
锁骨骨折MIPO微创技术:专家解析与技术要点
Introduction & Epidemiology
Clavicle fractures are among the most common skeletal injuries, accounting for approximately 2.6% to 10% of all fractures and up to 45% of shoulder girdle injuries. The vast majority, roughly 80% as noted in the seminal content, occur in the midshaft, a region also known as the diaphyseal segment. Historically, conservative management, primarily with sling immobilization, was the mainstay for most clavicle fractures, with operative intervention reserved for specific indications such as open fractures, neurovascular compromise, or floating shoulder. This approach, while avoiding surgical risks, often resulted in malunion, shortening, and residual cosmetic deformity, particularly in displaced adult fractures. For pediatric populations, especially those under 14 years of age, robust remodeling potential typically favors conservative treatment, as also highlighted in the seed content.
However, the understanding of functional deficits associated with significant malunion (e.g., shortening >2 cm, displacement >100%) and the increasing demand for faster return to function and improved cosmetic outcomes have led to a paradigm shift towards more frequent operative intervention for displaced adult clavicle fractures. Traditional open reduction and internal fixation (ORIF) with plate and screw constructs, while providing excellent stability and predictable union rates, inherently involve a relatively long incision along the subcutaneous border of the clavicle. This often leads to prominent scarring and a high incidence of iatrogenic injury to the supraclavicular nerves, resulting in localized numbness or dysesthesia, which can be particularly bothersome for many patients, especially females.
The evolution of surgical techniques has introduced minimally invasive approaches to address these concerns. Minimally Invasive Plate Osteosynthesis (MIPO) for clavicle fractures, alongside techniques such as elastic intramedullary nailing, represents a significant advancement. MIPO aims to achieve fracture reduction and stable fixation through smaller incisions, preserving soft tissue integrity and periosteal blood supply, thereby promoting biological healing, reducing scar burden, and minimizing neurovascular complications compared to conventional ORIF. This detailed guide focuses on the technical aspects and clinical considerations of clavicle MIPO, providing a comprehensive reference for orthopedic surgeons.
Surgical Anatomy & Biomechanics
Successful clavicle fracture management, particularly with MIPO, necessitates a thorough understanding of its complex anatomy and biomechanical role.
Surgical Anatomy
The clavicle is an S-shaped long bone, acting as a strut that connects the upper limb to the axial skeleton. Its subcutaneous location makes it easily palpable but also susceptible to trauma and hardware prominence.
- Morphology: The medial two-thirds of the clavicle are convex anteriorly, while the lateral third is concave anteriorly. This S-shape is critical for biomechanical stability and articulation.
-
Neurovascular Structures:
This is paramount for MIPO to minimize iatrogenic injury.
- Superiorly: The supraclavicular nerves (medial, intermediate, and lateral branches of the cervical plexus) cross the clavicle's superior surface. These nerves provide sensation to the skin over the superior chest and shoulder. They are highly susceptible to injury during incision, soft tissue dissection, and tunneling, leading to numbness or painful neuroma. MIPO's smaller incisions and blunt tunneling aim to mitigate this risk.
- Posteriorly and Inferiorly: The subclavian artery and vein pass posterior and inferior to the clavicle, along with the brachial plexus. These vital structures are at risk during deep drilling, tunneling, or excessive manipulation, particularly in comminuted fractures with sharp fragments. The subclavius muscle, situated in the subclavian groove, offers some protection.
-
Muscular Attachments:
- Superior: Trapezius (lateral third), Sternocleidomastoid (medial third).
- Inferior: Subclavius (middle third), Pectoralis Major (medial half), Deltoid (lateral half).
- These muscles exert significant deforming forces on fracture fragments, influencing displacement and complicating reduction.
-
Ligaments:
- Medially: Sternoclavicular ligaments.
- Laterally: Acromioclavicular ligaments.
- Coracoclavicular Ligaments: Conoid (medial) and Trapezoid (lateral) ligaments connect the clavicle to the coracoid process of the scapula, providing crucial vertical stability for the lateral clavicle. Their integrity is vital, especially for lateral third fractures.
- Periosteum: The clavicle's periosteum provides significant blood supply for fracture healing. MIPO's principle of limited soft tissue dissection is designed to preserve this vital biological envelope, promoting superior healing capacity.
Biomechanics
The clavicle’s primary function is to maintain the length of the shoulder girdle, facilitating maximum arm range of motion, and protecting underlying neurovascular structures.
- Stress Distribution: The S-shape and robust cortical bone allow the clavicle to withstand significant axial, bending, and torsional stresses. Midshaft fractures are common due to this region being the narrowest and having an anatomical change in curvature.
- Fracture Displacement: Deforming forces from the sternocleidomastoid (pulling the medial fragment superiorly), pectoralis major, and deltoid (pulling the lateral fragment inferiorly and medially) typically result in superior displacement and shortening of midshaft fractures.
-
Fixation Principles:
- Relative Stability (MIPO): MIPO inherently promotes relative stability, allowing for callus formation and secondary bone healing. By avoiding extensive periosteal stripping, the biological environment for healing is maintained. This contrasts with absolute stability achieved by traditional open reduction and compression plating for simple fracture patterns.
-
Plate Positioning:
- Superior plating: Offers strong biomechanical fixation due to the clavicle's superior surface being a tension band. However, the plate is highly subcutaneous and prone to prominence and supraclavicular nerve irritation.
- Anterosuperior plating: Often preferred for MIPO. Placing the plate slightly anteriorly and superiorly, along the superior-anterior border, can reduce hardware prominence while providing adequate biomechanical stability. This position may require less aggressive subperiosteal tunneling compared to a purely superior position, potentially further reducing nerve irritation. The choice of pre-contoured locking plates facilitates effective fixation in this position.
MIPO leverages these biomechanical principles by achieving stable, yet not overly rigid, fixation that supports early mobilization while prioritizing biological healing through minimal tissue disruption.
Indications & Contraindications
The decision to proceed with operative fixation, and specifically MIPO, for clavicle fractures is multifactorial, balancing patient factors, fracture characteristics, and potential risks versus benefits.
Indications for Operative Treatment (including MIPO)
While conservative management remains appropriate for many non-displaced or minimally displaced fractures, operative fixation is indicated for:
- Significant Displacement: Transverse or oblique midshaft fractures with >1 shaft width displacement, or superior/inferior displacement >10 mm.
- Shortening: Clavicle shortening exceeding 1.5-2 cm, which can lead to scapular dyskinesis, altered shoulder mechanics, and functional deficits.
- Severe Comminution: Multifragmentary fractures where conservative treatment is highly likely to result in symptomatic malunion or nonunion.
- Open Fractures: Require surgical debridement and stable fixation to prevent infection and promote healing.
- Associated Neurovascular Injury: Fractures accompanied by compromise of the subclavian vessels or brachial plexus. While MIPO can be performed, careful direct visualization may be necessary for severe injuries, potentially requiring a more extensive approach.
- Threatened Skin Integrity: Sharp fracture fragments tenting the skin.
- Floating Shoulder: Ipsilateral clavicle fracture and scapular neck fracture, disrupting the superior shoulder suspensory complex.
- Nonunion or Symptomatic Malunion: Failed conservative treatment or symptomatic healing with deformity.
- Polytrauma Patient: When early mobilization and definitive fixation are critical for overall patient management.
- Patient Preference: For athletes requiring early return to high-demand activities, or individuals (e.g., female patients as highlighted in the seed content) prioritizing cosmetic outcomes and early functional recovery. MIPO specifically caters to this last group by minimizing scar burden and nerve irritation.
Contraindications for MIPO
While MIPO offers distinct advantages, certain scenarios may render it unsuitable or technically challenging:
- Active Local Infection: Any active infection in the surgical field is an absolute contraindication for elective hardware placement.
- Severe Local Soft Tissue Compromise: Extensive skin damage, blistering, or necrosis over the fracture site may preclude safe tunneling and incision placement.
- Extreme Comminution or Bone Loss: If there are too many small fragments or significant bone loss, achieving stable reduction and fixation with an indirect technique through small incisions may be difficult or impossible, necessitating direct visualization and potentially bone grafting.
- Obesity: Significant subcutaneous adipose tissue can make tunneling, reduction, and fluoroscopic visualization technically demanding.
- Severe Neurovascular Injury Requiring Direct Repair: If there is overt vascular compromise or brachial plexus transection, an open approach is mandated for direct visualization and repair.
- Lack of Surgeon Experience: The MIPO technique has a learning curve. Surgeons new to the technique should gain experience with simpler fractures or transition gradually from mini-open techniques.
- Certain Fracture Patterns: Medial clavicle fractures, or highly unstable lateral clavicle fractures requiring coracoclavicular ligament reconstruction or hook plates, may not be optimally managed with standard midshaft MIPO plating techniques.
Summary of Operative vs. Non-Operative Indications
| Feature | Non-Operative Treatment | Operative Treatment (MIPO/Open) |
|---|---|---|
| Indications |
- Nondisplaced/minimally displaced midshaft fractures (<2 cm shortening, <100% displacement)
- Pediatric fractures (<14 years) - High surgical risk patients - Contraindications to surgery |
- Displaced midshaft fractures (>2 cm shortening, >100% displacement)
- Multifragmentary/comminuted fractures - Open fractures - Neurovascular compromise (relative indication for MIPO, may require open) - Floating shoulder - Nonunion/symptomatic malunion - Polytrauma setting - Patient preference for early return to function or cosmetic outcome |
| Advantages |
- Avoids surgical risks
- No implant-related complications - No scar |
- Faster union rates
- Improved functional outcomes - Reduced malunion/nonunion rates - Better cosmetic outcomes (MIPO vs. open) - Early mobilization |
| Disadvantages |
- Higher risk of malunion/nonunion (adults)
- Potential for persistent pain/functional deficit - Longer immobilization - Poorer cosmetic outcome (deformity) |
- Surgical risks (infection, nerve injury, hardware failure)
- Scar formation (reduced with MIPO) - Potential for hardware removal |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning and meticulous patient positioning are crucial for successful MIPO of clavicle fractures.
Pre-Operative Planning
-
Imaging Review:
- Standard Radiographs: Anteroposterior (AP) view of the shoulder with 10-15 degrees of cephalic tilt, and a true AP clavicle view (0 degrees tilt) are essential. These provide initial assessment of fracture pattern, displacement, and shortening.
- Computed Tomography (CT) Scan: Highly recommended, especially for comminuted fractures, articular involvement (medial or lateral), or suspicion of neurovascular injury. A 3D reconstruction helps visualize fracture fragments, assess shortening and rotation, and plan plate trajectory.
-

-
Implant Selection:
- Choose a pre-contoured locking plate system specifically designed for the clavicle (e.g., superior, anterosuperior).
- Determine appropriate plate length to achieve adequate fixation (typically minimum 3-4 bicortical screws on each main fragment).
- Plan screw types (locking vs. non-locking) and lengths based on bone quality and desired stability.
-

-
Surgical Strategy:
- Visualize the reduction maneuver: Which arm movements (abduction, elevation, rotation) will best achieve length and alignment?
- Identify potential pitfalls: Difficult fragment manipulation, neurovascular structures at risk.
- Plan incision locations based on plate trajectory and fracture pattern.
- Prepare for potential conversion to a mini-open or full open approach if MIPO proves too challenging.
Patient Positioning
- Anesthesia: General endotracheal anesthesia is typically employed to ensure muscle relaxation and patient immobility for precise maneuvers.
-
Beach Chair Position:
The preferred position.
- The patient is placed in a semi-sitting "beach chair" position, similar to shoulder arthroscopy. This allows for excellent ergonomic access to the clavicle and facilitates C-arm fluoroscopy.
- The head is supported to permit flexion and extension, which can aid in relaxation of the sternocleidomastoid muscle.
-

- Scapular Padding: A padded bump or folded towel is placed under the ipsilateral scapula. As indicated in the seed content ("患侧肩胛骨处垫高,使肩部自然后张,以恢复锁骨长度"), this maneuver causes the shoulder to retract posteriorly and inferiorly, thereby restoring the anatomical length of the clavicle and facilitating reduction of displaced fragments.
-
Arm Draping:
The ipsilateral upper extremity is prepped and draped freely into the sterile field. This allows the surgeon or assistant to manipulate the arm (e.g., abduction, adduction, flexion, extension, rotation) intraoperatively to assist with fracture reduction, as highlighted in the seed content ("消毒范围包含患侧上肢并包手,以便术中调整患侧肩及上臂位置使骨折端易于复位").
-

-
- Sterile Field: A wide sterile field extending from the neck to the mid-chest and including the entire ipsilateral upper extremity is essential. This permits adequate working space and ensures sterility during arm manipulation.
- Fluoroscopy Access: The C-arm must be positioned to allow unobstructed AP and cephalic tilt views of the clavicle without repositioning the patient or contaminating the field.
Detailed Surgical Approach / Technique
The MIPO technique for clavicle fractures is a meticulous procedure requiring careful adherence to principles of indirect reduction and soft tissue preservation.
1. Incision Planning and Skin Marking
- Palpation and Marking: Carefully palpate the clavicle along its entire length, identifying the fracture site and the proposed course of the plate. Mark the skin corresponding to the ends of the selected plate, typically at the second screw hole from each end.
-
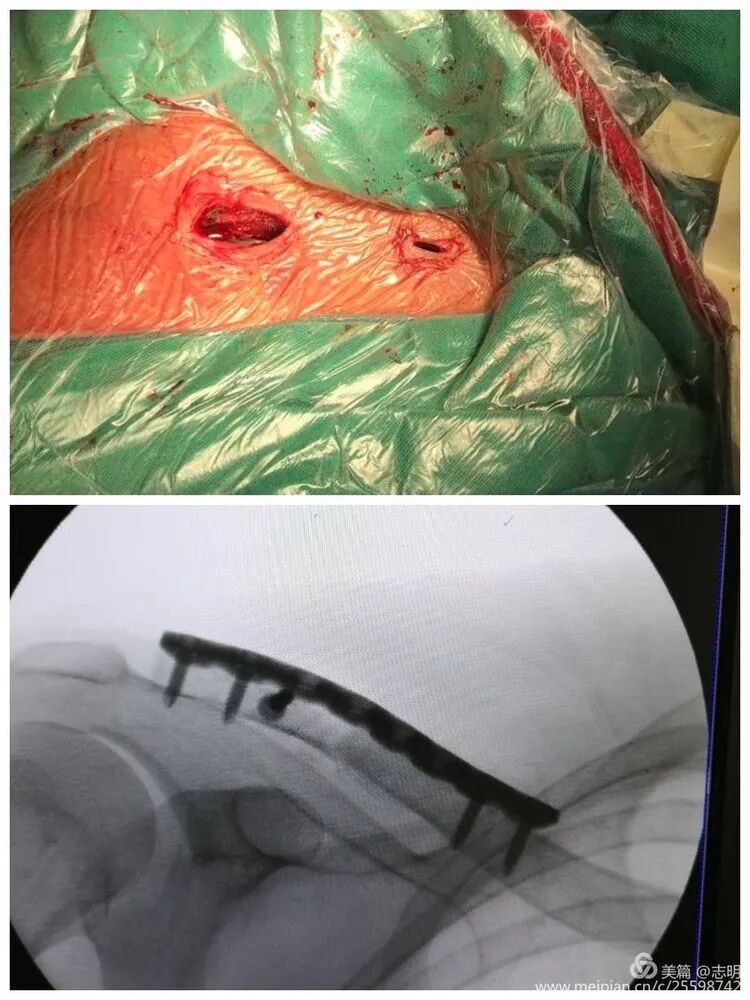
Small Incisions:
Make two small transverse or oblique incisions (approximately 1-2 cm each) directly over the marked points on the anterosuperior aspect of the clavicle. These incisions should be just large enough to allow screw insertion and passage of instruments. The choice of anterosuperior plating reduces prominence and potential irritation of supraclavicular nerves compared to purely superior plating.
-

-
2. Subcutaneous Tunnel Creation
- Dissection: Through each incision, meticulously dissect down to the clavicle, identifying and protecting the supraclavicular nerves. Blunt dissection is paramount.
-
Tunneling:
Using a specialized MIPO tunnelizer, a blunt periosteal elevator, or a curved clamp, create a subcutaneous tunnel over the superior aspect of the clavicle, connecting the two incisions. This tunnel should be just wide enough to accommodate the plate. The key is to stay submuscular to the platysma and directly on the superior surface of the clavicle, avoiding excessive periosteal stripping. This preserves the surrounding soft tissue envelope and its associated blood supply.
-
(This image shows a percutaneous tool, possibly for tunneling or reduction assistance).
-
3. Fracture Reduction
-
Indirect Maneuvers:
This is the most challenging step in MIPO. As mentioned in the seed content, "通过上抬肩部及调整上臂位置使断端初步复位" (By elevating the shoulder and adjusting the upper arm position, achieve preliminary reduction of the fracture fragments). The assistant manipulates the ipsilateral arm and shoulder to achieve length, alignment, and rotation of the clavicle.
- Length Restoration: Often achieved by abducting and extending the arm, with counter-traction from the assistant.
- Alignment: Adjusting shoulder position (retraction for posterior displacement, elevation for inferior displacement) helps align fragments.
- Rotation: Ensuring the natural anterior curvature of the clavicle is maintained.
-
Percutaneous Reduction Aids:
- Bone hooks, pointed reduction clamps, or small periosteal elevators can be inserted percutaneously through stab incisions to manipulate fragments under fluoroscopic guidance.
-

-
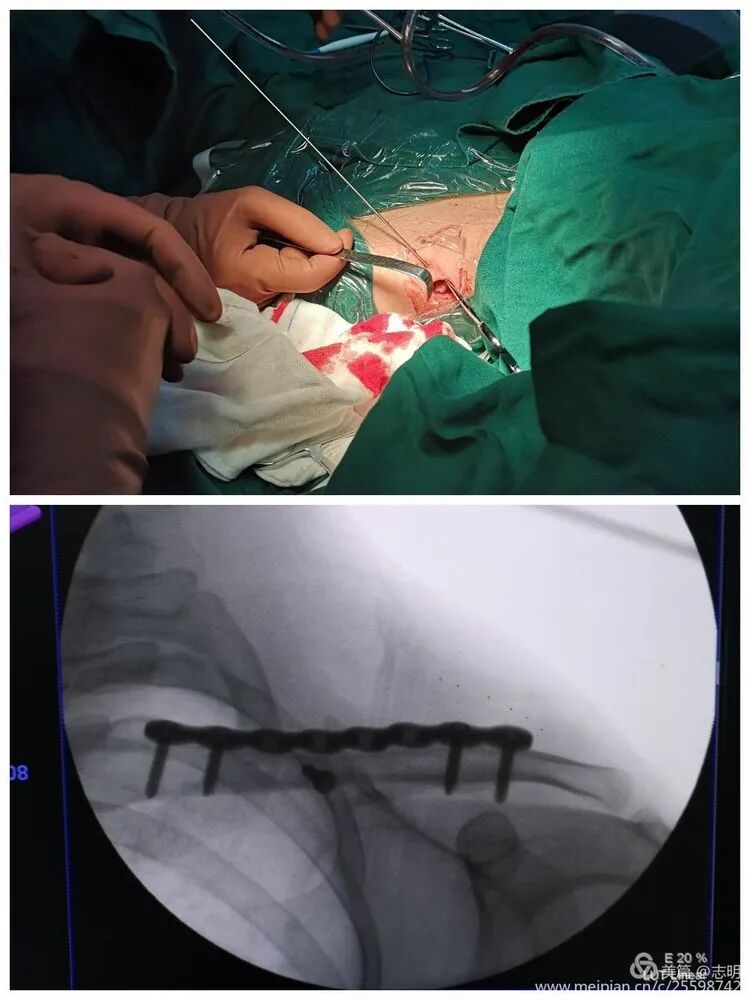
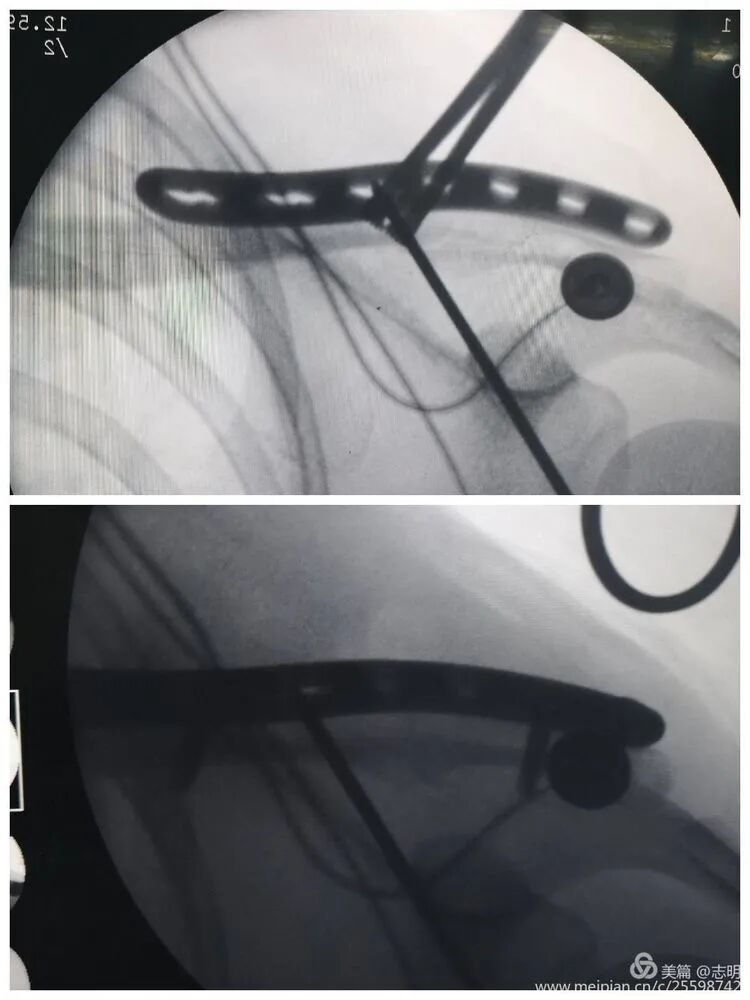
Temporary Fixation:
Once an acceptable reduction is achieved, maintain it with temporary percutaneous K-wires. As noted in the original text, "对于长斜形等易临时固定的骨折,可经皮钻入1.5mm克氏针维持复位" (For long oblique fractures and others easily temporarily fixed, 1.5mm Kirschner wires can be percutaneously drilled to maintain reduction). Ensure K-wires do not interfere with subsequent plate placement.
-
 -
(Fluoroscopy showing K-wire stabilization).
-
-
Fluoroscopic Guidance:
Continuous fluoroscopic imaging (AP and 30-45 degree cephalic tilt views) is essential throughout the reduction process to confirm alignment, length, and rotation.
-
 -
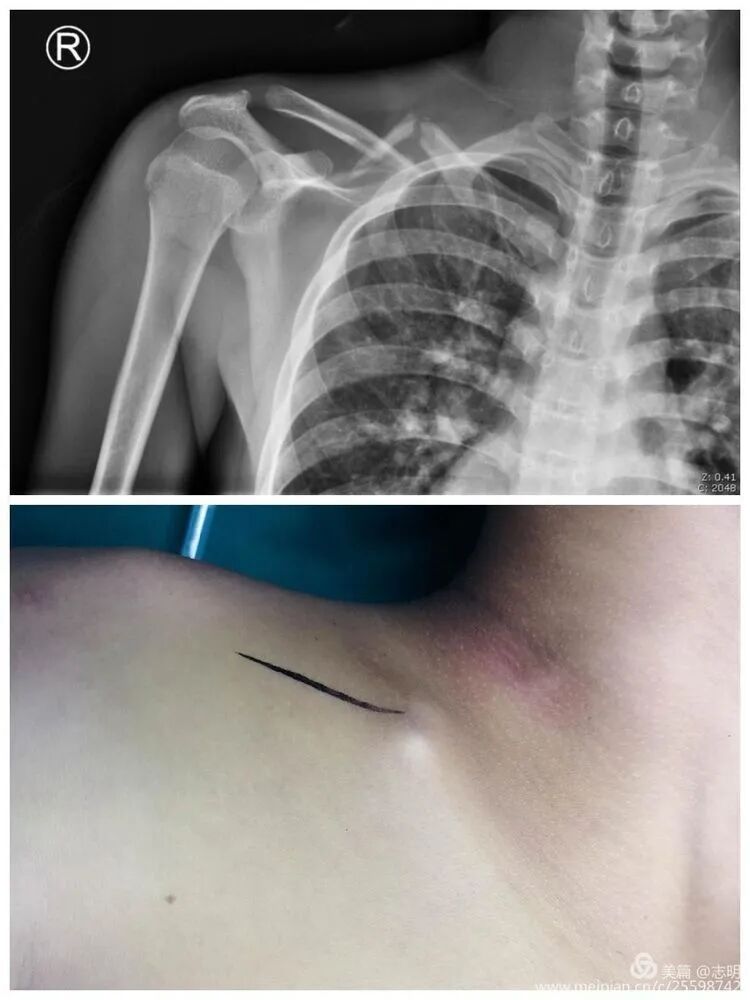
(X-ray showing pre-reduction fracture).
-
4. Plate Insertion and Fixation
-
Plate Passage:
Once reduction is satisfactory and temporarily stabilized, pass the pre-contoured locking plate through the subcutaneous tunnel. Use specialized plate manipulators to guide the plate and ensure it lies flush against the clavicle.
-
 -
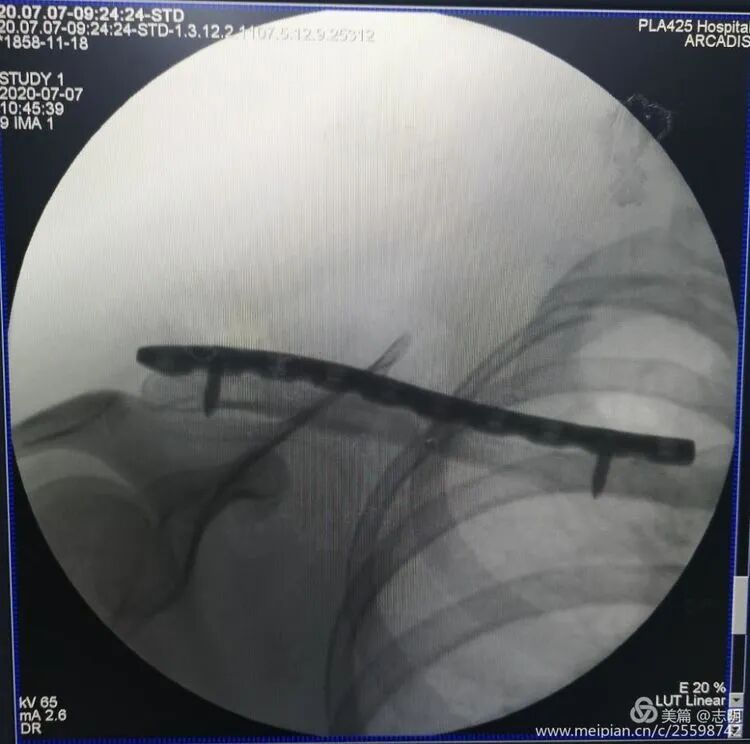
(Fluoroscopy confirming plate position). -
(Another fluoroscopy view of plate position).
-
-
Screw Insertion:
- Begin with drilling and inserting screws in the proximal and distal fragments through the small incisions. Use percutaneous drill guides and screw drivers.
- Carefully select screw length to achieve bicortical purchase while avoiding over-penetration, which could endanger underlying neurovascular structures. Fluoroscopy in both AP and lateral/cephalic tilt views is crucial for assessing screw trajectory and length.
- For highly comminuted fractures, locking screws are generally preferred to provide angular stability. For simpler patterns, an initial lag screw or compression screw (if the plate has dynamic compression units) can be used to optimize interfragmentary compression, followed by locking screws.
-
(Percutaneous drilling). -
(Fluoroscopy of screw insertion).
-
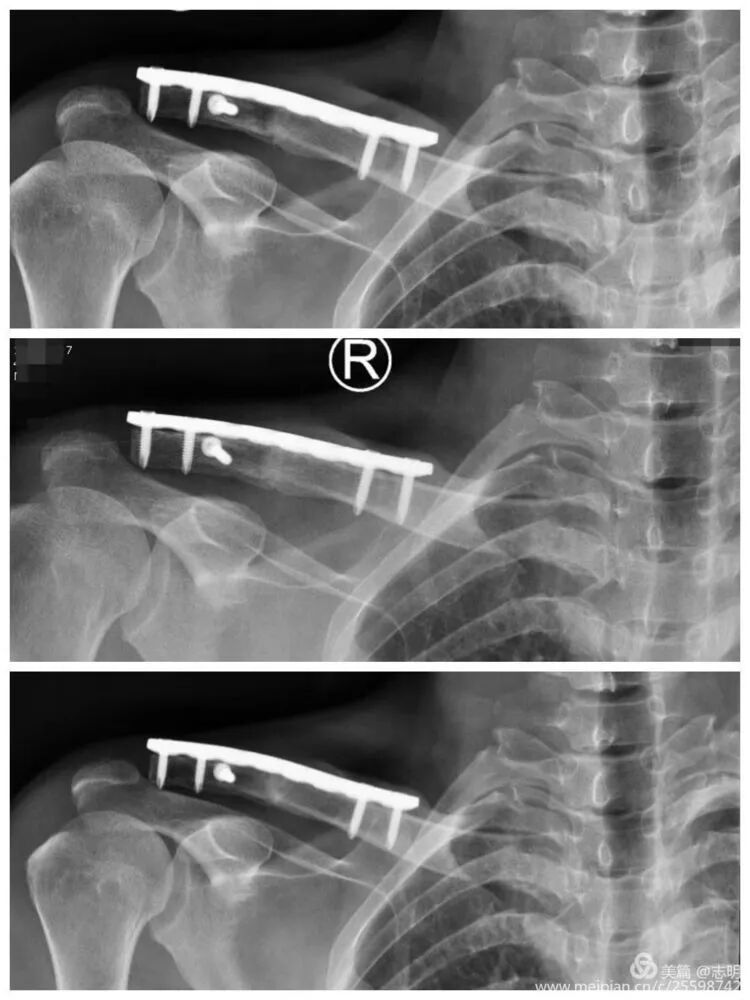
Final Assessment:
Once all screws are inserted, perform a final fluoroscopic assessment to confirm satisfactory fracture reduction, stable plate position, and appropriate screw lengths. Remove any temporary K-wires.
-
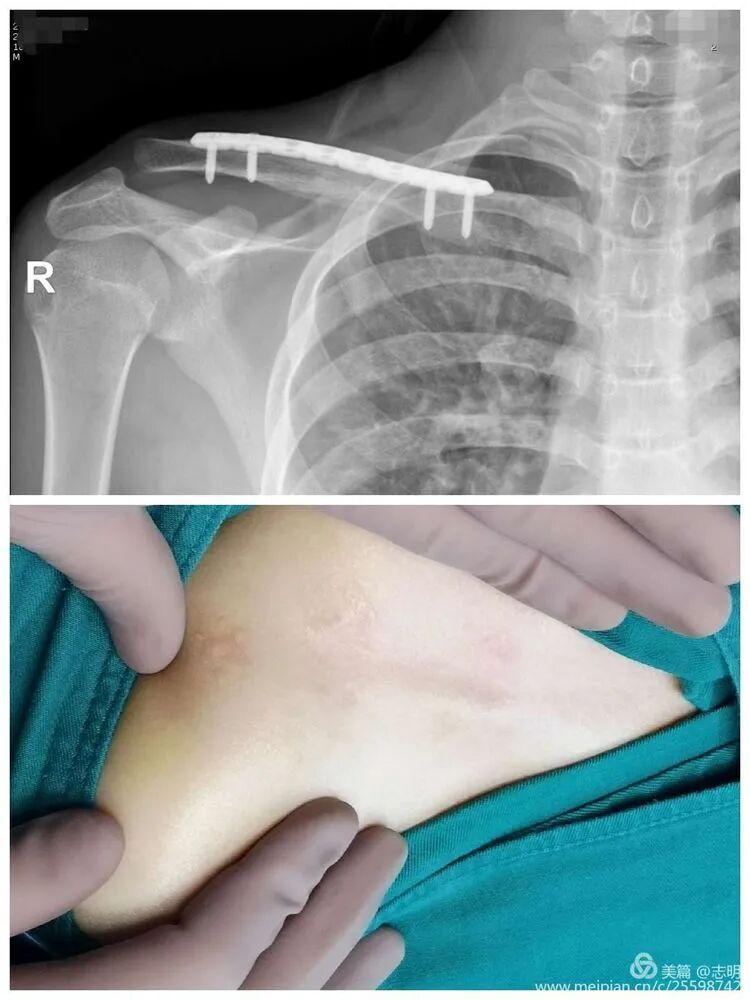(Post-fixation X-ray). -
(Healed fracture X-ray). -
(Another post-fixation X-ray).
-
5. Wound Closure
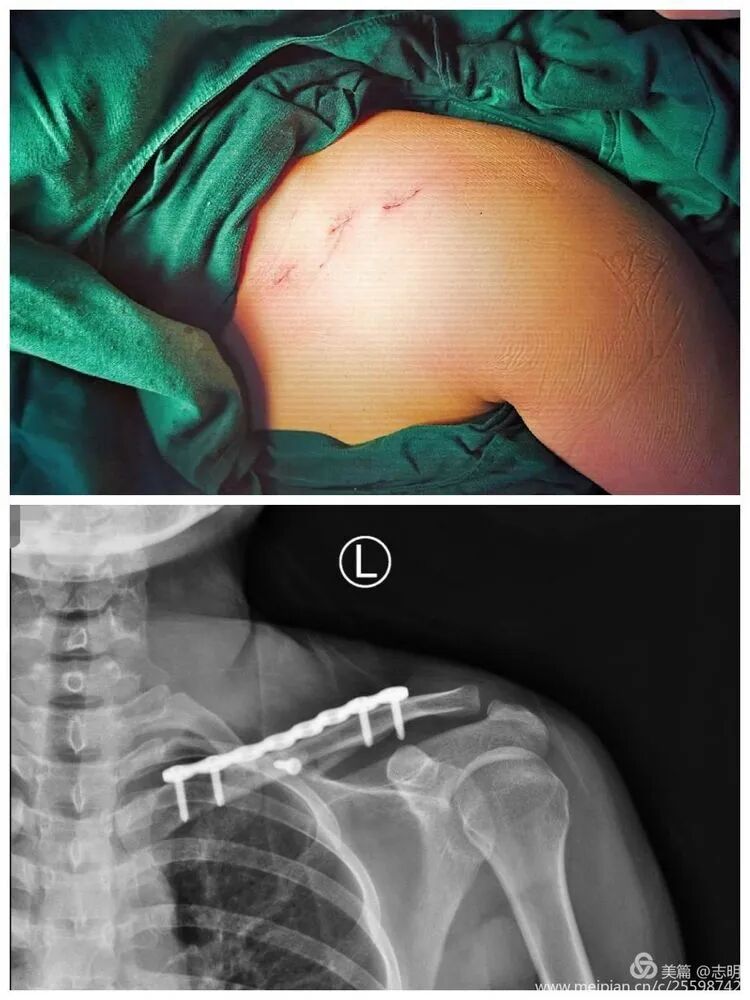
- Close the small skin incisions in layers. Ensure meticulous hemostasis.
-
The cosmetic outcome is significantly enhanced by these minimal incisions.
-
 -
 -
 -
-
Complications & Management
While MIPO for clavicle fractures offers significant advantages, it is not without potential complications. Awareness and proactive management are key to optimizing patient outcomes.
Common Complications and Management Strategies
| Complication | Incidence | Management Strategies ```
Clavicle Fractures: MIPO Microinvasive Technique - A Comprehensive Review for Surgeons
Introduction & Epidemiology
The clavicle, a superficial yet critical component of the shoulder girdle, is highly susceptible to fracture, accounting for 2-10% of all fractures and up to 45% of shoulder girdle injuries. Diaphyseal or midshaft clavicle fractures constitute the overwhelming majority, approximately 80%, of these occurrences. Historically, the management of most clavicle fractures leaned towards conservative measures, employing simple sling immobilization. This approach, while averting surgical risks, frequently resulted in undesirable sequelae such as malunion, symptomatic shortening, and aesthetic deformities, particularly in displaced adult fractures. Conversely, in the pediatric population, notably those under 14 years of age, the inherent robust potential for bone remodeling generally supports conservative treatment.
A significant shift in clinical practice has emerged from an enhanced understanding of the functional impairments attributable to substantial malunion (e.g., shortening exceeding 2 cm, >100% displacement) and the growing patient demand for expedited functional recovery and superior cosmetic outcomes. This has led to an increased propensity for operative intervention in displaced adult clavicle fractures. Traditional open reduction and internal fixation (ORIF) with plate and screw constructs, while offering robust stability and predictable union rates, inherently necessitates an extended incision along the subcutaneous border of the clavicle. This often precipitates conspicuous scarring and a considerable incidence of iatrogenic injury to the supraclavicular nerves, resulting in localized hypesthesia or dysesthesia, a common patient complaint, particularly among women.
The continuous evolution of surgical methodologies has introduced minimally invasive techniques to address these concerns. Minimally Invasive Plate Osteosynthesis (MIPO) for clavicle fractures, along with alternative approaches such as elastic intramedullary nailing, signifies a notable advancement. The core objective of MIPO is to achieve anatomical or near-anatomical fracture reduction and stable fixation via smaller incisions. This approach prioritizes the preservation of soft tissue integrity and periosteal blood supply, thereby fostering biological healing, minimizing scar burden, and reducing neurovascular complications in comparison to conventional ORIF. The following detailed discourse provides an exhaustive review of the technical intricacies and clinical considerations pertinent to clavicle MIPO, serving as an authoritative reference for orthopedic surgeons, residents, and medical students.
Surgical Anatomy & Biomechanics
A profound comprehension of clavicular anatomy and its biomechanical functions is foundational for successful MIPO of clavicle fractures. This knowledge is instrumental in guiding surgical technique, mitigating risks, and predicting outcomes.
Surgical Anatomy
The clavicle, an S-shaped long bone, serves as a crucial strut connecting the upper extremity to the axial skeleton. Its subcutaneous location renders it readily palpable but concurrently susceptible to direct trauma and postoperative hardware prominence.
- Morphology: The medial two-thirds of the clavicle exhibit an anterior convexity, while the lateral third demonstrates an anterior concavity. This characteristic S-shape is vital for its biomechanical attributes and articulatory functions.
-
Neurovascular Structures:
Meticulous attention to these structures is paramount for MIPO to minimize iatrogenic injury.
- Superiorly: The supraclavicular nerves—comprising medial, intermediate, and lateral branches originating from the cervical plexus—traverse the superior aspect of the clavicle. These nerves provide sensory innervation to the skin overlying the superior chest and shoulder. They are highly vulnerable to injury during initial incision, soft tissue dissection, and subcutaneous tunneling, which can lead to postoperative localized numbness or dysesthesia. MIPO's strategy of employing smaller incisions and blunt tunneling aims to significantly mitigate this specific risk.
- Posteriorly and Inferiorly: The subclavian artery and vein, alongside the brachial plexus, pass in close proximity, posterior and inferior to the clavicle. These vital neurovascular bundles are at considerable risk during deep drilling, aggressive tunneling, or excessive manipulation of displaced fracture fragments, particularly in highly comminuted patterns where sharp bone edges may impinge. The subclavius muscle, located within the subclavian groove on the inferior surface, provides a degree of protective cushioning.
-
Muscular Attachments:
The numerous muscular attachments exert substantial deforming forces on fracture fragments, influencing the pattern and extent of displacement, thereby complicating reduction maneuvers.
- Superior Attachments: The trapezius muscle attaches to the lateral third, while the sternocleidomastoid muscle attaches to the medial third. The sternocleidomastoid typically displaces the medial fragment superiorly.
- Inferior Attachments: The subclavius muscle occupies the subclavian groove in the middle third. The pectoralis major muscle attaches to the medial half, and the deltoid muscle attaches to the lateral half. The pectoralis major and deltoid, acting in concert, often displace the lateral fragment inferiorly and medially.
-
Ligaments:
- Medially: The sternoclavicular ligaments provide stability to the sternoclavicular joint.
- Laterally: The acromioclavicular ligaments stabilize the acromioclavicular joint.
- Coracoclavicular Ligaments: Comprising the conoid (medial) and trapezoid (lateral) ligaments, these robust structures connect the clavicle to the coracoid process of the scapula. They confer crucial vertical stability to the lateral clavicle, and their integrity is a critical consideration, especially in lateral third fractures.
- Periosteum: The clavicle's periosteum is a significant contributor to its intrinsic blood supply, which is indispensable for fracture healing. A cornerstone principle of MIPO is the limitation of soft tissue dissection to preserve this vital biological envelope, thereby enhancing the capacity for biological bone healing.
Biomechanics
The clavicle's primary biomechanical function is to act as a rigid strut, maintaining the length and integrity of the shoulder girdle. This structural role facilitates a maximal range of motion for the upper limb and provides essential protection for the underlying neurovascular structures.
- Stress Distribution: The inherent S-shape and robust cortical bone architecture enable the clavicle to effectively withstand considerable axial, bending, and torsional stresses. Midshaft fractures are most prevalent because this region represents the narrowest segment and coincides with a significant change in anatomical curvature, rendering it a stress riser.
- Fracture Displacement: As previously noted, the synergistic pull of the sternocleidomastoid muscle (elevating the medial fragment) and the combined forces of the pectoralis major and deltoid muscles (depressing and adducting the lateral fragment) typically result in superior displacement, angulation, and shortening of midshaft fracture fragments.
-
Fixation Principles:
- Relative Stability (MIPO): MIPO inherently promotes a biomechanical environment of relative stability, which encourages the formation of callus and secondary bone healing. By meticulously avoiding extensive periosteal stripping, the natural biological environment essential for healing is preserved. This approach contrasts with the pursuit of absolute stability, typically achieved by direct open reduction and compression plating, often indicated for simple transverse or short oblique fracture patterns.
-
Plate Positioning:
- Superior plating: Biomechanically, superior plating functions as a tension band, offering strong fixation. However, the superior surface of the clavicle is highly subcutaneous, increasing the likelihood of postoperative hardware prominence and irritation of the supraclavicular nerves.
- Anterosuperior plating: This position is frequently favored for MIPO. Placing the plate slightly anterior and superior, along the superior-anterior border, effectively reduces hardware prominence while maintaining adequate biomechanical stability. This trajectory may also necessitate less aggressive subperiosteal tunneling compared to a purely superior placement, potentially further minimizing nerve irritation. The judicious use of pre-contoured locking plates significantly facilitates effective and stable fixation in this preferred anatomical position.
MIPO strategically capitalizes on these biomechanical principles by achieving stable, yet biologically sympathetic, fixation. This allows for early postoperative mobilization while rigorously prioritizing tissue preservation and the biological processes essential for robust fracture healing, ultimately leading to superior functional and cosmetic outcomes.
Indications & Contraindications
The judicious decision to proceed with operative fixation, and specifically to employ the MIPO technique for clavicle fractures, hinges on a meticulous evaluation of numerous factors. These include patient-specific considerations, the precise characteristics of the fracture, and a thorough assessment of potential risks versus anticipated benefits.
Indications for Operative Treatment (including MIPO)
While conservative management remains a viable and appropriate option for many non-displaced or minimally displaced clavicle fractures, operative fixation is generally indicated for the following scenarios:
- Significant Displacement: Fractures with greater than one shaft width of displacement in transverse or oblique patterns, or superior/inferior displacement exceeding 10 mm, are strong indicators for surgical intervention.
- Clavicular Shortening: Shortening of the clavicle greater than 1.5-2 cm has been correlated with altered shoulder biomechanics, scapular dyskinesis, and resultant functional deficits.
- Severe Comminution: Multifragmentary fracture patterns where conservative treatment carries a high probability of leading to symptomatic malunion or nonunion.
- Open Fractures: These invariably require immediate surgical debridement and stable internal fixation to prevent deep infection and facilitate timely bone healing.
- Associated Neurovascular Injury: Fractures complicated by documented compromise of the subclavian vessels or brachial plexus warrant operative intervention. While MIPO can be cautiously employed, severe injuries may necessitate a more extensive open approach to allow direct visualization and repair.
- Threatened Skin Integrity: Sharp fracture fragments that are tenting or impending penetration of the overlying skin.
- Floating Shoulder: A severe injury characterized by concomitant ipsilateral clavicle and scapular neck fractures, effectively disrupting the entire superior shoulder suspensory complex.
- Established Nonunion or Symptomatic Malunion: Cases where conservative treatment has failed, or where healed fractures exhibit persistent pain, functional limitation, or significant deformity.
- Polytrauma Patient: In the context of multiple injuries, early definitive fixation of the clavicle fracture is often crucial for facilitating overall patient rehabilitation and management.
- Patient Preference: This is an increasingly relevant factor, particularly for athletes requiring an accelerated return to high-demand activities, or for individuals (e.g., female patients, as highlighted in the seed content) who prioritize optimal cosmetic outcomes and swift functional recovery. MIPO is uniquely positioned to address these specific patient demands by minimizing scar burden and reducing the incidence of iatrogenic nerve irritation.
Contraindications for MIPO
Despite the distinct advantages offered by MIPO, certain clinical scenarios may render the technique unsuitable or technically challenging:
- Active Local Infection: The presence of any active infection within the planned surgical field constitutes an absolute contraindication for elective implant placement.
- Severe Local Soft Tissue Compromise: Extensive skin damage, severe blistering, or necrotic tissue overlying the fracture site can preclude safe and effective subcutaneous tunneling and incision placement.
- Extreme Comminution or Significant Bone Loss: In situations with an excessive number of small, unstable fragments or substantial bone loss, achieving adequate indirect reduction and stable fixation through limited incisions can be exceedingly difficult or impossible, often necessitating direct visualization and potentially bone grafting.
- Significant Obesity: A thick subcutaneous adipose layer can render tunneling, indirect reduction maneuvers, and accurate fluoroscopic visualization technically demanding and significantly prolong operative time.
- Severe Neurovascular Injury Requiring Direct Repair: Overt vascular compromise (e.g., arterial transection) or documented brachial plexus transection necessitates an open surgical approach for direct visualization, exploration, and microvascular or microneural repair.
- Lack of Surgeon Experience: The MIPO technique, particularly in its indirect reduction aspects, has a notable learning curve. Surgeons new to the technique are advised to gain experience with less complex fracture patterns or to transition gradually from mini-open or traditional open approaches.
- Certain Fracture Patterns: Medial clavicle fractures, or highly unstable lateral clavicle fractures requiring specific implants like hook plates or direct coracoclavicular ligament reconstruction, may not be optimally managed with standard midshaft MIPO plating techniques.
Summary of Operative vs. Non-Operative Indications
| Feature | Non-Operative Treatment | Operative Treatment (MIPO/Open) |
|---|---|---|
| Indications |
- Nondisplaced/minimally displaced midshaft fractures (<2 cm shortening, <100% displacement)
- Pediatric fractures (<14 years) - High surgical risk patients - Contraindications to surgery |
- Displaced midshaft fractures (>2 cm shortening, >100% displacement)
- Multifragmentary/comminuted fractures - Open fractures - Neurovascular compromise (relative indication for MIPO, may require open) - Floating shoulder - Nonunion/symptomatic malunion - Polytrauma setting - Patient preference for early return to function or cosmetic outcome |
| Advantages |
- Avoids surgical risks
- No implant-related complications - No scar |
- Faster union rates
- Improved functional outcomes - Reduced malunion/nonunion rates - Better cosmetic outcomes (MIPO vs. open) - Early mobilization |
| Disadvantages |
- Higher risk of malunion/nonunion (adults)
- Potential for persistent pain/functional deficit - Longer immobilization - Poorer cosmetic outcome (deformity) |
- Surgical risks (infection, nerve injury, hardware failure)
- Scar formation (reduced with MIPO) - Potential for hardware removal |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are indispensable elements for ensuring the safe and successful execution of MIPO for clavicle fractures. These steps lay the groundwork for efficient intraoperative workflow and optimal clinical outcomes.
Pre-Operative Planning
-
Comprehensive Imaging Review:
- Standard Radiographs: Acquire high-quality anteroposterior (AP) views of the shoulder with a 10-15 degree cephalic tilt, along with a true AP clavicle view (0 degrees tilt). These projections are crucial for initial assessment of the fracture pattern, the degree and direction of displacement, and any significant shortening.
-
Computed Tomography (CT) Scan:
A CT scan, especially with 3D reconstructions, is highly recommended for comminuted fractures, fractures with suspected articular involvement (medial or lateral ends), or when neurovascular injury is a concern. The 3D reconstruction provides invaluable insights into fragment orientation, axial rotation, and the true extent of shortening, allowing for precise pre-operative templating of plate trajectory and screw placement.
-
(Example of pre-operative imaging, likely an X-ray showing fracture).
-
-
Implant Selection and Templating:
- Plate System: Select a pre-contoured locking plate system specifically designed for clavicle fixation (e.g., superior, anterosuperior plating systems). These plates are anatomically shaped to conform to the natural S-curve of the clavicle, minimizing the need for intraoperative contouring and reducing hardware prominence.
- Plate Length: Determine the appropriate plate length to ensure adequate fixation. A general principle is to achieve a minimum of 3-4 bicortical screws in each main fracture fragment, proximal and distal to the fracture site, to ensure stable construct integrity.
-
Screw Selection:
Plan the types of screws (locking vs. non-locking) and their anticipated lengths based on bone quality (assessed from imaging), fracture pattern (simple vs. comminuted), and the desired biomechanical environment (absolute vs. relative stability).
-
(Pre-contoured clavicle plate).
-
-
Surgical Strategy Development:
- Reduction Maneuvers: Visualize the specific indirect reduction maneuvers required. This includes anticipating which arm and shoulder movements (e.g., abduction, elevation, external rotation, retraction) will best restore clavicle length, alignment, and rotation.
- Potential Challenges: Identify potential intraoperative difficulties, such as particularly recalcitrant fragment manipulation, proximity to critical neurovascular structures, or limitations of fluoroscopic imaging.
- Incision Planning: Precisely plan the locations and orientations of the small skin incisions based on the chosen plate trajectory and fracture morphology.
- Contingency Plan: Always prepare for the possibility of converting to a mini-open or full open approach if MIPO techniques prove technically insurmountable or compromise patient safety.
Patient Positioning
- Anesthesia: General endotracheal anesthesia is the standard. It provides complete muscle relaxation, critical for achieving and maintaining fracture reduction, and ensures patient immobility throughout the delicate procedure.
-
Beach Chair Position:
This semi-sitting position is the universally preferred choice for clavicle MIPO.
- It offers optimal ergonomic access to the clavicle and facilitates unhindered manipulation of the C-arm for fluoroscopic imaging.
- The patient's head is carefully supported to allow for flexion and extension, which can aid in relaxation of the sternocleidomastoid muscle, thereby contributing to easier reduction of the medial fragment.
-
(Image showing patient preparation with clavicle marked and padding).
- Scapular Padding: A firm, padded bump or a series of folded towels is strategically placed beneath the ipsilateral scapula. As explicitly stated in the seed content, this maneuver "患侧肩胛骨处垫高,使肩部自然后张,以恢复锁骨长度" (elevates the ipsilateral scapula, causing the shoulder to naturally retract, thereby restoring clavicle length). This posterior and inferior retraction of the shoulder girdle is crucial for restoring the anatomical length of the clavicle and facilitating the reduction of displaced fragments.
-
Arm Draping:
The entire ipsilateral upper extremity is meticulously prepped and draped freely into the sterile field. This critical step permits dynamic intraoperative manipulation of the arm (e.g., abduction, adduction, flexion, extension, rotation) by the surgeon or an assistant, which is often indispensable for achieving and confirming fracture reduction. The seed content emphasizes this: "消毒范围包含患侧上肢并包手,以便术中调整患侧肩及上臂位置使骨折端易于复位" (The sterile field includes the ipsilateral upper extremity and hand, allowing for intraoperative adjustment of the ipsilateral shoulder and upper arm position to facilitate fracture fragment reduction).
-
(Image showing the sterile draping including the arm).
-
- Sterile Field and Fluoroscopy Access: A broad sterile field extending from the neck to the mid-chest, encompassing the entire ipsilateral upper extremity, is imperative. This generous field provides ample working space and ensures sterility during necessary arm manipulations. The C-arm fluoroscopy unit must be strategically positioned to allow unhindered acquisition of both AP and 30-45 degree cephalic tilt views of the clavicle without the need for patient repositioning or compromising the sterile field. This ensures continuous real-time radiographic assessment throughout the procedure.
Detailed Surgical Approach / Technique
The MIPO technique for clavicle fractures is a sophisticated procedure that demands precision, a nuanced understanding of indirect reduction maneuvers, and a steadfast commitment to soft tissue preservation.
1. Incision Planning and Skin Marking
- Palpation and Clavicle Outline: Begin by thoroughly palpating the entire length of the clavicle, meticulously identifying the precise fracture site and the anticipated course of the chosen plate. Mark the overlying skin to delineate the clavicular outline.
-
Incision Placement:
Based on the pre-operative templating, mark the skin for two small incisions, typically positioned over the second screw hole from each end of the selected plate. These incisions, approximately 1-2 cm in length, are usually oriented transversely or obliquely on the anterosuperior aspect of the clavicle. The chosen anterosuperior plate trajectory is preferred over a purely superior one to mitigate hardware prominence and minimize the risk of irritation to the supraclavicular nerves. Ensure the incisions are just sufficient to accommodate screw insertion and the passage of necessary instruments.
-
(Image showing plate used for surface marking to define incision points).
-
2. Subcutaneous Tunnel Creation
- Initial Dissection: Through each planned incision, carefully dissect down to the clavicle using blunt techniques, primarily. It is paramount to identify and meticulously protect the branches of the supraclavicular nerves within the subcutaneous tissue. Subplatysmal dissection is typically maintained.
-
Tunneling Technique:
A specialized MIPO tunnelizer, a blunt periosteal elevator, or a curved clamp is used to create a subcutaneous tunnel directly over the superior aspect of the clavicle, connecting the two incisions. The tunnel should be precisely wide enough to allow the unimpeded passage of the plate. The fundamental principle here is to remain directly on the superior cortical surface of the clavicle while avoiding any unnecessary or extensive periosteal stripping. This critical step preserves the vital surrounding soft tissue envelope and its associated blood supply, which is crucial for promoting robust biological fracture healing.
-
(Image likely illustrating an instrument used for tunneling or manipulating fragments percutaneously).
-
3. Fracture Reduction
-
Indirect Reduction Maneuvers:
This stage is often the most technically demanding aspect of MIPO. As articulated in the original content, "通过上抬肩部及调整上臂位置使断端初步复位" (By elevating the shoulder and adjusting the upper arm position, achieve preliminary reduction of the fracture fragments). The assistant plays a crucial role by dynamically manipulating the ipsilateral arm and shoulder to restore the clavicle's anatomical length, achieve proper alignment, and correct any rotational deformity.
- Length Restoration: Typically achieved by a combination of arm abduction and extension, often with an element of traction, while an assistant provides counter-traction at the axilla or chest wall.
- Alignment Correction: Adjusting the shoulder's position (e.g., posterior retraction for anterior displacement, superior elevation for inferior sag) helps to align the fracture fragments in both sagittal and coronal planes.
- Rotation Control: Ensuring that the natural anterior curvature of the clavicle is maintained, avoiding malrotation.
-
Percutaneous Reduction Aids:
Various instruments can be employed percutaneously through small stab incisions to aid in reduction under fluoroscopic guidance. These include bone hooks, pointed reduction clamps, or small periosteal elevators. These tools allow for direct manipulation of fragments without extensive soft tissue exposure.
-
(Clinical image showing surgeon's hands manipulating the shoulder, likely assisting in reduction).
-
-
Temporary Fixation:
Once a satisfactory reduction is achieved, it must be temporarily secured prior to plate application. Percutaneous Kirschner wires (K-wires) are commonly used for this purpose. The seed content states: "对于长斜形等易临时固定的骨折,可经皮钻入1.5mm克氏针维持复位" (For long oblique fractures and others easily temporarily fixed, 1.5mm Kirschner wires can be percutaneously drilled to maintain reduction). Ensure that the K-wires are placed in a manner that does not impede subsequent plate placement or screw trajectory.
-
(X-ray showing temporary K-wire fixation after reduction). -
(Fluoroscopic image demonstrating K-wire placement for temporary reduction).
-
-
Fluoroscopic Guidance:
Continuous, high-quality fluoroscopic imaging is absolutely essential throughout the entire reduction process. Both AP and 30-45 degree cephalic tilt views must be utilized to confirm accurate length restoration, anatomical alignment, and correct rotational profile.
-
(Initial fluoroscopic view of the fracture). -
(Another pre-reduction X-ray).
-
4. Plate Insertion and Screw Fixation
-
Plate Passage:
Once the fracture reduction is deemed satisfactory and secured with temporary fixation, the pre-contoured locking plate is carefully passed through the previously created subcutaneous tunnel. Specialized plate manipulators and guides are used to ensure the plate lies snugly and flush against the superior or anterosuperior cortical surface of the clavicle.
-
(Image depicting the insertion of a plate through a small incision). -
(Fluoroscopic image confirming proper plate positioning). -
(Another fluoroscopic view illustrating the plate's final position).
-
-
Screw Insertion:
- Begin by drilling and inserting screws in both the proximal and distal main fracture fragments through the small skin incisions. Utilize percutaneous drill guides and specialized screw drivers designed for MIPO techniques.
- Screw Length and Trajectory: Exercise extreme caution when selecting screw length to ensure adequate bicortical purchase without over-penetration, which carries a significant risk of damaging underlying neurovascular structures. Fluoroscopy, again in both AP and lateral/cephalic tilt views, is paramount for real-time assessment of screw trajectory and length.
- Screw Type and Sequence: For comminuted fractures, locking screws are generally preferred to provide angular stability and maintain reduction indirectly. In simpler fracture patterns, an initial lag screw or a compression screw (if the plate design permits dynamic compression) can be employed to achieve optimal interfragmentary compression, followed by the insertion of locking screws to complete the construct.
-
(Image showing percutaneous drilling through a guide). -
(Fluoroscopic image depicting screw insertion).
-
Final Intraoperative Assessment:
Once all screws are securely inserted, perform a comprehensive final fluoroscopic assessment. Verify satisfactory fracture reduction, confirm stable and flush plate position, and ensure appropriate screw lengths and trajectories. Any temporary K-wires are then removed.
-
(Post-fixation X-ray showing the plate and screws in place). -
(Another post-fixation X-ray).
-
5. Wound Closure
- Close the small skin incisions in a layered fashion. Ensure meticulous hemostasis to prevent hematoma formation, which can compromise the cosmetic outcome and increase infection risk.
-
The primary cosmetic advantage of MIPO derives from these minimal incisions, resulting in significantly less visible scarring.
-
(Clinical image of small, well-healed MIPO incisions). -
(Another clinical view of minimal scarring). -
(Close-up of a small post-operative incision). -
(Clinical view of small post-operative incisions). -
(Clinical image demonstrating good range of motion post-operatively).
-
Complications & Management
While MIPO for clavicle fractures offers several advantages, it is imperative for orthopedic surgeons to be acutely aware of potential complications. Proactive recognition, prevention strategies, and appropriate management are crucial for optimizing patient outcomes.
Common Complications and Management Strategies
| Complication | Incidence | Management Strategies |
|
Neurovascular Injury
| <1% (severe); Supraclavicular nerve ~10-40% (sensory deficits) |
Prevention:
Meticulous surgical technique, blunt tunneling, careful drilling, and fluoroscopic guidance (especially for anterior/posterior screw depth).
Management:
Sensory deficits are often temporary and managed with observation; persistent or painful deficits may warrant neurophysiological evaluation and consideration of surgical exploration/neurolysis. Vascular injuries are surgical emergencies requiring immediate repair. |
|
Infection
| 1-5% (superficial or deep) |
Prevention:
Strict aseptic technique, appropriate perioperative prophylactic antibiotics.
Management:
Superficial infections typically respond to local wound care and oral antibiotics. Deep infections necessitate surgical debridement, intravenous antibiotic therapy, and potentially hardware removal (once union is achieved) or retention with long-term suppressive therapy if fixation is critical. |
|
Nonunion
| 2-10% (lower than non-operative for displaced fractures) |
Prevention:
Stable fixation, meticulous surgical technique, preservation of periosteal blood supply (MIPO advantage), appropriate patient selection.
Management:
Revision surgery, often involving open reduction, debridement of fibrous tissue, bone grafting (autograft or allograft), and a stiffer, longer fixation construct. Biological augmentation may be considered. |
|
Malunion
| <5% (symptomatic) |
Prevention:
Accurate intraoperative reduction (achieved through indirect maneuvers and fluoroscopy) and stable fixation.
Management:
Asymptomatic malunions are managed with observation. Symptomatic malunions, particularly those causing pain or functional impairment, may require corrective osteotomy and refixation. |
|
Hardware Prominence/Irritation
| 10-30% |
Prevention:
Use of low-profile, anatomically contoured plates (e.g., anterosuperior position), careful surgical technique to ensure the plate lies flush.
Management:
This is a common indication for elective hardware removal, typically performed 12-18 months post-operatively, after complete fracture healing is confirmed. |
|
Hardware Failure
| <5% |
Prevention:
Selection of appropriate plate length and strength, adequate screw purchase (bicortical), stable initial reduction, and patient adherence to post-operative weight-bearing restrictions.
Management:
Revision surgery is required, often utilizing a larger or stronger plate, a different construct (e.g., dual plating), and addressing any underlying issues contributing to failure. |
|
Pneumothorax
| Rare (<0.1%) |
Prevention:
Extreme caution during drilling and instrumentation, particularly when working inferiorly or medially near the sternoclavicular joint. Avoid deep penetration beyond the posterior cortex.
Management:
Immediate recognition, often by intraoperative auscultation or post-operative chest X-ray. Typically managed with chest tube insertion and observation until lung re-expansion. |
|
Refracture
| 1-5% (after hardware removal) |
Prevention:
Ensuring complete radiographic and clinical fracture healing prior to hardware removal. Gradual, progressive return to full activity following implant removal.
Management:
Requires refixation, often with a longer and stronger plate, treating it as a new fracture with consideration for bone grafting. |
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is integral to achieving optimal functional outcomes following MIPO for clavicle fractures. The protocol aims to protect the operative fixation, promote robust bone healing, prevent shoulder stiffness, and gradually restore full strength and range of motion.
Phases of Rehabilitation
Phase 1: Immediate Post-Operative Protection (Weeks 0-2/4)
- Goals: Protect the surgical repair, manage pain and swelling, initiate early hand/wrist/elbow motion.
-
Immobilization:
- The arm is typically immobilized in a sling for comfort and protection. The duration of sling use varies based on fracture stability, patient compliance, and surgeon preference (commonly 2-4 weeks). Strict avoidance of active shoulder movement is usually advised.
-
Pain Management:
- Utilize multimodal analgesia (NSAIDs, acetaminophen, opioids as needed) to control post-operative pain and facilitate early, gentle movement.
-
Early Motion:
- Hand, Wrist, Elbow: Encourage active range of motion (AROM) exercises for the hand, wrist, and elbow to prevent stiffness and maintain circulation.
- Shoulder: Gentle passive pendulum exercises for the shoulder may be initiated as pain allows, ensuring no active muscle contraction around the clavicle.
-
Activity Restrictions:
- Absolutely no active shoulder elevation, abduction, or external rotation beyond neutral.
- Strict avoidance of lifting, pushing, pulling, or any activities that could place stress on the healing clavicle.
- No weight-bearing on the affected arm.
Phase 2: Early Mobilization (Weeks 2/4 - 6/8)
- Goals: Gradually restore active shoulder range of motion, maintain soft tissue mobility, initiate early scapular stabilization.
- Sling Weaning: The sling is gradually weaned as comfort improves and radiographic signs of early healing appear. It may be used for protection in crowded environments.
-
Active-Assisted Range of Motion (AAROM):
- Initiate gentle active-assisted range of motion (AAROM) exercises for shoulder flexion and abduction, typically progressing up to 90 degrees as tolerated. These can involve a cane, pulley system, or assistance from the contralateral arm.
- External and internal rotation are also progressively introduced within pain-free limits.
-
Scapular Stabilization:
- Begin isometric exercises for scapular retractors (e.g., gentle shoulder blade squeezes) to restore proprioception and muscular control without stressing the fracture.
-
Activity Progression:
- Light activities of daily living (ADLs) are permitted within the prescribed range of motion.
- Continued avoidance of heavy lifting, overhead activities, and direct pressure on the clavicle.
Phase 3: Progressive Strengthening (Weeks 6/8 - 12/16)
- Goals: Achieve full active range of motion, initiate progressive strengthening, prepare for return to more demanding activities.
-
Full AROM:
- Aim for full active shoulder range of motion in all planes.
-
Strengthening:
- Progressive strengthening exercises for the entire shoulder girdle musculature are introduced. This includes rotator cuff strengthening (internal/external rotation with light resistance), deltoid strengthening (flexion, abduction), and advanced scapular stabilization exercises.
- Light resistance training (e.g., resistance bands, light weights) is initiated, gradually increasing intensity.
-
Activity Progression:
- Cautiously begin overhead activities and functional tasks.
- Radiographic assessment of fracture healing is typically performed around 8-12 weeks to guide further progression. Clinical union should be evident.
Phase 4: Return to Activity (Weeks 12/16+)
- Goals: Advanced strengthening, sport-specific training, safe return to unrestricted activities.
-
Advanced Training:
- Continue with advanced strengthening exercises, focusing on power, endurance, and sport-specific movements (if applicable).
- Proprioceptive training and plyometrics may be incorporated for athletes.
-
Return to Activity:
- Gradual return to unrestricted activities, including contact sports or heavy labor, is permitted only after achieving complete clinical and radiographic evidence of robust fracture union.
- The decision for return to contact sports or high-impact activities should typically be delayed until 4-6 months post-operatively, after thorough clinical and radiographic assessment.
-
Hardware Removal:
- Discussion regarding elective hardware removal (typically 12-18 months post-operatively) should occur once the fracture is fully consolidated and mature. Risks and benefits of removal, including potential refracture, should be thoroughly reviewed with the patient.
Throughout all phases, individual patient response, pain levels, and radiographic healing must dictate the pace of progression. Close communication between the surgeon, physical therapist, and patient is essential for a safe and effective rehabilitation journey.
Summary of Key Literature / Guidelines
The landscape of clavicle fracture management has evolved significantly, particularly with the increasing adoption of operative techniques. MIPO represents a refinement within this operative paradigm, aiming to optimize patient-centered outcomes. A robust body of literature now supports the efficacy and benefits of MIPO for select clavicle fractures.
Evolution of Operative Indications
Early Level I randomized controlled trials (RCTs) such as the Canadian Orthopaedic Trauma Society (COTS) study (2007) provided strong evidence for operative fixation of significantly displaced midshaft clavicle fractures in adults. These studies demonstrated superior union rates, lower rates of symptomatic malunion and nonunion, and improved functional outcomes (e.g., DASH scores) compared to non-operative treatment for these specific fracture types. This evidence solidified the role of surgical intervention, primarily with plate fixation, for displaced fractures.
MIPO vs. Open Plating: Comparative Outcomes
With the established efficacy of operative fixation, the focus shifted to refining surgical techniques. MIPO emerged as an alternative to traditional ORIF, specifically addressing concerns regarding large scars and iatrogenic supraclavicular nerve injury.
- Comparable Efficacy: Numerous comparative studies, including meta-analyses, have consistently shown that MIPO techniques for midshaft clavicle fractures yield union rates and functional outcomes (e.g., Constant score, DASH score) that are comparable to, if not slightly superior to, those achieved with conventional open plating. There is no evidence suggesting MIPO compromises fracture healing.
-
Cosmetic and Neurological Advantages:
The primary advantages of MIPO lie in its minimally invasive nature:
- Reduced Scar Burden: MIPO utilizes smaller, typically two, short incisions, resulting in significantly less conspicuous scarring. This is a considerable cosmetic benefit, particularly important for patients sensitive to body image.
- Lower Incidence of Supraclavicular Nerve Injury: By limiting soft tissue dissection and utilizing blunt tunneling techniques, MIPO demonstrably reduces the incidence of iatrogenic injury to the supraclavicular nerves. Studies have reported lower rates of sensory deficits and dysesthesia with MIPO compared to traditional open approaches, where extensive subplatysmal dissection is often required to expose the entire clavicle. The preservation of the nerve branches minimizes post-operative numbness, a common complaint after ORIF.
- Biological Healing: The principle of indirect reduction and limited soft tissue stripping inherent in MIPO preserves the periosteal blood supply to the fracture fragments. This biological advantage is hypothesized to promote more robust and rapid bone healing by enhancing the local healing environment, although direct clinical quantification of this benefit over ORIF remains challenging in large-scale comparative studies.
- Surgical Challenges and Learning Curve: While advantageous, MIPO presents a steeper learning curve than open plating. The indirect reduction maneuvers, percutaneous instrument manipulation, and reliance on fluoroscopy require significant surgical skill and experience. Difficult cases, such as highly comminuted or multi-planar displaced fractures, may increase operative time or necessitate conversion to a mini-open or traditional open technique if adequate reduction cannot be achieved indirectly.
Role of Plate Design
The evolution of plate design, particularly the advent of pre-contoured locking plates, has been instrumental in facilitating MIPO techniques. These plates are anatomically shaped to fit the clavicle's S-curve, minimizing the need for intraoperative bending and reducing the risk of hardware prominence. Locking plates provide angular stability, which is highly beneficial for indirect reduction techniques as it allows for stable fixation even with comminuted patterns, effectively creating a "fixed-angle construct." The choice between superior and anterosuperior plating in MIPO often favors the anterosuperior position to further minimize hardware prominence and nerve irritation without compromising biomechanical stability.
Current Guidelines and Recommendations
Current consensus and evolving guidelines advocate for individualized treatment of clavicle fractures. For significantly displaced midshaft clavicle fractures in adults, operative fixation is generally recommended to optimize functional and radiographic outcomes. Within the operative spectrum, MIPO techniques are increasingly recognized as a valuable option, particularly for patients who prioritize aesthetic outcomes and seek to minimize postoperative sensory disturbances, provided the surgeon possesses the requisite experience and the fracture pattern is amenable to indirect reduction.
In summary, MIPO for clavicle fractures offers a sophisticated, tissue-sparing approach that provides comparable union rates and functional outcomes to traditional open methods, coupled with superior cosmetic results and a reduced incidence of supraclavicular nerve morbidity. Its successful application hinges on thorough pre-operative planning, meticulous surgical technique, and a comprehensive understanding of clavicular anatomy and biomechanics. As an academic orthopedic surgeon, I advocate for its judicious application as a preferred technique in appropriate clinical scenarios.
