspect of the knee was addressed. A 4-centimeter incision was made centered over the lateral epicondyle. The iliotibial band was exposed. A 1-centimeter wide by 8-centimeter long strip of the posterior third of the iliotibial band was harvested, leaving its distal attachment at Gerdy's tubercle intact. The proximal end was whipstitched.
The femoral attachment site was identified slightly proximal and posterior to the lateral epicondyle. A guide pin was placed, and a small socket was drilled. The iliotibial band strip was passed deep to the fibular collateral ligament. With the knee held in 30 degrees of flexion and neutral rotation, the graft was tensioned and secured into the femoral socket using a 6-millimeter bioabsorbable interference screw.
Closure
The wounds were copiously irrigated with sterile saline. The patellar tendon defect was loosely approximated, and the paratenon was meticulously closed to minimize adhesions. The subcutaneous tissues and skin were closed in layers. Sterile dressings and a hinged knee brace locked in extension were applied. The tourniquet was deflated, and the patient was extubated without complication.
Post Operative Protocol and Rehabilitation
The rehabilitation following a combined anterior cruciate ligament reconstruction, meniscal repair, and lateral extra-articular tenodesis is complex and requires strict adherence to biological healing timelines. The presence of the meniscal repair dictates the initial weight-bearing and range of motion restrictions.
Phase I: Protection and Early Range of Motion (Weeks 0 to 4)
The primary goals in the immediate postoperative phase are to control inflammation, protect the graft and meniscal repair, and restore terminal extension.
* Weight Bearing: Due to the all-inside repair of the posterior horn of the medial meniscus, weight-bearing was restricted. The patient was allowed touch-down weight-bearing with crutches with the brace locked in full extension.
* Bracing: The hinged knee brace remained locked in extension for ambulation and sleeping to prevent flexion contractures.
* Range of Motion: Passive and active-assisted range of motion was initiated early but restricted to 0 to 90 degrees for the first four weeks to prevent excessive shear stress on the healing meniscus. Prone hangs and heel props were emphasized to achieve symmetrical hyperextension.
* Muscle Activation: Quadriceps re-education is critical. Modalities such as neuromuscular electrical stimulation (NMES) were utilized alongside isometric quadriceps sets and straight leg raises.
Phase II: Progressive Weight Bearing and Strengthening (Weeks 4 to 8)
As the meniscal repair begins to heal, restrictions are gradually lifted.
* Weight Bearing: Progression to full weight-bearing as tolerated, weaning off crutches once normal gait mechanics were achieved without an extensor lag.
* Bracing: The brace was unlocked for ambulation and eventually discontinued by week 6 once adequate quadriceps control was demonstrated.
* Range of Motion: Progression to full, symmetric range of motion.
* Strengthening: Closed kinetic chain exercises (mini-squats, leg press) were initiated. Open kinetic chain knee extension was restricted to the 90 to 40-degree arc to minimize anterior shear forces on the healing BTB graft.
Phase III: Advanced Strengthening and Proprioception (Weeks 8 to 16)
This phase focuses on hypertrophy and neuromuscular control.
* Strengthening: Progression of unilateral closed kinetic chain exercises (Bulgarian split squats,
